the Management of Perianal Abscess, Fistula and Recto-Vaginal Fistula
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | the Management of Perianal Abscess, Fistula and Recto-Vaginal Fistula |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:01 AM |
Description
"last update: 12 Jan 2026" Download Guideline
- Executive summary
These guidelines offer evidence-based recommendations on the targeted levels of clinical practice guidelines and provide healthcare professionals with practice guidance on the surgical management of perianal abscess, fistula and recto-vaginal fistula.
• A disease-specific history and physical examination should be performed evaluating symptoms, relevant history, abscess and fistula location, and presence of secondary cellulitis, (Good practice statement).
• We recommend against routine use of diagnostic imaging for patients with anorectal abscess or fistula. However, imaging may be considered in selected patients with an occult anorectal abscess, recurrent or complex anal fistula, immunosuppression, or anorectal Crohn’s disease, (Strong recommendation).
• Patients with acute anorectal abscess should be treated promptly with incision and drainage, (Strong recommendation).
• Abscess drainage with concomitant fistulotomy is recommended in selected patients with simple low anal fistulae. (It is not recommended in patients with complex fistulas, recurrent abscesses, IBD, preexisting incontinence, or history of anorectal surgery), (Strong recommendation).
• After I & D, we advise antibiotics to be reserved for patients with an anorectal abscess complicated by cellulitis, systemic signs of infection, or underlying immunosuppression, (Conditional recommendation).
• For patients with a simple fistula-in-ano and normal anal sphincter function, we recommend treatment with lay-open fistulotomy, (Strong recommendation).
• We recommend treatment of recurrent fistula-in-ano with endorectal advancement flap, (Strong recommendation).
• For transsphincteric fistulae, we recommend treatment with ligation of the intersphincteric fistula tract (LIFT) procedure, (Strong recommendation).
• A cutting Seton is advised selectively in the management of complex cryptoglandular anal fistulae, (Conditional recommendation).
• We recommend against the anal fistula plug and fibrin glue as they are ineffective treatments for fistula-in-ano, (Strong recommendation).
• Minimally invasive approaches, (that use endoscopic or laser closure techniques), to treat fistula- in-ano may be used, as they have a reasonable short-term healing rates but unknown long-term fistula healing and recurrence rates, (Conditional recommendation).
• We advise performing non-operative management for the initial care of obstetrical rectovaginal fistula and may also be considered for other benign and minimally symptomatic fistulae, (Conditional recommendation).
• We recommend a draining Seton because it may facilitate resolution of acute inflammation or infection associated with rectovaginal fistulae, (Strong recommendation).
• Endorectal advancement flap with or without sphincteroplasty is recommended as the procedure of choice for most patients with a rectovaginal fistula, (Strong recommendation).
• Episio-proctotomy is recommended to repair obstetrical or cryptoglandular rectovaginal fistulae in patients with anal sphincter defects, (Strong recommendation).
• We advise performing a gracilis muscle or bulbocavernosus (Martius) flap for recurrent or complex rectovaginal fistula, (conditional recommendation).
• We recommend a transabdominal approach for repair of rectovaginal fistulae that result from colorectal anastomotic complications, (Strong recommendation).
• We advise performing completion proctectomy with or without colonic pull-through or coloanal anastomosis to treat radiation-related or recurrent complex rectovaginal fistula, (Conditional recommendation).
• We recommend management of symptomatic anorectal fistula associated with Crohn’s disease, with a combination of surgical and medical approaches, (Strong recommendation).
• We recommend against surgical treatment of asymptomatic fistulae in patients with Crohn’s disease, (Strong recommendation).
• We recommend draining Setons in the multimodality therapy of fistulizing anorectal CD and may be used for long-term disease control, (Strong recommendation).
• Endorectal advancement flaps and the LIFT procedure are recommended to treat fistula-in-ano associated with CD, (Strong recommendation).
• We advise to treat symptomatic, simple, single, low anal fistulae in patients with Crohn’s disease, by lay-open fistulotomy, (Conditional recommendation).
• Fecal diversion or proctectomy, is recommended for patients with uncontrolled symptoms from complex anorectal fistulizing CD, (Strong recommendation).
- Recommendations
Section 1: Initial evaluation of anorectal abscess and fistula:
• A disease-specific history and physical examination should be performed evaluating symptoms, relevant history, abscess and fistula location, and presence of secondary cellulitis, (Good practice statement).
• We recommend against routine use of diagnostic imaging for patients with anorectal abscess or fistula. However, imaging may be considered in selected patients with an occult anorectal abscess, recurrent or complex anal fistula, immunosuppression, or anorectal Crohn’s disease, (Strong recommendation, moderate certainty evidence (10, 11)).
Section 2: Anorectal abscess:
• Patients with acute anorectal abscess should be treated promptly with incision and drainage, (Strong recommendation, low certainty evidence (10, 11)).
