diagnosis and treatment of H pylori related diseases in children and adolescent
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | طب الأطفال |
| كتاب: | diagnosis and treatment of H pylori related diseases in children and adolescent |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:55 AM |
الوصف
"last update: 3 Feb 2026" Download Guideline
جدول المحتويات
- - Acknowledgements
- - Abbreviations
- - Glossary
- - Executive Summary
- - Introduction
- - Purpose and Scope
- - Methods
- - Recommendations
- - Evidence to recommendations: Considerations
- - Implementation Tools and Considerations
- - research needs
- - Monitoring and evaluating the impact of the guideline.
- - Updating of the guideline
- - References
- - Annexes
- Acknowledgements
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Clinicians subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Suzan Samir Gad (moderator) |
MD, Suez Canal University |
coordinate and supervise the guidelines development process, share in collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft,
|
|||
|
Ahmed Foad |
MD, Alexandria University |
Supervise and share in collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Ahmed Hamdy |
MD, Ain Shams University |
Attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Amal Mahfouz |
MD, Alexandria University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Ayman Emil Eskandr |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Gihan Bebars |
MD, Minia University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Hala Hussien Mansour |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Hanan Fathy |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Maha Abou Zekri |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Mohamed Ezz |
MD, Mansoura University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Naglaa Abu Faddan |
MD, Assuit University |
Collecting published guidelines from databases, attending online meetings of GDG, shares also in the guidelines appraisal, and she was the main organizer of the guidelines draft, and revising its final draft
|
|||
|
Sara Tarek |
MD, Cairo University |
|
|||
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Guideline Methodologists subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Prof. Ashraf Abdel Baky |
Professor of Pediatrics Ain Shams University, Egypt Founder and Chair of EPG |
Overseeing the adolopment process of the guidelines, training and education of new members, revision of the final draft, and organizing online meetings of GDG |
|||
|
Dr. Yasser Sami Amer |
1. Pediatrics Department and Clinical Practice Guidelines and Quality Research Unit, Quality Management Department, King Saud University Medical City, Riyadh, Saudi Arabia; 2. Research Chair for Evidence-Based Health Care and Knowledge Translation, King Saud University, Riyadh, Saudi Arabia; 3. Chair, Adaptation Working Group, Guidelines International Network (GIN), Perth, Scotland 4. Department of Internal Medicine, Ribeirão Preto Medical School, University of São Paulo (FMRP-USP), Ribeirão Preto, São Paulo, Brazil. |
Overseeing the adolopment process of the guidelines, training and education of new members, participating in writing up the methodology of adaptation process, guideline appraisal, and revision of the final draft |
|||
|
Lecturer of pediatrics, Faculty of Medicine, Modern University for Technology and Information (MTI), Egypt |
Participating in multiple steps of the guideline adaptation process, Writing the methodology of adaptation process and revised the whole document. |
||||
|
External Reviewers Group (ERG) |
|||||
|
External Reviewer(s) for Clinical Content |
|||||
|
|||||
|
Dr. Mohamed El Guindy |
MD, Menofiya University |
||||
|
Dr. Mostafa Hodhod |
MD, Ain Shams University |
||||
|
Dr. Ahmed Megahed |
MD, Mansoura University |
||||
|
International Peer Reviewers |
|||||
|
External Reviewer(s) for methodology |
|||||
|
Prof. Iván D. Flórez |
Department of Pediatrics, University of Antioquia, Medellín, Colombia, Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada, Leader, AGREE Collaboration (Appraisal of Guidelines for Research & Evaluation) Director, Cochrane Colombia |
||||
|
Prof. Airton Tetelbom Stein
|
Professor Titular de Saúde Coletiva, Fundação Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, Brazil Professor Adjunto, Universidade Luterana do Brasil (Ulbra), Canoas, Brazil Coordenador de Diretrizes Clínicas, Grupo Hospitalar Conceição, Porto Alegre, Brazil 4. Member, Board of Trustees, Guidelines International Network (G-I-N) |
||||
- The GDG/ GAG acknowledge EPG for its help in completing this project.
- We acknowledge JSPGHAN guidelines and ESPGHAN/NASPGHAN Guidelines
- The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatrics International (2020) 62, 1315–1331 and
Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016) guidelines (the source original guidelines) for their cooperation in providing the permission for adapting our guidelines.
· Finally, we wish the best for all our patients and their families who inspired us. It is for them this work is being finalized.
Funding
· This work is not related to any pharmaceutical or industrial company. The members of the GDG/ GAG and their institutes and universities volunteered their participation and contribution
- Abbreviations
|
- Glossary
1. Acceptability
Is the extent to which the users are likely to adopt a recommendation, based on internal qualities such as clarity, comprehensiveness, and logical reasoning and on external factors such as the burden imposed on the process and system of care, patient and providers attitudes and beliefs, and patients' needs, expectations, and preferences.
2. Adaptation (of guidelines)
Is the systematic approach to considering the use and/or modification of (a) guidelines(s) produced in one cultural and organizational setting for application in different context? Adaptation can be used as an alternative to de novo guideline development or for customizing (an) existing guideline(s) to suit the local context.
3. Adoption (of a guideline)
Is the acceptance of a guideline as a whole after the assessment of its quality, currency, and content. When health care providers (or other users of recommendations) adopt a guideline, they feel committed to change their practices in accordance with the recommendations of the guideline.
4. Applicability
Is the extent to which the users are able to put a recommendation into practice, based on internal qualities such as a clearly defined eligible patient population that matches the population to which the intervention is targeted in the local setting and external factors such as the availability of the necessary knowledge, skills, provider time, staff, equipment, and other resources.
Applicability is sometimes taken as a synonym for feasibility:
Feasibility of the acquisition of necessary skills and knowledge
Feasibility of the necessary increase in provider time, staff, equipment, and so on.
5. Culture
Culture represents the norms and values of a specific group, community, or population.
6. Diffusion
Is a passive means of transferring knowledge; it is not directed towards a target audience (e.g. publication of articles in medical journals).
7. Dissemination
Is more active than diffusion in that it targets a specific audience and involve tailoring the information for that audience (e.g. of dissemination strategies include targeted mailings, presentations, and press conferences.
8. Evidence-based principles
Evidence-Based Medicine (EBM) has been defined as ― the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of EBM means integrating individual clinical expertise with the best available external clinical evidence from systematic research.
9. Evidence tables
Are summaries of the most salient information from studies identified in the systematic review. The elements of evidence tables are dependent on the types of information in studies related to a particular topic but might include information such as the article reference, the study type (e.g. RCT or Cohort), the number of patients and their characteristics, and the intervention, comparison arms, outcome measures, and effect sizes.
10. Guideline or Clinical Practice Guideline (CPG)
Systematically developed statements about specific health problems, intended to assist practitioners and patients in making decisions about appropriate health care.
11. Guideline consistency
Agreement between the evidence and the recommendations, based on the:
Comprehensiveness of the study search and selection process,
Coherence between the results of the studies and their interpretation by the guideline authors
Transparency between interpretation and recommendations.
12. Guideline content
In the ‘ADAPTE Manual and Resource Toolkit for Guideline Adaptation’ document, guideline content refers to the recommendations in the source guidelines.
13. Guideline currency
A CPG may be considered up to date ―when (no) new information on interventions, outcomes, and performance justifies updating (it).
14. Guideline quality
By quality of clinical practice guidelines, we mean the confidence that the potential biases of guideline development addressed adequately and that the recommendations are both internally and externally valid, and are feasible for practice. This process involves taking into account the benefits, harms and costs of the recommendations, as well as the practical issues attached to them. Therefore, the assessment (of quality) includes judgments about the methods used for developing the guidelines, the content of the final recommendations, and the factors linked to their uptake.
15. Guideline topic
In the ADAPTE Manual and Resource Toolkit for Guideline Adaptation' document, the topic refers to the theme of the guideline, as described in the guideline title, for a targeted population (disease and patients) and intervention. The purpose, the audience, and the setting intended for the guideline, although not necessarily explicitly stated in the title, are also part of the topic. A guideline on a given topic may contain more than one health question.
