CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF MILD HEAD INJURY (MHI) IN ADULTS
| Site: | EHC | Egyptian Health Council |
| Course: | Emergency Medicine Guidelines |
| Book: | CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF MILD HEAD INJURY (MHI) IN ADULTS |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:55 AM |
Description
"last update: 4 Jan 2026" Download Guideline
- Executive Summary
These recommendations promote selective CT imaging and safe disposition in adult mild head injury, and standardizing care with clear admission/discharge criteria.
|
No. |
Recommendations |
Strength of recommendation |
|
1. |
We recommend the Canadian CT Head Rule (CCHR) to guide CT use in adults with mild head injury not on anticoagulants or antiplatelets, to minimize unnecessary imaging. If CT imaging is not available, refer to an appropriate facility. CT is indicated if any of the following are present: · Failure to reach a GCS score of 15 within 2 hours of injury. · Suspected open skull fracture. · Signs of basal skull fracture. · Vomiting more than once. · Age > 64 years. The Canadian CT Head Rule (CCHR) is not applicable to patients younger than 16 years, those receiving anticoagulant therapy (blood thinners), or patients who experience a post-traumatic seizure. |
Strong |
|
2. |
We recommend performing a non-contrast head CT in patients over 60 years old who are present with loss of consciousness or post traumatic amnesia. If CT imaging is not available, refer to an appropriate facility. |
Strong |
|
3. |
We recommend performing a non-contrast head CT in intoxicated patients with mild head trauma who present with loss of consciousness or posttraumatic amnesia. If CT imaging is not available, refer to an appropriate facility. |
Strong |
|
4. |
We recommend performing a non-contrast head CT in anticoagulated patients with mild head injury, rather than relying solely on clinical decision tools to exclude imaging. If CT imaging is not available, refer to an appropriate facility. |
Strong |
|
5. |
We advise against routine repeating a non-contrast head CT in adults with mild head injury on anticoagulants or antiplatelets who remain at baseline neurologic assessment, if the initial CT is negative for hemorrhage. |
Conditional |
|
6. |
We recommend admitting patients with mild head injury to hospital if clinical assessment identifies any risk factors or concerning features that warrant close observation or further management. Admission is advised when one or more of the established admission criteria for mild head injury are present: · New, clinically important abnormalities on imaging (An isolated simple linear non-displaced skull fracture is unlikely to be clinically important unless the patient is taking anticoagulant or antiplatelet medication.) · GCS score did not return to 15 (or pre-injury baseline) after imaging, regardless of the imaging results. · Indications for CT scanning are present, but scanning cannot be performed within the appropriate time period, either because CT is unavailable or because the person is not sufficiently cooperative to allow scanning. · Continuing worrying symptoms of concern to the clinician, such as persistent vomiting, severe headaches, or seizures. · Other sources of clinician concern, including but not limited to drug or alcohol intoxication, other injuries, shock, suspected non-accidental injury, meningism, cerebrospinal fluid leak, or suspicion of ongoing post-traumatic amnesia. |
Good Practice Statement |
|
7. |
We recommend discharging patients with mild head injury when clinical assessment and investigations identify no evidence of clinically important brain or cervical spine injury, provided that: · CT scan of the head and/or cervical spine is not indicated or has shown normal findings, and the Glasgow Coma Scale (GCS) has returned to 15 or the pre-injury baseline. · There are no other factors that would warrant hospital admission. (refer to recommendation number 6) · There is appropriate supervision at home or a suitable environment for continued observation in the community. |
Good Practice Statement |
|
8. |
We advise against routine hospital admission in anticoagulated or antiplatelet-treated patients with mild head injury who have a normal neurological exam, a normal initial CT, and lack criteria warranting extended monitoring. The criteria warranting extended monitoring and hospital admission are the same as those for patients who are not taking anticoagulant or antiplatelet therapy. |
Conditional |
|
9. |
We recommend providing written discharge instructions outlining red-flag symptoms and follow-up guidance to adults with mild head injury to improve early recognition of complications. A. Discharge instructions should include advice to: · Avoid activities that may increase the risk of recurrent head injury. · Maintain social contact and communicate with family or friends about recovery symptoms. · Use only medications approved by the treating physician for symptom control. · Limit screen time and exposure to loud noise before sleep, keep a consistent sleep schedule, and rest in a quiet, dark environment. B. Inform a trusted person about the injury and the warning signs to monitor for, as they may recognize symptoms before the patient does. C. Arrange a follow-up visit within 48 hours of discharge. On discharge you should inform the patient and his/her companion about red-flag symptoms: · A headache that gets worse and does not go away. · Significant nausea or repeated vomiting. · Unusual behavior, increased confusion, restlessness, or agitation. · Drowsiness or inability to wake up · Slurred speech, weakness, numbness, or decreased coordination. · Convulsions or seizures (shaking or twitching). · Loss of consciousness (passing out) |
Good Practice Statement |
- Recommendations
We recommend the Canadian CT Head Rule (CCHR) to guide CT use in adults with mild head injury not on anticoagulants or antiplatelets, to minimize unnecessary imaging. If CT imaging is not available, refer to an appropriate facility.