• Abscess drainage with concomitant fistulotomy is recommended in selected patients with simple low anal fistulae. (It is not recommended in patients with complex fistulas, recurrent abscesses, IBD, preexisting incontinence, or history of anorectal surgery), (Strong recommendation, moderate certainty evidence (10, 11)).
• After I & D, we advise antibiotics to be reserved for patients with an anorectal abscess complicated by cellulitis, systemic signs of infection, or underlying immunosuppression, (Conditional recommendation, moderate certainty evidence (10, 11)).
Section 3: Anal Fistula
• For patients with a simple fistula-in-ano and normal anal sphincter function, we recommend treatment with lay-open fistulotomy, (Strong recommendation, moderate certainty evidence (10, 11)).
• We recommend treatment of recurrent fistula-in-ano with endorectal advancement flap, (Strong recommendation, moderate certainty evidence (10, 11)).
• For transsphincteric fistulae, we recommend treatment with ligation of the intersphincteric fistula tract (LIFT) procedure, (Strong recommendation, moderate certainty evidence (10, 11)).
• A cutting Seton is advised selectively in the management of complex cryptoglandular anal fistulae, (Conditional recommendation, low certainty evidence (10, 11)).
• We recommend against the anal fistula plug and fibrin glue as they are ineffective treatments for fistula-in-ano, (Strong recommendation, moderate certainty evidence (10, 11)).
• Minimally invasive approaches, (that use endoscopic or laser closure techniques), to treat fistula- in-ano may be used, as they have a reasonable short-term healing rates but unknown long-term fistula healing and recurrence rates, (Conditional recommendation, low certainty evidence (10, 11)).
Section 4: Rectovaginal fistula:
• We advise performing non-operative management for the initial care of obstetrical rectovaginal fistula and may also be considered for other benign and minimally symptomatic fistulae, (Conditional recommendation, low certainty evidence (10, 11)).
• We recommend a draining Seton because it may facilitate resolution of acute inflammation or infection associated with rectovaginal fistulae, (Strong recommendation, low certainty evidence (10, 11)).
• Endorectal advancement flap with or without sphincteroplasty is recommended as the procedure of choice for most patients with a rectovaginal fistula, (Strong recommendation, low certainty evidence (10, 11)).
• Episio-proctotomy is recommended to repair obstetrical or cryptoglandular rectovaginal fistulae in patients with anal sphincter defects, (Strong recommendation, low certainty evidence (10, 11)).
• We advise performing a gracilis muscle or bulbocavernosus (Martius) flap for recurrent or complex rectovaginal fistula, (conditional recommendation, low certainty evidence (10, 11)).
• We recommend a transabdominal approach for repair of rectovaginal fistulae that result from colorectal anastomotic complications, (Strong recommendation, low certainty evidence (10, 11)).
• We advise performing completion proctectomy with or without colonic pull-through or coloanal anastomosis to treat radiation-related or recurrent complex rectovaginal fistula, (Conditional recommendation, low certainty evidence (10, 11)).
Section 5: Anorectal fistula associated with Crohn’s disease:
• We recommend management of symptomatic anorectal fistula associated with Crohn’s disease, with a combination of surgical and medical approaches, (Strong recommendation, moderate certainty evidence (10, 11)).
• We recommend against surgical treatment of asymptomatic fistulae in patients with Crohn’s disease, (Strong recommendation, low certainty evidence (10, 11)).
• We recommend draining Setons in the multimodality therapy of fistulizing anorectal CD and may be used for long-term disease control, (Strong recommendation, moderate certainty evidence (10, 11)).
• Endorectal advancement flaps and the LIFT procedure are recommended to treat fistula-in-ano associated with CD, (Strong recommendation, moderate certainty evidence (10, 11)).
• We advise to treat symptomatic, simple, single, low anal fistulae in patients with Crohn’s disease, by lay-open fistulotomy, (Conditional recommendation, low certainty evidence (10, 11)).
• Fecal diversion or proctectomy, is recommended for patients with uncontrolled symptoms from complex anorectal fistulizing CD, (Strong recommendation, moderate certainty evidence (10, 11)).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for developing these guidelines.
Chair of GDG: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GDG: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGREE II |
Appraisal Of Guidelines For Research And Evaluation II. |
|
CD |
Crohn’s Disease |
|
CT scan |
Computed Tomography Scan |
|
GRADE |
Grade Of Recommendations, Assessment, Development And Evaluation. |
|
GDG |
Guideline Development Group. |
|
I & D: |
Incision and drainage. |
|
LIFT |
Ligation of intersphinctreric fistula tract. |
|
MRI |
Magnetic resonance imaging. |
|
WHO |
World Health Organization. |
- Introduction
A generally accepted explanation for the cause of anorectal abscess and fistula-in-ano is that an abscess results from obstruction of an anal gland and that a fistula is caused by chronic infection and epithelialization of the abscess drainage tract.(1–3) Anorectal abscesses are described by the anatomic space in which they develop; ischiorectal (also called ischioanal) abscesses are the most common followed by intersphincteric, supralevator, and submucosal locations.(4, 5) Anorectal abscess occurs more often in males than females. In general, an abscess is treated with prompt incision and drainage. (3, 4).