16. Health question or clinical question or key question
Is a precisely described health issue (e.g. clinical, professional practice or public health) relating to the topic of the guideline? Guideline may include one or more questions.
17. Implementation
Implementation includes methods to promote the uptake of research findings into routine healthcare in both clinical and policy contexts and hence to improve the quality and effectiveness of healthcare. It includes the study of influences on healthcare professional and organizational behavior.
18. Intra-class correlations
Intra-class correlations provide a measurement of the extent to which two or more raters agree when rating the same set of things. It is a reliability index and is typically a ratio of the variance of interest over the sum of the variance of interest plus error.
19. Recommendation
Any statement that promotes or advocates a particular course of action in clinical care.
20. Stakeholder
A stakeholder is an individual, group and/or organization with a stake in your decision to implement a guideline. Stakeholders include individuals or groups who will be directly or indirectly affected by the implementation of a guideline.
21. Source guideline
In the ADAPTE Manual and Resource Toolkit for Guideline Adaptation' document, source guideline refers to those guidelines selected to undergo assessments of quality, currency, content, consistency, and acceptability/applicability and upon which an adapted guideline may be based.
- Executive Summary
Helicobacter pylori (H. pylori) is one of the most common bacterial infections worldwide. (1) It is a Gram-negative microaerophilic bacterium colonizes the gastric mucosa, (2) the infections are usually acquired during early childhood and generally passes asymptomatically in most patients, in which it will remain in the gastric cavity throughout life in the absence of eradication therapy. (3)
The prevalence of infection in pediatric age is high and varies from country to country. In Egypt, a population-based cross-sectional study performed among asymptomatic school children used urea breath test (UBT) to show that the overall H. pylori prevalence was 72.38%. Its main risk factor is residing in an overcrowded home and socially deprived area (4) In a rural area, relatives with low socioeconomic level generally showed the highest seroprevalence (82.5% and 78.1%, respectively). (5)
Another cross-sectional study showed that seroprevalence of H. pylori was significantly age-dependent: 60.6% of patients aged more than 5 years and 25.9% of patients aged less than 5 years. One of the main factors associated with seroprevalence was crowding in beds. The seroprevalence among children was 59.7% in the case of more than 3 persons sharing a bed and 26.9% in the case of fewer than 3 persons sharing a bed.
Moreover, the duration of breastfeeding also played a role in H. pylori acquisition. The seroprevalence was 64.7% among children who were breastfed for <1 year and only 42.4% among those breastfed for more than 1 year. (6) A cross-sectional study showed prevalence of about 70%, indicating that the burden of H. pylori infection is high in rural areas than in urban areas. (7)
Several diagnostic tests for detection of H. pylori have been widely used in clinical practice either invasive which require endoscopy to obtain biopsies of gastric tissues, or non-invasive methods with different levels of sensitivity and specificity.(8) However, each of these tests has certain disadvantages (9) The invasive methods include histological examination, culture, urease test and molecular methods, while the non-invasive methods include urea breath testing, serology and stool antigen testing. There is no single method that can meet, on its own, the criteria for acceptable sensitivity and specificity in identification of the bacterium. In the last few years, more interest has been paid for the non-invasive methods. (10) Molecular testing assays can be also a rapid and accurate methods for the diagnosis of H. pylori infection. (11)
Spontaneous eradication is described mainly in infants and young children but unfortunately the eradication decreases with age. Without a treatment scheme, eradication is highly improbable. (12)
Although H. pylori infection is mainly acquired in childhood, complications generally arise much later. H. pylori infection is implicated in the pathogenesis of gastritis, gastric and duodenal ulcers, gastric cancer, and gastric mucosa‑associated lymphoid tissue (MALT) lymphoma (13- 16) In 2018, H. pylori was responsible for an estimated 810,000 new cases of non-cardia gastric adenocarcinoma worldwide, making it the leading cause of infection-attributable cancer ahead of high-risk human papillomavirus and hepatitis B and C viruses. (17)
It is now established that chronic H. pylori infection is the most important etiological factor for the occurrence of gastric cancer, (18-21) which is considered as the third leading cause of cancer death globally. (22) Importantly, its eradication is recommended in the treatment and/or prevention of these conditions.
There is a strong association between H. pylori infection and diseases like; lymphoma, cardiovascular disease, dermatological disease, liver and gallbladder diseases, anemia, diabetes mellitus, autoimmune disease, atopy, asthma, neurological disease, bone disease, micronutrient deficiency , iron deficiency anemia, growth restriction, and idiopathic thrombocytopenic purpura (ITP) (1,2,23) H. pylori infection can lead to these diseases apart from the gastro-intestinal system by a series of hormonal, immunological, cytokine and chemokine mediators.
Indications for treatment of this infection and optimal regimens have been proposed by a recent consensus guideline as well as optimal diagnostic tests. Eradication therapy should be considered in children under 5 years in whom the therapy is clinically indicated due to the disease or condition requiring a workup that results in the diagnosis of H. pylori infection including peptic ulcer diseases with stenotic lesion, perforation or recurrent hemorrhage, or MALT (mucosa‐associated lymphoid tissue lymphoma). Eradication therapy should also be considered in children who have recurrent or refractory IDA to iron supplementation and in whom an active H. pylori infection has been determined.
All treatment guidelines agree that the best approach to the treatment of H. pylori infection is to succeed on the first attempt, thereby avoiding re-treatment and reducing cost, anxiety, and the further promotion of resistant strains. (24)
Treatment to eliminate H pylori infection is not expected to improve symptoms in children, except in cases of peptic ulcer disease (Gastric and duodenal ulcers) (PUD). Therefore, in children fulfilling the Rome criteria for functional abdominal pain, diagnostic testing (noninvasive or invasive) for H pylori infection should not be undertaken. (25-30) In the absence of alarm signs or symptoms (persistent right upper or right lower quadrant pain, dysphagia, odynophagia, persistent vomiting, gastrointestinal blood loss, involuntary weight loss, deceleration of linear growth, delayed puberty, unexplained fever, and a family history of inflammatory bowel disease, celiac disease, or PUD), recent updated recommendations from the committee for ROME IV did not identify compelling evidence to support upper endoscopy as part of the diagnostic work up. (31)
Treatments targeting H. pylori infection consist of combinations of a PPI and several antimicrobial agents. (32,33) There are limited well-designed studies in children and adolescents with respect to the optimal duration of anti H pylori therapy. Meta-analyses of optimal duration of H pylori eradication therapy in adults have been performed and show that increasing the duration of therapy enhances eradication rates .(34) With respect to triple therapy, a recent systematic review and network analysis of studies in adults showed that 14-day duration of treatment improves eradication rates compared to 10-day, and both are superior to 7-day treatment. (35)
The recommended goal for H pylori treatment is an eradication rate of at least 90% to avoid further investigations and antibiotic use. However, the latest clinical studies published have shown that the target of 90% eradication with first-line treatment may not be achieved by these regimens especially if treatment is not tailored to antimicrobial susceptibility tests and if compliance is not optimal (> 90%). (36)
This guideline was implemented for optimal diagnosis and treatment of H pylori related diseases in Egyptian children.
Guideline development process and methods
After revising inclusion and exclusion criteria and quality appraisal results, the GDG/ GAG recommended using the following source original clinical practice guideline (CPG):
1. The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatrics International (2020) 62, 1315–1331
2. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016)
We conducted an adolopment for this guideline (Adoption, Adaptation, and Development)
- Adoption for most of the guideline recommendations.