CT is indicated if any of the following are present:
· Failure to reach a GCS score of 15 within 2 hours of injury.
· Suspected open skull fracture.
· Signs of basal skull fracture.
· Vomiting more than once.
· Age > 64 years.
The Canadian CT Head Rule (CCHR) is not applicable to patients younger than 16 years, those receiving blood thinners, or patients who experience a post-traumatic seizure.
(Strong recommendation, High certainty of evidence) 4,18,20–22
|
Criterion |
Judgment |
|
Certainty of the evidence |
High |
|
Values and preferences |
No important uncertainty or variability |
|
Desirable effects |
Large |
|
Undesirable effects |
Small |
|
Balance of effects |
Favors the intervention |
|
Resources required |
Large savings |
|
Certainty of evidence for resources |
No included studies |
|
Cost-effectiveness |
Favors the intervention |
|
Problem priority |
Yes |
|
Equity |
increased |
|
Acceptability |
Yes |
|
Feasibility |
Yes |
(2) In adults over 60 years old with head trauma who present with loss of consciousness or post-traumatic amnesia, do immediate CT brain imaging, compared to no CT or delayed imaging, improve the detection of clinically significant intracranial injury and guide appropriate management?
We recommend performing a non-contrast head CT in patients over 60 years old who are present with loss of consciousness or post traumatic amnesia. If CT imaging is not available, refer to an appropriate facility.
(Strong recommendation, High certainty of evidence) 19,23
|
Certainty of Evidence |
High |
|
Values and Preferences |
No important uncertainty or variability |
|
Desirable Effects |
Large |
|
Undesirable Effects |
Small |
|
Balance of Effects |
Probably favors the intervention |
|
Resources Required |
Moderate costs |
|
Certainty of Resource Evidence |
No included studies |
|
Cost-Effectiveness |
Probably favors the intervention |
|
Problem Priority |
Yes |
|
Equity |
Probably increased |
|
Acceptability |
Yes |
|
Feasibility |
Yes |
(3) In intoxicated patients with mild head trauma , does CT scanning compared to observation improve detection of clinically significant brain injury?
We recommend performing a non-contrast head CT in intoxicated patients with mild head trauma who present with loss of consciousness or posttraumatic amnesia. If CT imaging is not available, refer to an appropriate facility.
(Strong recommendation, Moderate certainty of evidence) 19,23
|
Criterion |
Judgment |
|
Certainty of the evidence |
High |
|
Values and preferences |
Probably no important uncertainty or variability |
|
Desirable effects of intervention (CT) |
Moderate |
|
Undesirable effects of intervention (CT) |
Small |
|
Balance of effects |
Favors the intervention (CT) |
|
Resources required |
Moderate costs |
|
Certainty of evidence for resources |
No included studies |
|
Cost-effectiveness |
Favors the intervention (CT) |
|
Priority of the problem |
Yes |
|
Equity |
increased |
|
Acceptability |
Yes |
|
Feasibility |
Yes |
(4) In adults with mild head injury (MHI) who are neurologically intact and are receiving anticoagulant or antiplatelet therapy , do routine head computed tomography (CT) imaging compared to no CT imaging improve the detection of intracranial hemorrhage?
We recommend performing a non-contrast head CT in anticoagulated patients with mild head injury, rather than relying solely on clinical decision tools to exclude imaging. If CT imaging is not available, refer to an appropriate facility.
(Strong recommendation, Low certainty of evidence) 18,24–29
|
Criterion |
Judgment |
|
Certainty of the evidence |
Low |
|
Values and preferences |
No important uncertainty or variability |
|
Desirable effects |
Large |
|
Undesirable effects |
Small |
|
Balance of effects |
Favors the intervention |
|
Resources required |
Moderate costs |
|
Certainty of resource evidence |
No included studies |
|
Cost-effectiveness |
Favors the intervention |
|
Priority of the problem |
Yes |
|
Equity |
Probably increased |
|
Acceptability |
Yes |
|
Feasibility |
Yes |
(5) In the same group of patients , does repeating a CT scan after an initial negative CT compared to no repeat CT improve detection of delayed intracranial hemorrhage?