Fistula-in-ano is an epithelialized tract that connects the perianal skin with the anal canal. In patients with an anorectal abscess, 30% to 70% present with a concomitant fistula-in-ano, and, of those who do not, approximately 30% to 50% will ultimately be diagnosed with a fistula in the months to years after abscess drainage. (2, 6-9). Although an anorectal abscess is described by the anatomic space in which it forms, a fistula-in-ano is classified in terms of its relationship with the internal and external anal sphincters. (9).
- Scope and purpose
The scope of these guidelines is to select patients with perianal abscess, perianal fistula and recto-vaginal fistula whom get the maximum benefit from surgical intervention.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target audience
The principle targeted audiences are the practicing surgeons, however, gastroenterologists, ICU specialists, radiologists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2016 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the Clinical Practice Guideline for the management of anorectal abscess, fistula in ano and rectovaginal fistula, 2016,(10), and the American society of colon and rectal surgeons Guideline for the management of anorectal abscess, fistula in ano and rectovaginal fistula, 2022,(11).
➡️Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
· GRADE working group: http://www.gradeworkinggroup.org
· GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 1& 2).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
these are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research needs
1. Use of laser in the treatment of perianal fistula.
2. Management of high perianal fistula.
3. Management of recurrent perianal fistula.
- Clinical indicators of monitoring
1. Documentation of the clinical symptoms and signs.
2. Radiology (MRI).
3. Documentation of the type of treatment, (medical, aspiration, surgical).
4. Documentation of the surgical details.
- Updating of the guideline
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about surgical management of anorectal abscess, fistula in ano and rectovaginal fistula. The present guideline will be updated in case of significant changes based on new evidence.
- Annexes
Table 1: Quality and Significance of the four levels of evidence in GRADE:

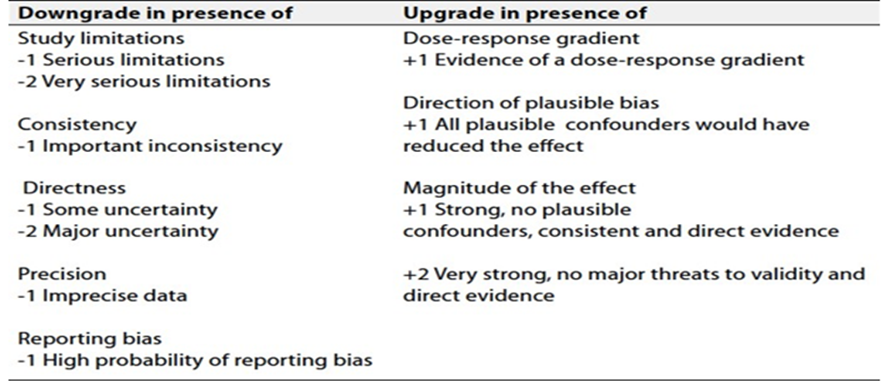
Table 2: Factors that determine How to upgrade or downgrade the quality of evidence
- References
1. Cox SW, Senagore AJ, Luchtefeld MA, Mazier WP. Outcome after incision and drainage with fistulotomy for ischiorectal abscess. Am Surg. 1997; 63:686–689.
2. Gosselink MP, van Onkelen RS, Schouten WR. The cryptoglandular theory revisited. Colorectal Dis. 2015; 17:1041–1043.
3. Abcarian H. Anorectal infection: abscess-fistula. Clin Colon Rectal Surg. 2011; 24:14–21.
4. Read DR, Abcarian H. A prospective survey of 474 patients with anorectal abscess. Dis Colon Rectum. 1979; 22:566–568.
5. Vasilevsky CA, Gordon PH. The incidence of recurrent abscesses or fistula-in-ano following anorectal suppuration. Dis Colon Rectum. 1984; 27:126–130.
6. Wang D, Yang G, Qiu J, et al. Risk factors for anal fistula: a case- control study. Tech Coloproctol. 2014; 18:635–639.
7. Hämäläinen KP, Sainio AP. Incidence of fistulae after drainage of acute anorectal abscesses. Dis Colon Rectum. 1998; 41:1357–1361.
8. Hall JF, Bordeianou L, Hyman N, et al. Outcomes after operations for anal fistula: results of a prospective, multicenter, regional study. Dis Colon Rectum. 2014; 57:1304–1308.
9. Parks AG, Gordon PH, Hardcastle JD. A classification of fistula- in-ano. Br J Surg. 1976; 63:1–12.
10. Gaertner, WB, Burgess, PL, Davids, JS, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula, Dis Colon Rectum 2022 Aug 1;65(8):964-985. doi: 10.1097/DCR.0000000000002473.
11. Vogel, JD, Johnson, EK,.Morris, AM, et al. Clinical practice guideline for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula. Dis Colon Rectum 2016; 59: 1117–1133 DOI: 10.1097/DCR.0000000000000733.