- Adaptation for 2 recommendations according to GRADE criteria to be suitable to our Economic implications (Evidence-to-Decision (EtD) table was done)
- Development of Good Practice Statements
We can summarize the guidelines’ recommendations for H. Pylori related diseases in children and adolescent
in the following:
We recommend that testing for H. pylori be performed in children with gastric or duodenal peptic ulcer disease (PUD). If H. pylori infection is identified then treatment should be administered and eradication confirmed. (Strong)
We recommend against diagnostic testing for H. pylori infection in children with functional abdominal pain disorders. (Strong)
We recommend against diagnostic testing for H. pylori infection as part of the initial investigation in children with iron deficiency anemia (IDA). (Strong)
We suggest that in children with refractory IDA in which other causes have been ruled out, testing for H. pylori during upper endoscopy may be considered. (Conditional)
We suggest that noninvasive diagnostic testing for H. pylori infection may be considered when investigating causes of chronic immune thrombocytopenic purpura (ITP). (Conditional)
We recommend against diagnostic testing for H. pylori infection when investigating causes of short stature. (Strong)
We recommend that one of the following tests be used to determine whether H. pylori treatment was successful: (1) The 13C‑UBT. (2) A 2‑step monoclonal stool H. pylori antigen test. (Strong)
To confirm eradication, we recommend that before testing for H. pylori, wait at least 2 weeks after stopping PPIs and 4 weeks after stopping antibiotics. (Strong)
We recommend against tests to detect anti‑H. pylori antibodies as single diagnostic tests in clinical settings to diagnose active H. pylori infection. (Strong)
We recommend more than two H. pylori tests such as two non‑invasive tests (breath test and stool test), or a biopsy‑based and non‑invasive test (breath test) for more accurate diagnosis of active infection. (Strong)
We recommend considering the performance of a rapid urease test directly on gastric biopsies to determine presence/absence of H. pylori as a diagnostic test for active infection. (Conditional)
We recommend histological examination of gastric biopsies as a biopsy‑based diagnostic test for active H. pylori infection. (Conditional)
We recommend H. pylori culture because the culture method is the gold standard biopsy‑based test for active infection and it can also be used for antimicrobial susceptibility testing for optimization of eradication therapy. (GPS)
Diagnostic accuracy: pre‑eradication H&E staining sensitivity is 92%–98.8% and specificity is 89%–100%. (GPS)
We recommend that at least 6 gastric biopsies should be obtained for the diagnosis of H. pylori infection during upper endoscopy. (Strong)
Diagnostic accuracy: sensitivity of 68%–98% and specificity of 100%. (GPS)
Diagnostic accuracy: Pre‑eradication sensitivity is 91.0%–98.5% and specificity is 90.9%–100%. Post‑eradication sensitivity is 58.8%–86% and specificity is 97.8%–99.2%. (GPS)
We recommend H. pylori tests when the following endoscopic findings are observed: antrum‑predominant nodularity, ulcerations or erosions in the stomach or duodenum, disappearance of regular arrangement of collecting venules (RAC) in the gastric body. (Strong)
We recommend eradication therapy for H. pylori‑infected children with gastric and/or duodenal ulcers. (Strong)
Eradication therapy should be considered for children, 5 years of age or more, determined to be infected with H. pylori by a test for active infection, taking account possible re‑infection. (Conditional)
We recommend consideration of eradication therapy for H. pylori‑infected children who underwent diagnostic upper gastrointestinal endoscopy for abdominal symptoms. (Weak)
We recommend eradication therapy for H. pylori‑infected children with gastric MALT lymphoma. (Strong)
We recommend eradication therapy for H. pylori‑infected children with IDA when the iron deficiency is recurrent or refractory to iron supplement therapy. (Strong)
We recommend eradication therapy for H. pylori‑infected children with chronic ITP as the first‑line therapy. (Strong)
We do not recommend eradication therapies for H. pylori‑infected children with chronic idiopathic urticaria. (Conditional)
We recommend against a “test‑and‑treat” strategy for H. pylori infection for asymptomatic children to protect against gastric cancer development. (Conditional)
If H. pylori is an incidental finding at endoscopy, treatment may be considered following careful discussion of the risks and benefits of H. pylori treatment with the patient/parents. When H. pylori is detected by biopsy‑based methods in absence of PUD, treatment may be considered. (GPS)
We recommend consideration of eradication therapies for children who have a family history of gastric cancer in their first‑ or second‑degree relatives and in whom active H. pylori infection has been found. (Weak)
We recommend against a “test‑and‑treat” strategy for asymptomatic children living in the household of an H. pylori‑infected adult who received eradication therapy to prevent re‑infection in that adult. (Weak)
A proton pump inhibitor‑based triple regimen with amoxicillin and clarithromycin is recommended as first‑line therapy if strains are susceptible or susceptibility is unknown. A proton pump inhibitor‑based triple regimen with amoxicillin and metronidazole is recommended if strains are resistant to clarithromycin. (Strong)
Regarding the duration of eradication regimen in children, a 7‑day course is basically recommended. However, if clinicians judge that there is a therapeutic need according to individual risk of eradication failure, then the regimen may be extended up to 14 days. (Strong)
Second‑line therapies in children in whom first‑line therapy failed: a proton pump inhibitor‑based triple regimen with amoxicillin and metronidazole was shown to be successful in children who failed clarithromycin‑containing triple therapy. In patients with second‑line eradication failure, antimicrobial susceptibility should be obtained and salvage therapy tailored accordingly. (Strong)
Improvement of eradication rate by a combination of probiotics is not clear. However, probiotics have been shown to be effective for prevention of side effects including diarrhea. Side effects such as diarrhea, nausea, vomiting, dyspepsia or dysphagia significantly decreased when combined with probiotics. (Conditional)
We recommend that the outcome of anti‑H. pylori therapy be assessed at least 4 weeks after completion of therapy. (Strong)
We recommend that one of the following tests be used to determine whether H. pylori treatment was successful: (1) The 13C‑UBT. (2) A 2‑step monoclonal stool H. pylori antigen test. (Strong)
We recommend H. pylori testing for active infection four weeks or more after completion of eradication therapy to avoid false negative results. (Strong)
We recommend that the 13C‑urea breath test or stool antigen ELISA test using a monoclonal antibody be employed to confirm eradication. (Strong)
We recommend against H. pylori tests using endoscopic biopsy specimens (rapid urease test, histological examination, and culture method) to confirm eradication. (Conditional)
We recommend against serological tests to detect anti‑H. pylori antibodies as a single test to confirm eradication. (Strong)
Guideline Registration
PREPARE (Practice guideline REgistration for transPAREncy), WHO Collaborating Center for Guideline Implementation and Knowledge Translation, EBM Center, University of Lanzhou, Lanzhou, China. Registration Number: ((submitted and in process)). Link: http://www.guidelines-registry.org/
- Introduction
Helicobacter pylori (H. pylori) is one of the most common bacterial infections worldwide. (1) It is a Gram-negative microaerophilic bacterium colonizes the gastric mucosa, (2) the infections are usually acquired during early childhood and generally passes asymptomatically in most patients, in which it will remain in the gastric cavity throughout life in the absence of eradication therapy. (3)
The prevalence of infection in pediatric age is high and varies from country to country. In Egypt, a population-based cross-sectional study performed among asymptomatic school children used urea breath test (UBT) to show that the overall H. pylori prevalence was 72.38%. Its main risk factor is residing in an overcrowded home and socially deprived area (4) In a rural area, relatives with low socioeconomic level generally showed the highest seroprevalence (82.5% and 78.1%, respectively). (5)
Another cross-sectional study showed that seroprevalence of H. pylori was significantly age-dependent: 60.6% of patients aged more than 5 years and 25.9% of patients aged less than 5 years. One of the main factors associated with seroprevalence was crowding in beds. The seroprevalence among children was 59.7% in the case of more than 3 persons sharing a bed and 26.9% in the case of fewer than 3 persons sharing a bed.