We advise against routine repeating a non-contrast head CT in adults with mild head injury on anticoagulants or antiplatelets who remain at baseline neurologic assessment, if the initial CT is negative for hemorrhage.
(Conditional recommendation, Moderate certainty of evidence) 18,25–29
|
Criterion |
Your Judgment |
|
Certainty of evidence |
Moderate |
|
Values and preferences |
Probably no important uncertainty or variability |
|
Desirable effects |
Small |
|
Undesirable effects |
Moderate |
|
Balance of effects |
Favors the comparison (no repeat CT) |
|
Resources required |
Moderate costs |
|
Certainty of resource evidence |
No included studies |
|
Cost-effectiveness |
Favors the comparison |
|
Priority of the problem |
Probably No |
|
Equity |
Probably no impact |
|
Acceptability |
Probably No |
|
Feasibility |
Yes |
(6) In patients with mild head injury , does hospital admission compared with discharge with observation at home improve early detection and management of complications?
We recommend admitting patients with mild head injury to hospital if clinical assessment identifies any risk factors or concerning features that warrant close observation or further management.
Admission is advised when one or more of the established admission criteria for mild head injury are present:
· New, clinically important abnormalities on imaging (An isolated simple linear non-displaced skull fracture is unlikely to be clinically important unless the patient is taking anticoagulant or antiplatelet medication.)
· GCS score did not return to 15 (or pre-injury baseline) after imaging, regardless of the imaging results.
· Indications for CT scanning are present, but scanning cannot be performed within the appropriate time period, either because CT is unavailable or because the person is not sufficiently cooperative to allow scanning.
· Continuing worrying symptoms of concern to the clinician, such as persistent vomiting, severe headaches, or seizures.
· Other sources of clinician concern, including but not limited to drug or alcohol intoxication, other injuries, shock, suspected non-accidental injury, meningism, cerebrospinal fluid leak, or suspicion of ongoing post-traumatic amnesia.
(Good practice statement)
(7) In patients presenting with mild head injury , does discharging them from hospital based on normal clinical assessment and imaging results compared to continued observation or hospital admission lead to safe outcomes without missed clinically significant brain or cervical spine injuries?
We recommend discharging patients with mild head injury when clinical assessment and investigations identify no evidence of clinically important brain or cervical spine injury, provided that:
· CT scan of the head and/or cervical spine is not indicated or has shown normal findings, and the Glasgow Coma Scale (GCS) has returned to 15 or the pre-injury baseline.
· There are no other factors that would warrant hospital admission. (refer to recommendation number 6)
· There is appropriate supervision at home or a suitable environment for continued observation in the community.
(Good practice statement)
(8) In adults with mild head trauma, normal neurological exam, and on anticoagulants/antiplatelets , is inpatient admission, or prolonged ED observation compared to safe discharge from the ED equally safe without missed complications?
We advise against routine hospital admission in anticoagulated or antiplatelet-treated patients with mild head injury who have a normal neurological exam, a normal initial CT, and lack criteria warranting extended monitoring.
The criteria warranting extended monitoring and hospital admission are the same as those for patients who are not taking anticoagulant or antiplatelet therapy.
(Conditional recommendation, Low certainty of evidence) 18,25–30
|
Criterion |
Judgment |
|
Certainty of the evidence |
Moderate |
|
Values and preferences |
Possibly important uncertainty or variability |
|
Desirable effects of intervention (admission) |
Small |
|
Undesirable effects of intervention (admission) |
Moderate |
|
Balance of effects |
Favors the comparison (discharge) |
|
Resources required |
Large costs |
|
Certainty of evidence for resources |
High |
|
Cost-effectiveness |
Favors the comparison (discharge) |
|
Priority of the problem |
Yes |
|
Equity |
Reduced (with intervention) |
|
Acceptability |
No (for intervention) |
|
Feasibility |
No (for intervention) |
(9) In adults with mild head trauma , does providing discharge advice including red-flag symptoms and when to seek re-evaluation compared to no structured advice improve early recognition of complications and timely return for care?
We recommend providing written discharge instructions outlining red-flag symptoms and follow-up guidance to adults with mild head injury to improve early recognition of complications.
A. Discharge instructions should include advice to:
· Avoid activities that may increase the risk of recurrent head injury.
· Maintain social contact and communicate with family or friends about recovery symptoms.
· Use only medications approved by the treating physician for symptom control.
· Limit screen time and exposure to loud noise before sleep, keep a consistent sleep schedule, and rest in a quiet, dark environment.