Moreover, the duration of breastfeeding also played a role in H. pylori acquisition. The seroprevalence was 64.7% among children who were breastfed for <1 year and only 42.4% among those breastfed for more than 1 year. (6) A cross-sectional study showed prevalence of about 70%, indicating that the burden of H. pylori infection is high in rural areas than in urban areas. (7)
Several diagnostic tests for detection of H. pylori have been widely used in clinical practice either invasive which require endoscopy to obtain biopsies of gastric tissues, or non-invasive methods with different levels of sensitivity and specificity.(8) However, each of these tests has certain disadvantages (9) The invasive methods include histological examination, culture, urease test and molecular methods, while the non-invasive methods include urea breath testing, serology and stool antigen testing. There is no single method that can meet, on its own, the criteria for acceptable sensitivity and specificity in identification of the bacterium. In the last few years, more interest has been paid for the non-invasive methods. (10) Molecular testing assays can be also a rapid and accurate methods for the diagnosis of H. pylori infection. (11)
Spontaneous eradication is described mainly in infants and young children but unfortunately the eradication decreases with age. Without a treatment scheme, eradication is highly improbable. (12)
Although H. pylori infection is mainly acquired in childhood, complications generally arise much later. H. pylori infection is implicated in the pathogenesis of gastritis, gastric and duodenal ulcers, gastric cancer, and gastric mucosa‑associated lymphoid tissue (MALT) lymphoma (13- 16) In 2018, H. pylori was responsible for an estimated 810,000 new cases of non-cardia gastric adenocarcinoma worldwide, making it the leading cause of infection-attributable cancer ahead of high-risk human papillomavirus and hepatitis B and C viruses. (17)
It is now established that chronic H. pylori infection is the most important etiological factor for the occurrence of gastric cancer, (18-21) which is considered as the third leading cause of cancer death globally. (22) Importantly, its eradication is recommended in the treatment and/or prevention of these conditions.
There is a strong association between H. pylori infection and diseases like; lymphoma, cardiovascular disease, dermatological disease, liver and gallbladder diseases, anemia, diabetes mellitus, autoimmune disease, atopy, asthma, neurological disease, bone disease, micronutrient deficiency , iron deficiency anemia, growth restriction, and idiopathic thrombocytopenic purpura (ITP) (1,2,23) H. pylori infection can lead to these diseases apart from the gastro-intestinal system by a series of hormonal, immunological, cytokine and chemokine mediators.
Indications for treatment of this infection and optimal regimens have been proposed by a recent consensus guideline as well as optimal diagnostic tests. Eradication therapy should be considered in children under 5 years in whom the therapy is clinically indicated due to the disease or condition requiring a workup that results in the diagnosis of H. pylori infection including peptic ulcer diseases with stenotic lesion, perforation or recurrent hemorrhage, or MALT (mucosa‐associated lymphoid tissue lymphoma). Eradication therapy should also be considered in children who have recurrent or refractory IDA to iron supplementation and in whom an active H. pylori infection has been determined.
All treatment guidelines agree that the best approach to the treatment of H. pylori infection is to succeed on the first attempt, thereby avoiding re-treatment and reducing cost, anxiety, and the further promotion of resistant strains. (24)
Treatment to eliminate H pylori infection is not expected to improve symptoms in children, except in cases of peptic ulcer disease (Gastric and duodenal ulcers) (PUD). Therefore, in children fulfilling the Rome criteria for functional abdominal pain, diagnostic testing (noninvasive or invasive) for H pylori infection should not be undertaken. (25-30) In the absence of alarm signs or symptoms (persistent right upper or right lower quadrant pain, dysphagia, odynophagia, persistent vomiting, gastrointestinal blood loss, involuntary weight loss, deceleration of linear growth, delayed puberty, unexplained fever, and a family history of inflammatory bowel disease, celiac disease, or PUD), recent updated recommendations from the committee for ROME IV did not identify compelling evidence to support upper endoscopy as part of the diagnostic work up. (31)
Treatments targeting H. pylori infection consist of combinations of a PPI and several antimicrobial agents. (32,33) There are limited well-designed studies in children and adolescents with respect to the optimal duration of anti H pylori therapy. Meta-analyses of optimal duration of H pylori eradication therapy in adults have been performed and show that increasing the duration of therapy enhances eradication rates .(34) With respect to triple therapy, a recent systematic review and network analysis of studies in adults showed that 14-day duration of treatment improves eradication rates compared to 10-day, and both are superior to 7-day treatment. (35)
The recommended goal for H pylori treatment is an eradication rate of at least 90% to avoid further investigations and antibiotic use. However, the latest clinical studies published have shown that the target of 90% eradication with first-line treatment may not be achieved by these regimens especially if treatment is not tailored to antimicrobial susceptibility tests and if compliance is not optimal (> 90%). (36)
This guideline was implemented for optimal diagnosis and treatment of H pylori related diseases in Egyptian children.
- Purpose and Scope
- DISEASE/ CONDITION
H pylori related diseases in children and adolescent
- GUIDELINE OBJECTIVES
1. To identify diagnosis of H pylori related diseases including clinical and laboratory investigations
2. To specify proper treatment of H pylori related diseases
3. To correct common faults in diagnosis and treatment of H pylori related diseases
- INTENDED USER (Target users)
1. Primary health care physician
2. General practitioners
3. Family physician
4. Pediatrician
5. Gastroenterologist
- Health/Clinical Question (PIPOH)
- P (patients, target population):
Gender: Both genders
Age group: children and adolescent from 5-18 years Disease/condition: H pylori related diseases (N.B. age below 5 years refer to gastroenterologist)
- I (interventions and practices considered/ guideline category):
Clinical: history taking and examination
Laboratory investigations:
H pylori stool antigen
Urea breath test
Upper GIT endoscopy
Biopsy and histopathology
Biopsy and bacteriology
Biopsy and rapid urease test
Treatment
- P (Professionals / intended or target users and clinical specialties):
Primary health care physician
General practitioners
Family physician
Pediatrician
Gastroenterologist
- O (major outcomes considered):
Primary outcome: proper diagnosis of H pylori related diseases
Secondary outcome: proper treatment of H pylori related diseases
- H (Healthcare settings):
Types:
· Primary, Secondary and Tertiary Healthcare Centers.
· Governmental Healthcare Sector:
MOH, University, Military, Health Insurance Organization
•Non-Governmental Healthcare Sector:
· Private and NGO Healthcare Centers.
- Methods
Methods of search:
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation. Keywords used for search are: H pylori
Inclusion / exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on methodology of development including the systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in the last 10 years)
• Selecting peer-reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. The panel decided a cut-off point or rank the guidelines (any guideline scoring above 60% in the AGREE II Domain 3 (rigor of development) was retained).
Two guidelines were considered eligible for the AGREE II appraisal instrument which were:
1. The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatrics International (2020) 62, 1315–1331
2. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016)
After reviewing all the previous criteria and the AGREE II appraisal results the GDG/ GAG recommended using 2 guidelines:
1. The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatrics International (2020) 62, 1315–1331
2. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016)
We did Adolopment for these guidelines: (Adoption, Adaptation, and Development)
- Adoption for most of the guideline recommendations.
- Adaptation for 2 recommendations according to GRADE criteria to be suitable to our Economic implications (Evidence to Decision (EtD) table was done). In this guideline no EtD table was done.
- Development of Good Practice Statement
➡️Contributors to the guideline development process:
Guideline Development Group (GDG)/ Guideline Adaptation Group (GAG):
The GDG/ GAG included two subgroups; the clinicians/ healthcare providers subgroup and the guideline methodologists’ subgroup.
➡️Clinicians Subgroups
The clinicians’ subgroup or clinical panel for this guideline included experts with a range of knowledge, technical skills and diverse perspectives in the field of Gastroenterology
The main functions of the clinical panel were adolopment of:
1. The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatrics International (2020) 62, 1315–1331
2. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016) guideline, determining the scope of the guideline and guideline, reviewing the evidence, and formulating evidence-informed recommendations in case of changing strength of recommandations.
➡️Guideline Methodologists Subgroup
There were guideline methodologists with expertise in guidelines development, adaptation, GRADE and translation of evidence into recommendations. Methodologists provided orientation and overview of evidence-informed guideline development processes using the GRADE approach, guideline adaptation using the Adapted ADAPTE, provided AGREE II assessment of the source guidelines in collaboration with the clinician’s subgroup, generation of the EtD frameworks whenever applicable.
➡️External Review Group:
The External Review Group for this guideline comprises 3 clinical national experts who have interest and expertise in as well as eminent international reviewers in the diagnosis and treatment of H pylori.
They were identified by Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) as people who can provide valuable insights during the guideline development process.
The External Review Group was asked to comment on (peer review) the final guideline to identify any criticism on the content and to comment on clarity and applicability as well as issues relating to implementation, dissemination, ethics, regulations, or monitoring, but not to change the recommendations formulated by the GDG/ GAG. The members of the External Review Group were required to submit declarations of interest before the peer review process.
➡️Guideline Development/ Adaptation Group meetings:
GDG/ GAG meetings were organized virtually (weekly/bimonthly). Due to the extensive scope of
the guideline, EPG was responsible for overseeing the adolopment process. the timetable and objectives of each meeting. GDG/ GAG meetings were also attended by members of the methodologists. Working rules for each contributor type were outlined by the chair at the start of each meeting, covering aspects such as vocal rights, voting, and evidence to decision and recommendation formulating processes.
➡️Declarations of interests:
Prospective members of the GDG/ GAG were asked to fill in and sign the standard WHO declaration of interest and confidentiality undertaking forms. All guideline members and methodologists were also asked to fill in and sign the standard WHO declaration-of-interests.
Members of the external review group will be asked to fill in and sign the standard WHO declaration-of-interests form before the peer review process.
➡️Evidence for the guideline:
We used the GRADE system (Grading of Recommendations, Assessment, Development and Evaluation) for assigning the quality of evidence and strength of recommendations that includes the following definitions [13]. Informed by the evidence required for the GRADE Evidence to Decision (EtD) framework(s) was(were) done while considering changing strength of recommendations according to availability of some resources in the recommendations (both ETD and changing strength of recommendation were not done in this guideline).
Description of the interpretation of the GRADE four levels of certainty of evidence:
Table 1. Classification of the Quality of Evidence
|
High |
We are very confident that the true effect lies close to that of the estimate of the effect. |
|
Moderate |
We are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. |
|
Low |
Our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect. |
|
Very Low |
We have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of the effect. |
➡️GRADE EtD’s contextual factors, criteria and considerations that link to the strength of recommendations:
Criteria and Considerations:
1. Benefits and harms: When a new recommendation is developed, desirable effects (benefits) need to be weighed against undesirable effects (risks/harms), considering any previous recommendation or another alternative. The larger the gap or gradient in favor of the desirable effects over the undesirable effects, the more likely that a strong recommendation will be made.
2. Certainty of the evidence about the effects: The higher the certainty of the scientific evidence base, the more likely that a strong will be made.
3. Values and preferences: If there is no important uncertainty or variability in how much people value the main outcomes, it is likely that a strong recommendation will be made. Uncertainty or variability around these values that could likely lead to different decisions, is more likely to lead to a conditional recommendation.
4. Economic implications: Lower costs (monetary, infrastructure, equipment or human resources) or greater cost-effectiveness are more likely to support a strong recommendation.
5. Equity and human rights: If an intervention will reduce inequities, improve equity or contribute to the realization of human rights, the greater the likelihood of a strong recommendation.
6. Feasibility: The greater the feasibility of an intervention to all stakeholders, the greater the likelihood of a strong recommendation.
7. Acceptability: If a recommendation is widely supported by health workers and program managers and there is widespread acceptance for implementation within the health service, the likelihood of a strong recommendation is greater.
Table 2. Classification of the Strengths of Recommendations
|
Strong |
The desirable effects of an intervention clearly outweigh the undesirable effects (or vice versa), so most patients should receive the recommended course of action. |
|
Conditional |
There is uncertainty about the trade-offs. The clinician and patient need to discuss the patient's values and preferences, and the decision should be individualized. |
➡️Developing good practice statements:
The GDG/ GAG also developed good practice statements for this guideline, which are actionable messages relevant to the guideline questions. The justification for each good practice statement was carefully considered by the GDG/ GAG with an emphasis that they are clearly needed. Good practice statements were developed, guided by the following GRADE criteria:
1- Message is really necessary with regard to actual healthcare practice
2- Have large net positive consequence (relevant outcomes and downstream consequences) (GRADE EtD domains)
3- Collecting and summarizing the evidence is a poor use of time and resources
4- Include awell-documented, clear rationale connecting indirect evidence
5- Are clear and actionable statements.
The GDG/ GAG collectively drafted and finalized good practice statements with relevant justifications and remarks to help with their interpretation, with close support and input from the consultant and guideline methodologists.
We have used the Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for adapted guidelines (RIGHT-Ad@pt Tool) as a reporting checklist for this guideline adaptation process as recommended by the EQUATOR network.
- Recommendations
|
Health question |
Source of guideline |
Recommendation |
Quality of evidence |
Strength of recommendation |
|
1-What are the GI symptoms? |
JESPGHAN |
H. pylori related diseases in children with gastric and/or duodenal ulcers. |
High |
Strong |
|
1B |
ESPGHAN/NASPGHAN |
We recommend that testing for H pylori be performed in children with gastric or duodenal PUD. If H pylori infection is identified then treatment should be administered and eradication confirmed. |
High |
Strong |
|
1C |
ESPGHAN/NASPGHAN |
We recommend against diagnostic testing for H pylori infection in children with functional abdominal pain disorders. |
High |
Strong |
|
2A- Iron-deficiency anemia |
ESPGHAN/NASPGHAN |
We recommend against diagnostic testing for H pylori infection as part of the initial investigation in children with iron deficiency anemia (IDA). |
Moderate |
Strong |
|
2B |
ESPGHAN/NASPGHAN |
We suggest that in children with refractory IDA in which other causes have been ruled out, testing for H pylori during upper endoscopy may be considered. |
Low |
Conditional |
|
2C- Chronic ITP |
ESPGHAN/NASPGHAN |
We suggest that noninvasive diagnostic testing for H pylori infection may be considered when investigating causes of chronic immune thrombocytopenic purpura (ITP). |
Low |
Conditional |
|
2E- Short stature |
ESPGHAN/NASPGHAN |
We recommend against diagnostic testing for H pylori infection when investigating causes of short stature. |
Moderate |
Strong |
|
3A- What is the non-invasive test |
ESPGHAN/NASPGHAN |
We recommend that one of the following tests be used to determine whether H pylori treatment was successful: (1) The 13C-UBT. (2) A 2-step monoclonal stool H pylori antigen test. |
High |
Strong |
|
3B- Precautions of stool antigen |
ESPGHAN/NASPGHAN |
To confirm eradication, we recommend that before testing for H pylori, wait at least 2 weeks after stopping PPIs and 4 weeks after stopping antibiotics. |
Low |
Strong |
|
3C |
JAPANES |
We recommend against tests to detect anti-H. pylori antibodies as single diagnostic tests in clinical settings to diagnose active H. pylori infection. |
High |
Strong |
|
4- What are the uses of non-invasive |
JESPGHAN |
We recommend more than two H. pylori tests such as two non-invasive tests, i.e. breath test and stool test, or a biopsy-based and non-invasive test (i.e. breath test) for more accurate diagnosis of active infection. |
Low |
Strong |
|
5A- When to do upper endoscopy |
JESPGHAN |
We recommend considering the performance of a rapid urease test directly on gastric biopsies to determine presence / absence of H. pylori as a diagnostic test for active infection. |
Low |
Conditional |
|
5B |
JESPGHAN |
We recommend histological examination of gastric biopsies as a biopsy-based diagnostic test for active H. pylori infection. |
Moderate |
Conditional |
|
5C |
JESPGHAN |
We recommend H. pylori culture because the culture method is the gold standard biopsy-based test for active infection and it can also be used for antimicrobial susceptibility testing for optimization of eradication therapy. |
GPS |
|
|
6A- Upper endo with histopathology
|
|
Diagnostic accuracy: pre‐eradication H&E staining sensitivity is 92%–98.8% and specificity is 89%–100% |
GPS |
|
|
6B |
ESPGHAN/NASPGHAN |
We recommend that at least 6 gastric biopsies should be obtained for the diagnosis of H pylori infection during upper endoscopy. |
Low |
Strong |
|
7- upper endoscopy with bacteriology
|
JESPGHAN |
Diagnostic accuracy: sensitivity of 68%–98% and specificity of 100%
|
GPS |
|
|
8A- upper endoscopy with RUT
|
JESPGHAN |
Diagnostic accuracy: Pre‐eradication sensitivities is 91.0%– 98.5% and specificity is 90.9%–100%. Post-eradication sensitivity is 58.8%–86% and specificity is 97.8%–99.2%.