B. Inform a trusted person about the injury and the warning signs to monitor for, as they may recognize symptoms before the patient does.
C. Arrange a follow-up visit within 48 hours of discharge.
On discharge you should inform the patient and his/her companion about red-flag symptoms:
· A headache that gets worse and does not go away.
· Significant nausea or repeated vomiting.
· Unusual behavior, increased confusion, restlessness, or agitation.
· Drowsiness or inability to wake up
· Slurred speech, weakness, numbness, or decreased coordination.
· Convulsions or seizures (shaking or twitching).
· Loss of consciousness (passing out)
(Good practice statement)
- Acknowledgement
Chairperson of the Guideline Development Group (GDG):
· Prof. Dr. Jehan Ali ElKholy, Head of Scientific Committee of the Egyptian Board of the Emergency Medicine. Head of Anesthesia, SICU & Pain Management Cairo University. Provided overall supervision and coordination of the guideline development process. Conducted comprehensive revision of the introduction and all recommendations
Members of the Guideline Development Group (GDG):
· Dr. Wael Atia Ahmed Abdel Aziz, Consultant and Head of Emergency Medicine Department, Dar Al-Fouad Hospital: Served as the principal architect of the recommendations, leading the clinical structuring and framing of Recommendations 1–9, defining their scope, flow, and clinical logic; contributed substantially to drafting the recommendations; and revised the Introduction to ensure alignment with clinical practice and guideline objectives.
· Dr. Radwa Muhammad Ashour, Lecturer of Emergency medicine and critical care, Suez University: Provided overall supervision and coordination of the guideline development process; led PICO questions formulation; formatted Recommendations 1–9 and ensured consistency across sections; managed and verified references; and conducted comprehensive revision of the Introduction and all recommendations.
· Dr. Nahla El-Sebaie Mostafa, Lecturer of Emergency Medicine and Traumatology - Tanta University: Authored the Introduction; contributed to writing Recommendations 5–9; and revised Recommendations 1–4.
· Dr. Lekaa Ebrahim Ahmed Elsherbiny, Lecturer of Emergency Medicine, Mansoura University: Contributed to writing Recommendations 1–4 and critically revised Recommendations 5–9.
· Dr. Omnia Yahia El Sayed Kamel, Lecturer of Anesthesia, surgical intensive care and pain management, Kasr Al Ainy teaching hospitals, Cairo University: Participated in writing Recommendations 5–9 and revision of Recommendations 1–4.
· Dr. Ibrahim Hassan Ibrahim Elsayed, Lecture of Critical care medicine, The Military Medical Academy: Contributed to writing Recommendations 1–4 and revision of Recommendations 5–9.
· Dr. Mohamed Saied Hamza Yousef, Teaching assistant of Emergency Medicine-Kasralainy-Cairo University: Participated in writing Recommendations 1–4 and revision of Recommendations 5–9.
· Dr. Ola Alaa Eldin Attia, Lecturer of Anesthesia, surgical intensive care and pain management, Kasr Al Ainy teaching hospitals, Cairo University: Contributed to writing Recommendations 5–9 and revision of Recommendations 1–4.
· Dr. Mai Mohammed Salama, National Methodologist, National Hepatology and Tropical Medicine Research institute NHTMRI: Provided methodological support, including guidance on evidence appraisal, certainty grading, and alignment with evidence-based guideline development standards.
· Dr. Athar Reda Ibrahim, National Guidelines Methodologist, Pediatrics Consultant, Quality Management Director, National Institute of Diabetes and Endocrinology, Clinical Research Consultant, Research & Development (R&D) Department, Heliopolis university for sustainable development, Cairo, Egypt: Supported methodology and evidence assessment, particularly in level-of-evidence evaluation and strength-of-recommendation classification.
We would like to acknowledge the efforts of
Coordinators & Editing Supervisors
· Prof. Jehan ElKholy
· Dr. Radwa Muhammad Ashour.
· Dr. Wael Atia Ahmed Abdel Aziz.
- Abbreviations
|
CCHR |
Canadian CT Head Rule |
|
CT |
Computed Tomography |
|
DOAC |
Direct Oral Anticoagulants |
|
GCS |
Glasgow Coma Scale |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation |
|
MHI |
Mild Head Injury |
|
PICO |
Population, Intervention, Comparison, Outcome |
- Scope and Purpose
This guidelines provides evidence-based recommendations for the assessment and early management of adults with mild head injury (GCS 13–15) presenting to emergency and acute care settings, covering key decisions on neuroimaging (CT) use, referral when CT is unavailable, observation/admission criteria, safe discharge, and discharge advice.