|
GPS |
|
|
8B |
JESPGHAN |
We recommend H. pylori tests when the following endoscopic findings are observed at diagnostic upper endoscopy: antrum-predominant nodularity, ulcerations or erosions in the stomach or duodenum disappearance of regular arrangement of collecting venules (RAC) in the gastric body. |
Low |
Strong |
|
9A- who should be treated PUD |
We recommend eradication therapy for H. pylori- infected children with gastric and/or duodenal ulcers. |
High |
Strong |
|
|
9B |
JESPGHAN |
Eradication therapy should be considered for children, 5 years of age or more, determined to be infected with H. pylori by a test for active infection, taking account possible re-infection. |
Low |
Conditional |
|
9C |
JESPGHAN |
We recommend consideration of eradication therapy for H. pylori-infected children who underwent diagnostic upper gastrointestinal endoscopy for abdominal symptoms. |
Very low |
Weak |
|
9D |
JESPGHAN |
We recommend eradication therapy for H. pylori-infected children with gastric MALT lymphoma. |
Moderate |
Strong |
|
9E |
JESPGHAN |
We recommend eradication therapy for H. pylori-infected children with IDA when the iron deficiency is recurrent or refractory to iron supplement therapy. |
High |
Strong |
|
9F |
JESPGHAN |
We recommend eradication therapy for H. pylori-infected children with chronic ITP as the first line therapy. |
Moderate |
Strong |
|
9G |
JESPGHAN |
We do not recommend eradication therapies for H. pylori-infected children with chronic idiopathic urticaria. |
Low |
Conditional |
|
9H |
JESPGHAN |
We recommend against a “test-and treat” strategy for H. pylori infection for asymptomatic children to protect gastric cancer development. |
Low |
Conditional |
|
9K |
ESPGHAN/NASPGHAN |
If H pylori is an incidental finding at endoscopy treatment may be considered following careful discussion of the risks and benefits of H pylori treatment with the patient/parents. When H pylori is detected by biopsy-based methods in absence of PUD, treatment may be considered. |
||
|
Family history of gastric cancer |
JESPGHAN |
We recommend consideration of eradication therapies for children who have a family history of gastric cancer in their first- or second-degree relatives and in whom active H. pylori infection has been found. |
Moderate |
Weak |
|
JESPGHAN |
We recommend against a “test-and treat” strategy for asymptomatic children living in the household of an H. pylori-infected adult who received eradication therapy to prevent re-infection in that adult. |
Moderate |
Weak |
|
|
ESPGHAN/NASPGHAN |
We recommend that testing for H pylori be performed in children with gastric or duodenal PUD. If H pylori infection is identified then treatment should be administered and eradication confirmed. |
High |
Strong |
|
|
10- how to treat |
JESPGHAN |
A proton pump inhibitor- based triple regimen with amoxicillin and clarithromycin as the first-line therapy if H. pylori strains are susceptible to clarithromycin or the antimicrobial susceptibility of the strains is unknown. a proton pump inhibitor- based triple regimen with amoxicillin and metronidazole as the first-line therapy, if H. pylori strains are shown to be resistant to clarithromycin. |
Very low |
Strong |
|
Duration of eradication regimen |
JESPGHAN |
Regarding the duration of eradiation regimen in children, a 7-day course of treatment regimen is basically recommended. However, if clinicians judge that there is a therapeutic need according to individual risk of eradication failure, then the eradication regimen should be employed as a longer duration regimen for up to 14 days.
|
Moderate |
Strong |
|
Second-line therapies |
Second-line therapies in H. pylori-infected children in whom the first-line therapy failed 1-a proton pump inhibitor- based triple regimen with amoxicillin and metronidazole was shown to be successful in children who failed in eradicating H. pylori with clarithromycin containing triple therapy. In patients with second-line eradication failure, antimicrobial susceptibility should be obtained for the infecting H. pylori strain and salvage therapy should be tailored accordingly. |
Very low |
Strong |
|
|
Role of probiotic |
Improvement of the eradication rate by a combination of probiotics is not clear. However, it has been shown to be effective for the prevention of side effects including diarrhea. Individual side-effect such as diarrhea, nausea, vomiting, dyspepsia or dysphagia, which occurred with the conventional eradication therapy, significantly decreased by combining with probiotics. |
Low |
Conditional |
|
|
11- When and how to test eradication |
ESPGHAN/NASPGHAN |
We recommend that the outcome of anti–H pylori therapy be assessed at least 4 weeks after completion of therapy. |
Moderate |
Strong |
|
ESPGHAN/NASPGHAN |
We recommend that one of the following tests be used to determine whether H pylori treatment was successful: (1) The 13C-UBT. (2) A 2-step monoclonal stool H pylori antigen test. |
High |
Strong |
|
|
JESPGHAN |
We recommend H. pylori testing for active infection four weeks or more after completion of eradication therapy to avoid false negative results. |
Low |
Strong |
|
|
JESPGHAN |
We recommend that the 13C-urea breath test or stool antigen ELISA test using a monoclonal antibody be employed to confirm eradication. |
High |
Strong |
|
|
JESPGHAN |
We recommend against H. pylori tests using endoscopic biopsy specimens (rapid urease test, histological examination, and the culture method) to confirm the eradication of the infection |
Low |
Conditional. |
|
|
|
JESPGHAN |
We recommend against serological tests to detect anti-H. pylori antibodies as a single test to confirm eradication. |
High |
Strong |
- Evidence to recommendations: Considerations
The GDG/ GAG was guided by the results of the AGREE II appraisals of the eligible CPGs and thoroughly reviewed the recommendations of the original source WHO CPGs in consideration of local contextual factors related to the national Egyptian health system like burden of the disease, equity, acceptability, feasibility, and other relevant factors. The GDG decided through an informal consensus process to adopt most recommendations however, there was a need to change the strength of 2 recommendations (B2 and B3) as they lack feasibility. Also, GDG/ GAG develops group of good practice statements to improve acceptability and feasibility.
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing Pylori diagnosis, treatment, and prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
· Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of CAP in children have been made available in several forms.
➡️Steps to implementing the guideline:
Table (9): CPG implementation strategies
|
Focus of Strategy |
Strategies |
|
Practitioners |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patients |
|
|
|
|
|
|
|
|
Organizations and regulatory bodies |
|
|
|
|
|
|
|
|
|
|
|
|
➡️Example of Dissemination and Implementation Proposed Resources
Educational materials based on this Adapted CPG for H. pylori related diseases are made available in flow chart, including
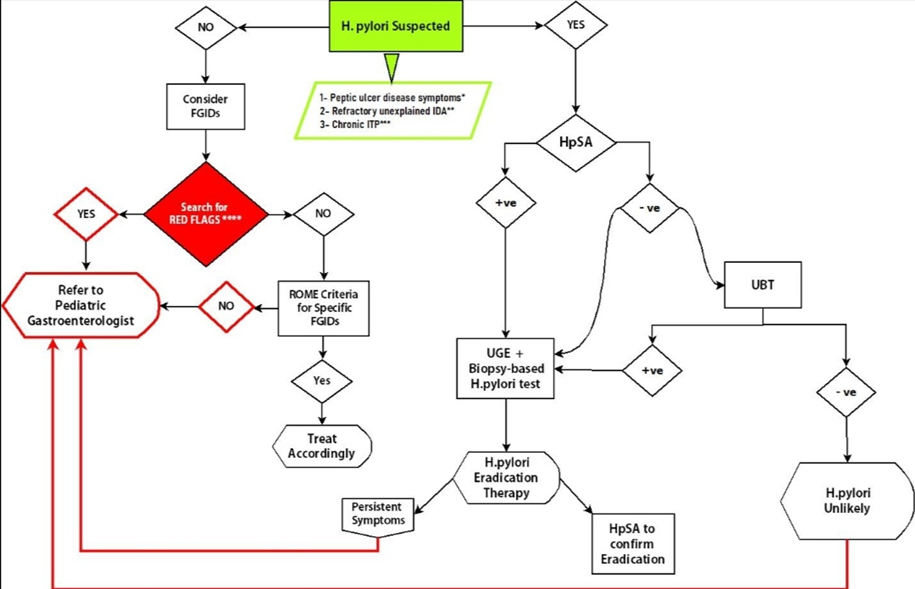
*PUD symptoms involve sudden, sharp abdominal pain, black or bloody stools, and bloody or coffee-like vomits. Other alarm features which warrant prompt gastroenterology referral include anemia, early satiety, unexplained weight loss, progressive dysphagia or odynophagia, and family history of GI cancer (Chey and Wong, 2007)
**Refractoriness to oral iron is defined as failure to respond to treatment at a dose of at least 100 mg of elemental iron per day after 4 to 6 weeks of therapy (Hershko C and Camaschella C.2014)
***Chronic ITP is defined by ITP persistence beyond 12 months, with spontaneous recovery occurring in less than 10% of adults (William B and Mitchell MD, 2019)
****Functional bowel disorders are heterogeneous group of disorder, the most prevalent of which is irritable bowel syndrome (IBS) and functional abdominal pain (FAP) syndrome. FAP characterized by frequent or continuous abdominal pain associated with a degree of loss of daily activity, in
- research needs
Future research recommendations for the management of Pylori in children in the Egyptian context could include:
· Teaching upper GIT endoscopy to be able to diagnose H.pylori.