The guideline is intended to reduce unwarranted variation in clinical practice and standardize the quality of service delivered to patients nationwide, improving safety, consistency, and efficient use of resources through clear, actionable recommendations aligned with internationally accepted guideline principles.
- Introduction
Trauma is considered a leading cause of death in the world and brain injury contributes a significant proportion of that mortality, hence it is a public health emergency. 1 In Egypt, road traffic accidents continue to represent the primary cause of head injuries, reflecting global trends identified by the World Health Organization (2023). Integrating national data underscores the public health significance of establishing standardized approaches for head injury management. 2
Mild head injury (MHI) is defined as blunt head injury with Glasgow Coma Scale (GCS) score of 13-15 within 30 minutes of injury or at presentation or as a blunt injury to the head which is accompanied with temporary loss of consciousness, amnesia or disorientation/confusion with a Glasgow Coma Score of 13-15.3,4
Some recommend classifying patients with a GCS score of 13 as moderate head injury (defined as GCS score of 9-12) because they seem more similar with regard to prognosis and incidence of intracranial abnormalities. 5,6 MHI constitute about 80-90% of all MHI, and may have intracranial pathologies requiring neurosurgical intervention in about 10% of cases, 1% of which could be life-threatening. 7
For an industrialized country, estimates of the relative causes of head injury are as follows: motor vehicle accidents (20 to 45 %), falls (30 to 38 %), occupational accidents (10 %), recreational accidents (10 %) and assaults (5 to 17 %). 8,9 In older adults, falls are more likely the cause, and motor vehicle accidents are more common in the young.
MHI results from direct external contact forces or from the brain being slapped against intracranial surfaces with acceleration/deceleration trauma. Concussion may result in neuropathologic changes, but the acute clinical symptoms are believed to reflect a disturbance of function rather than structural injury. 10
The acute evaluation of a patient with MHI includes a neurologic assessment and mental status testing. Prolonged unconsciousness (greater than one minute), persistent mental status alterations, or abnormalities on neurologic examination require urgent imaging and neurosurgical consultation.
It is important to note that MHI and concussion may be unrecognized by both the injured and non-medical trained observers, particularly if there is no loss of consciousness.11 Some surveys have found that more than 80 percent of individuals with a past concussion did not recognize it as such. 12,13
Imaging usually computed tomography (CT) without contrast is recommended for a subset of patients with MHI. While imaging is normal in patients with a concussion or MHI, studies suggest that there is a sufficient incidence of abnormalities to make imaging worthwhile in a subset of at-risk patients. One systematic review of the literature estimated the prevalence of CT abnormalities of 5% among patients presenting to a hospital with GCS of 15 and 30% for those presenting with a GCS of 13. The incidence of abnormalities leading to neurosurgical intervention was approximately 1%. 5, 14–17
- Target Audience
This guideline targets healthcare professionals and health-system stakeholders involved in the assessment and early management of adults with mild head injury (GCS 13–15) across prehospital and hospital settings.
It is primarily designed for Prehospital clinicians: EMS/ambulance clinicians and paramedics involved in triage and transfer, Emergency/acute care teams: emergency physicians, trauma/surgical teams, and ED nurses, and Consulting and diagnostic services: radiology and neurosurgery teams.