These recommendations aim to address specific challenges and characteristics of the Egyptian context, potentially leading to more effective prevention and management strategies for Pylori in children.
➡️Challenges
· teaching upper gastrointestinal endoscopy to medical practitioners and being able to use it for diagnosing H.pylori.
Strengthen the evidence base of the next update of this guideline by generating GRADE summary of finding tables, evidence profiles, and EtD frameworks- Monitoring and evaluating the impact of the guideline.
The following are three performance measures or indicators for implementing this adapted CPG for H. Pylori. in children:
1. Adherence to H. Pylori diagnosis and treatment Guidelines
· Numerator: Number of children with H. Pylori who received treatment as per guideline recommendations.
· Denominator: Total number of children diagnosed with H. Pylori
· Data Source: Hospital or clinic patient records.
2. Duration of Hospital Stay
· Numerator: Total number of hospitals stay days for children with H. Pylori
· Denominator: Total number of children admitted with H. Pylori
· Data Source: Hospital admission and discharge records.
3. Rate of Readmission
· Numerator: Number of children readmitted with symptoms of H. Pylori within a certain period (e.g., 30 days) after discharge.
· Denominator: Total number of children initially admitted with H. Pylori
· Data Source: Hospital readmission records.
These key performance indicators are designed to measure the effectiveness and adherence to the guidelines, the efficiency of the treatment in terms of resource utilization (hospital stay), and the success of the treatment in preventing further complications (readmissions).
- Updating of the guideline
The EPG Gastroenterology GAG has decided to conduct the next review of this adapted CPG for updates after five years. This should be carried out in 2029 after checking for updates in the source CPGs, consultation of expert opinion on the changes needed for updating according to the newest evidence and recommendations published in this area and the clinical audit and feedback from implementation efforts in the aforementioned local healthcare settings except if any breakthrough evidence- based recommendations are published before that date. The process will be guided by the Checklist for the Reporting of Updated Guidelines (CheckUp) Tool that is freely provided by the AGREE Enterprise and by the Reporting Items for Practice Guidelines in Healthcare (RIGHT) extension for adapted guidelines RIGHT-Ad@pt Checklist.
- References
- Korotkaya Y and Shores D. Helicobacter pylori in Pediatric Patients. Pediatrics in Review 2020;41;585. DOI: 10.1542/pir.2019-0048.
- Aguilera Matos I, et al. BMJ Paediatrics Open 2020; 4: e 000679. doi:10.1136/bmjpo-2020-000679
- Jones NL, Koletzko S, Goodman K, et al. Joint ESPGHAN/ NASPGHAN guidelines for the management of Helicobacter pylori in children and adolescents (update 2016). J Pediatr Gastroenterol Nutr 2017; 64:991–1003.
- Mohammad MA et al. Prevalence of Helicobacter pylori infection among Egyptian children: impact of social background and effect on growth. Public Health Nutr 2008;11(3):230–6.
- Hamed ME et al. Seroprevalence of Helicobacter pylori infection among family members of infected and non-infected symptomatic children. J Egypt Soc Parasitol 2013;43(3):755–66.
- Omar A et al. Prevalence and possible risk factors of Helicobacter pylori infection among children attending Damanhour Teaching Hospital. J Egypt Public Health Assoc 2001;76(5–6):393–410.
- Sabah AA, Gneidy MR, Saleh N. Prevalence of Helicobacter pylori infection among adult patients with different gastrointestinal parasites in Tanta City district. J Egypt Soc Parasitol 2015;45(1):101–6.
- O'Ryan ML, Lucero Y, Rabello M, et al. Persistent and transient Helicobacter pylori infections in early childhood. Clin Infect Dis 2015; 61:2118.doi:10.1093/cid/civ256pmid: http://www.ncbi.nlm.nih.gov/pubmed/25838286. CrossRefPubMedGoogle Scholar
- Qi Q, Guo C, Ji R, Li Z, Zuo X, Li Y. Diagnostic Performance of Magnifying Endoscopy for Helicobacter pylori Infection: A Meta-Analysis. PLoS One 2016; 11(12): e0168201.
- Ibrahim EA-S, Moustafa M A-M, Monis W. Comparison between phenol red chromo-endoscopy and a stool rapid immunoassay for the diagnosis of Helicobacter pylori in patients with gastritis. J Microsc Ultrastruct 2015; 3:175-180.
- Ramzy I et al. Genetic mutations affecting the first line eradication therapy of Helicobacter pylori-infected Egyptian patients. Revista do Instituto de Medicina Tropical de São Paulo 2016;58.
- 12- Graham DY, Fischbach L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010; 59:1143 – 53.
- 13- Fallone CA, Chiba N, van Zanten SV, Fischbach L, Gisbert JP, Hunt RH, Jones NL, Render C, Leontiadis GI, Moayyedi P, Marshall JK. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology. 2016;151(1):51–69. doi: 10.1053/j.gastro.2016.04.006. [PubMed] [CrossRef] [Google Scholar]
- 14- Sugano K, Tack J, Kuipers EJ, Graham DY, El-Omar EM, Miura S, et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut. 2015;64(9):1353–1367. doi: 10.1136/gutjnl-2015-309252.[PMC free article] [PubMed] [CrossRef] [Google Scholar]
- 15- Wang AY, Peura DA. The prevalence and incidence of Helicobacter pylori-associated peptic ulcer disease and upper gastrointestinal bleeding throughout the world. Gastrointest Endosc Clin N Am. 2011;21(4):613–635. doi: 10.1016/j.giec.2011.07.011. [PubMed] [CrossRef] [Google Scholar]
- 16- Malfertheiner P, Megraud F, O'Morain CA, Gisbert JP, Kuipers EJ, Axon AT, et al. Management of Helicobacter pylori infection-the Maastricht V/florence consensus report. Gut. 2017;66(1):6–30. 10.1136/gutjnl-2016-312288 The most recent European guideline and recommendations related to H. pylori infection. [PubMed]
- 17- de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2019. 10.1016/S2214-109X (19)30488-7 Interesting perspective that H. pylori is responsible for more cancers worldwide than HPV, HBV, or HCV. [PubMed]
- 18- Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pyloriinfection—the Maastricht V/Florence Consensus Report.Gut 2017;66:6–30. doi:10.1136/gutjnl-2016-312288
- 19- Sugano K, Tack J, Kuipers EJ, et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015; 64:1353–67.doi:10.1136/gutjnl-2015-309252
- 20-Chey WD, Leontiadis GI, Howden CW, et al. ACG Clinical Guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol 2017; 112:212–39. doi:10.1038/ajg.2016.563
- 21- Liu WZ, Xie Y, Lu H, et al. Fifth Chinese National Consensus Report on the management of Helicobacter pylori infection. Helicobacter 2018;23: e12475. doi:10.1111/hel.12475
- 22- International Agency for Research on Cancer Helicobacter pylori Working Group Helicobacter Pylori Eradication as a Strategy for Preventing Gastric Cancer. IARC Working Group Report Volume 8. Lyon, France, 2014. Available from:http://publications.iarc.fr/Book-And-Report-Series/Iarc-Working-Group-Reports/-Em-Helicobacter-Pylori-Em-Eradication-As-A-Strategy-For-Preventing-Gastric-Cancer-2014.