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria were followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guidelines must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Selecting peer-reviewed publications only
· Selecting guidelines written in the English language
· Excluding guidelines written by a single author, not on behalf of an organization, to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references, as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adopt Clinical Policy: Critical Issues in the Management of Adult Patients Presenting to the Emergency Department With Mild Traumatic Brain Injury - ACR Appropriateness Criteria Head Trauma: 2021 Update. 18,19
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of
Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because they represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
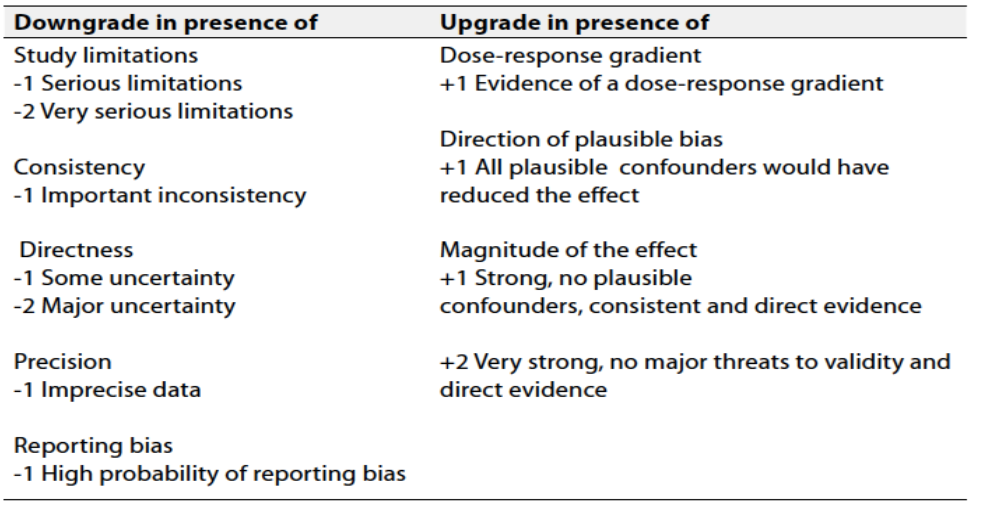
Table 1 Quality and Significance of the four levels of evidence in GRADE:
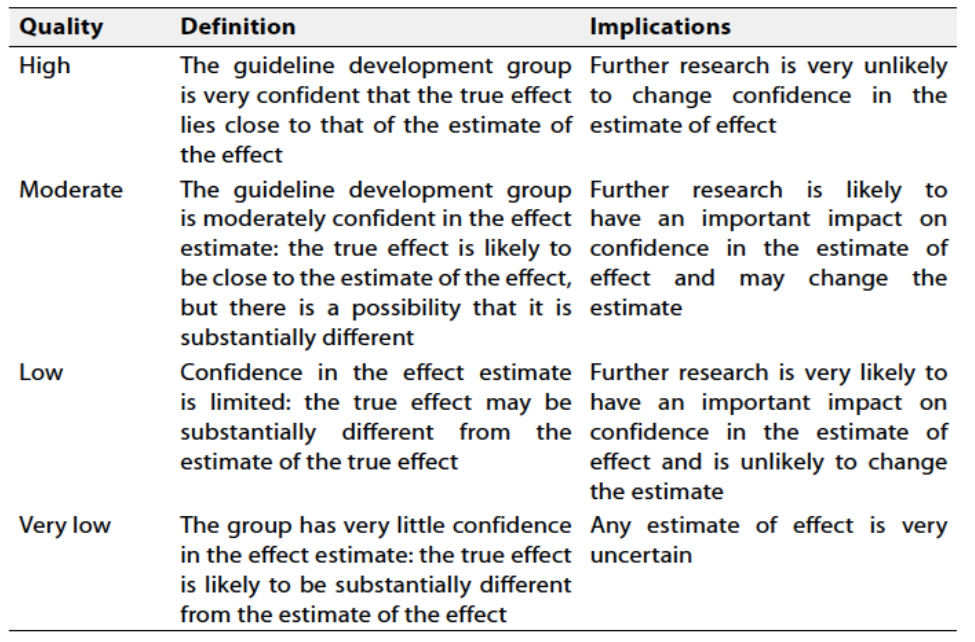
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation should account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Clinical Indicators for Monitoring
(1) Use and documentation of CCHR in eligible adults
(2) Avoidance of CT when no indication exists
(3) Referral to another facility when CT is unavailable
(4) Timely availability of radiology reports
(5) Admission when predefined clinical risk factors are present
(6) Provision of written discharge instructions with red-flag symptoms
(7) Arrangement of follow-up within 48 hours
- Research Gaps
During the review of evidence and development of recommendations, several research gaps were identified:
(1) Anticoagulated/antiplatelet patients: Clear risk stratification for CT, observation, admission, and repeat CT (especially DOACs vs warfarin).
(2) Delayed intracranial hemorrhage: Optimal duration of observation after a normal initial CT remains uncertain.
(3) Older adults: Need tailored pathways for elderly/frail patients, including those with baseline cognitive impairment or recurrent falls.
(4) Intoxicated patients: Insufficient data on safe imaging and discharge decisions when clinical assessment is unreliable.
(5) Low-resource settings: Lack of evidence on effective CT-unavailable pathways, referral thresholds, and cost-effectiveness.
(6) Patient-centered outcomes: Limited data on long-term outcomes (missed injuries, post-concussion symptoms, re-attendance, satisfaction).
- Update of the Guideline
This guideline will be updated whenever there is new evidence
- References
[1] Trauma Facts. https://www.aast.org/trauma-acs-resources/trauma-facts.html. Accessed October 20, 2025
[2] Road safety Egypt 2023 country profile. https://www.who.int/publications/m/item/road-safety-egy-2023-country-profile. Accessed October 20, 2025
[3] Smits M, Dippel DWJ, Nederkoorn PJ, Dekker HM, Vos PE, Kool DR, et al. Minor head injury: CT-based strategies for management—a cost-effectiveness analysis. pubs.rsna.orgM Smits, DWJ Dippel, PJ Nederkoorn, HM Dekker, PE Vos, DR Kool, DA van RijsselRadiology, 2010•pubs.rsna.org. 2010;254(2):532-540. doi:10.1148/RADIOL.2541081672
[4] Stiell IG, Clement CM, Rowe BH, Schull MJ, Brison R, Cass D, et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA. 2005;294(12):1511-1518. doi:10.1001/JAMA.294.12.1511
[5] Stein SC, Ross SE. The Value of Computed Tomographic Scans in Patients with Low-Risk Head Injuries. Neurosurgery. 1990;26(4). https://journals.lww.com/neurosurgery/fulltext/1990/04000/the_value_of_computed_tomographic_scans_in.12.aspx
[6] Culotta V, Sementilli M, Gerold K, Neurosurgery CW, 1996 undefined. Clinicopathological heterogeneity in the classification of mild head injury. journals.lww.comVP Culotta, ME Sementilli, K Gerold, CC WattsNeurosurgery, 1996•journals.lww.com. https://journals.lww.com/neurosurgery/fulltext/1996/02000/Clinicopathological_Heterogeneity_in_the.2.aspx. Accessed October 20, 2025
[7] Vos PE, Alekseenko Y, Battistin L, Ehler E, Gerstenbrand F, Muresanu DF, et al. Mild traumatic brain injury. Eur J Neurol. 2012;19(2):191-198. doi:10.1111/J.1468-1331.2011.03581.X
[8] Feigin VL, Theadom A, Barker-Collo S, Starkey NJ, McPherson K, Kahan M, et al. Incidence of traumatic brain injury in New Zealand: a population-based study. thelancet.comVL Feigin, A Theadom, S Barker-Collo, NJ Starkey, K McPherson, M Kahan, A DowellThe Lancet Neurology, 2013•thelancet.com. 2013;12:53. doi:10.1016/S1474-4422(12)70262-4
[9] Jennett B. Epidemiology of head injury. J Neurol Neurosurg Psychiatry. 1996;60(4):362. doi:10.1136/JNNP.60.4.362
[10] McCrory P, Meeuwisse WH, Aubry M, Cantu RC, Dvořák J, Echemendia RJ, et al. Consensus Statement on Concussion in Sport: The 4th International Conference on Concussion in Sport, Zurich, November 2012. J Athl Train. 2013;48(4):554-575. doi:10.4085/1062-6050-48.4.05
[11] Duhaime AC, Beckwith JG, Maerlender AC, Mcallister TW, Crisco JJ, Duma SM, et al. Spectrum of acute clinical characteristics of diagnosed concussions in college athletes wearing instrumented helmets: Clinical article. J Neurosurg. 2012;117(6):1092-1099. doi:10.3171/2012.8.JNS112298
[12] Delaney J, Lacroix V, … SLCJ of S, 2000 undefined. Concussions during the 1997 Canadian football league season. journals.lww.comJS Delaney, VJ Lacroix, S Leclerc, KM JohnstonClinical Journal of Sport Medicine, 2000•journals.lww.com. Published online 2000. https://journals.lww.com/cjsportsmed/fulltext/2000/01000/Concussions_During_the_1997_Canadian_Football.00003.aspx. Accessed October 20, 2025
[13] Delaney J, Abuzeyad F, … JCTJ of emergency, 2005 undefined. Recognition and characteristics of concussions in the emergency department population. Elsevier. https://www.sciencedirect.com/science/article/pii/S0736467905001228. Accessed October 20, 2025
[14] Menditto V, Lucci M, Polonara S, … GPA of emergency, 2012 undefined. Management of minor head injury in patients receiving oral anticoagulant therapy: a prospective study of a 24-hour observation protocol. Elsevier. https://www.sciencedirect.com/science/article/pii/S0196064411018877. Accessed October 20, 2025
[15] Atzema C, Mower W, Hoffman J, … JHA of emergency, 2004 undefined. Defining “therapeutically inconsequential” head computed tomographic findings in patients with blunt head trauma. Elsevier. https://www.sciencedirect.com/science/article/pii/S0196064404001969. Accessed October 20, 2025
[16] Dacey R, Alves W, Rimel R, … HWJ of, 1986 undefined. Neurosurgical complications after apparently minor head injury: assessment of risk in a series of 610 patients. thejns.org. https://thejns.org/view/journals/j-neurosurg/65/2/article-p203.xml. Accessed October 20, 2025
[17] Borg J, Holm L, Cassidy J, … PPJ of, 2004 undefined. Diagnostic procedures in mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. academia.eduJ Borg, L Holm, JD Cassidy, P Peloso, L Carroll, H Von Holst, K EricsonJournal of rehabilitation medicine, 2004•academia.edu. https://www.academia.edu/download/46458696/Diagnostic_procedures_in_mild_traumatic_20160613-30876-1p7xvap.pdf. Accessed October 20, 2025
[18] Diercks DB, Anderson JD, Byyny R, Carpenter CR, Friedman B, Gemme SR, et al. Clinical Policy: Critical Issues in the Management of Adult Patients Presenting to the Emergency Department With Mild Traumatic Brain Injury: Approved by ACEP Board of Directors, February 1, 2023 Clinical Policy Endorsed by the Emergency Nurses Association (April 5, 2023). Ann Emerg Med. 2023;81(5):e63-e105. doi:10.1016/j.annemergmed.2023.01.014
[19] Shih RY, Burns J, Ajam AA, Broder JS, Chakraborty S, Kendi AT, et al. ACR Appropriateness Criteria® Head Trauma: 2021 Update. Journal of the American College of Radiology. 2021;18(5):S13-S36. doi:10.1016/j.jacr.2021.01.006
[20] Stiell IG, Wells GA, Vandemheen K, Clement C, Lesiuk H, Laupacis A, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357(9266):1391-1396. doi:10.1016/S0140-6736(00)04561-X
[21] Ro YS, Shin S Do, Holmes JF, Song KJ, Park JO, Cho JS, et al. Comparison of clinical performance of cranial computed tomography rules in patients with minor head injury: a multicenter prospective study. Acad Emerg Med. 2011;18(6):597-604. doi:10.1111/J.1553-2712.2011.01094.X
[22] Smits M, Dippel DWJ, De Haan GG, Dekker HM, Vos PE, Kool DR, et al. External validation of the Canadian CT Head Rule and the New Orleans Criteria for CT scanning in patients with minor head injury. JAMA. 2005;294(12):1519-1525. doi:10.1001/JAMA.294.12.1519
[23] Jagoda AS, Bazarian JJ, Bruns JJ, Cantrill S V., Gean AD, Howard PK, et al. Clinical Policy: Neuroimaging and Decisionmaking in Adult Mild Traumatic Brain Injury in the Acute Setting. Ann Emerg Med. 2008;52(6):714-748. doi:10.1016/j.annemergmed.2008.08.021
[24] Probst MA, Gupta M, Hendey GW, Rodriguez RM, Winkel G, Loo GT, et al. Prevalence of Intracranial Injury in Adult Patients With Blunt Head Trauma With and Without Anticoagulant or Antiplatelet Use. Ann Emerg Med. 2020;75(3):354-364. doi:10.1016/J.ANNEMERGMED.2019.10.004
[25] Cipriano A, Pecori A, Bionda AE, Bardini M, Frassi F, Leoli F, et al. Intracranial hemorrhage in anticoagulated patients with mild traumatic brain injury: significant differences between direct oral anticoagulants and vitamin K antagonists. Intern Emerg Med. 2018;13(7):1077-1087. doi:10.1007/S11739-018-1806-1
[26] Covino M, Manno A, della Pepa GM, Piccioni A, Tullo G, Petrucci M, et al. Delayed intracranial hemorrhage after mild traumatic brain injury in patients on oral anticoagulants: is the juice worth the squeeze? Eur Rev Med Pharmacol Sci. 2021;25(7):3066-3073. doi:10.26355/EURREV_202104_25560
[27] Nishijima DK, Offerman SR, Ballard DW, Vinson DR, Chettipally UK, Rauchwerger AS, et al. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use. Ann Emerg Med. 2012;59(6). doi:10.1016/j.annemergmed.2012.04.007
[28] Menditto VG, Lucci M, Polonara S, Pomponio G, Gabrielli A. Management of minor head injury in patients receiving oral anticoagulant therapy: a prospective study of a 24-hour observation protocol. Ann Emerg Med. 2012;59(6):451-455. doi:10.1016/J.ANNEMERGMED.2011.12.003
[29] Kaen A, Jimenez-Roldan L, Arrese I, Amosa Delgado M, Lopez PG, Alday R, et al. The value of sequential computed tomography scanning in anticoagulated patients suffering from minor head injury. J Trauma. 2010;68(4):895-898. doi:10.1097/TA.0B013E3181B28A76
[30] Head injury: assessment and early management NICE guideline. Published online 2023. www.nice.org.uk/guidance/ng232. Accessed September 30, 2025