- 23- Pacifico L, Osborn JF, Tromba V, Romaggioli S, Bascetta S, Chiesa C. (2014). Helicobacter pyloriinfection and extra gastric disorders in children: acriticalupdate. World J Gastroenterol, 20 (6): 1379–401. [PMC free article] [PubMed] [Google Scholar]
- 24-Fallone CA, Moss SF, Malfertheiner P. Reconciliation of recent Helicobacter pylori treatment guidelines in a time of increasing resistance to antibiotics. Gastroenterology. 2019;157(1):44–53. doi: 10.1053/j.gastro.2019.04.011. [PubMed] [CrossRef] [Google Scholar]
- 25- Emiroglu HH. Is there a relationship between Helicobacter pylori infection and erosive reflux disease in children? Acta Pædiatrica 2010; 99:121 – 5.
- 26- Llanes R, Millan LM, Escobar MP, et al. Low prevalence of Helico- bacter pylori among symptomatic children from a hospital in Havana, Cuba. J Trop Pediatr 2012; 58:231 – 4.
- 27- Mansour MM, Al Hadidi KhM, Omar MA. Helicobacter pylori and recurrent abdominal pain in children: is there any relation? Trop Gastroenterol 2012; 33:55–61.
- 28- Ganesh M, Nurko S. Functional dyspepsia in children. Pediatr Ann 2014;43: e101 – 5.
- 29- Thakkar K, Chen L, Tessier ME, et al. Outcomes of children after esophagogastroduodenoscopy for chronic abdominal pain. Clin Gastro- enterol Hepatol 2014; 12:963 – 9.
- 30- Dhroove G, Chogle A, Saps M. A million-dollar work-up for abdominal pain: is it worth it? J Pediatr Gastroenterol Nutr 2010; 51:579 – 83.
- 31- Hyams JS, Di Lorenzo C, Saps M, et al. Functional disorders: children and adolescents. Gastroenterology 2016 [Epub ahead of print].
- 32-Graham DY, Fischbach L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut. 2010;59(8):1143–53.
- 33-Graham DY, Lee Y-C, Wu M-S. Rational Helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol. 2014;12(2):177–86.
- 34- Yuan Y, Ford AC, Khan KJ, et al. Optimum durations of regimens for Helicobacter pylori eradication. Cochrane Database Syst Rev 2013:CD008337.
- 35- Li BZ, Threapleton DE, Wang JY, et al. Comparative effectiveness and tolerance of treatments for Helicobacter pylori: systematic review and network meta-analysis. BMJ 2015;351:h4052.
- 36- Kotile K, Kalac N, Homan M, Bontems P. Helicobacter pylori Infection in Pediatric Patients: Update on Diagnosis and Pediatr Drugs (2018) 20:337–351 https://doi.org/10.1007/s40272-018-0296-y
- Hershko C and Camaschella C. How I treat unexplained refractory iron deficiency anemia Blood, 2014; 123: 326–333.
- William B and Mitchell MD. Chronic Immune Thrombocytopenia in Transfusion Medicine and Hemostasis (Third Edition), 2019
- Farmer AD and Aziz Q. Mechanisms and management of functional abdominal pain. J R Soc Med. 2014; 107: 347–354
- Chey WD and Wong BCY, “American College of Gastroenterology guideline on the management of Helicobacter pylori infection,” American Journal of Gastroenterology, vol. 102, no. 8, pp. 1808–1825, 2007.View at: Publisher Site | Google Scholar
References for ADAPTE:
1. Abdel Baky A, Omar TEI, Amer YS; Egyptian Pediatric Clinical Practice Guidelines Committee (EPG). Adapting global evidence-based practice guidelines to the Egyptian healthcare context: the Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) initiative. Bull Natl Res Cent. 2023;47(1):88. https://doi.org/10.1186%2Fs42269-023-01059-0
2. Alshehri A, Almazrou S, Amer Y. Methodological frameworks for adapting global practice guidelines to national context in the Eastern Mediterranean Region. Eastern Mediterranean Health Journal. 2023 Jul 1;29(7). https://www.emro.who.int/emhj-volume-29-2023/volume-29-issue-7/methodological-frameworks-for-adapting-global-practice-guidelines-to-national-context-in-the-eastern-mediterranean-region.html
3. Schünemann H, Brozek J, Guyatt G, Oxman A (editors). GRADE handbook: handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group; 2013 (Online updated version: https://gdt.gradepro.org/app/handbook/handbook.html Accessed 16/8/2024)
4. Klugar M, Lotfi T, Darzi AJ, et al. GRADE Guidance 39: Using GRADE-ADOLOPMENT to adopt, adapt or create contextualized recommendations from source guidelines and evidence syntheses. Journal of Clinical Epidemiology. 2024 Aug 6:111494. https://doi.org/10.1016/j.jclinepi.2024.111494 (in press)
5. Amer YS, Elzalabany MM, Omar TI, Ibrahim AG, Dowidar NL. The ‘Adapted ADAPTE’: an approach to improve utilization of the ADAPTE guideline adaptation resource toolkit in the A lexandria C enter for E vidence‐B ased C linical P ractice G uidelines. Journal of evaluation in clinical practice. 2015 Dec;21(6):1095-106. https://doi.org/10.1111/jep.12479
6. Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. https://doi.org/10.1503%2Fcmaj.090449
7. Agree II (2022) AGREE Enterprise website. Available at: https://www.agreetrust.org/resource-centre/agree-ii/ (Accessed: 16/8/2024).
8. Song Y, Alonso-Coello P, Ballesteros M, et al. A Reporting Tool for Adapted Guidelines in Health Care: The RIGHT-Ad@pt Checklist[J]. Annals of Internal Medicine, 2022, 175(5):710-719. https://doi.org/10.7326/M21-4352 (Official RIGHT Statement Website: http://www.right-statement.org/extensions/13 Accessed 16/8/2024)
- Annexes
Annex Table 1.
➡️Declaration of Conflict of Interests
The members of the guideline development/ adaptation group and the external review group have no academic, financial, or competing interests to declare and none of them were involved in the development of the original source guideline(s).
Any identified potential COI has been reported below.
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Clinicians subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Suzan Samir Gad (moderator) |
MD, Suez Canal University |
coordinate and supervise the guidelines development process, share in collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft,
|
|||
|
Ahmed Foad |
MD, Alexandria University |
Supervise and share in collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Ahmed Hamdy |
MD, Ain Shams University |
Attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Amal Mahfouz |
MD, Alexandria University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Ayman Emil Eskandr |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Gihan Bebars |
MD, Minia University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Hala Hussien Mansour |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Hanan Fathy |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Maha Abou Zekri |
MD, Cairo University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Mohamed Ezz |
MD, Mansoura University |
Collecting published guidelines from databases, attending online meetings of GDG, sharing in writing up the manuscript and revising its final draft |
|||
|
Naglaa Abu Faddan |
MD, Assuit University |
Collecting published guidelines from databases, attending online meetings of GDG, shares also in the guidelines appraisal, and she was the main organizer of the guidelines draft, and revising its final draft
|
|||
|
Sara Tarek |
MD, Cairo University |
|
|||
|
Egyptian Pediatric Clinical Practice Guidelines Committee (EPG) Guideline Development/ Adaptation Group (Guideline Methodologists subgroup) |
|||||
|
Name |
Affiliation, Area of expertise / Country / Primary location [work] |
Contribution |
|||
|
Prof. Ashraf Abdel Baky |
Professor of Pediatrics Ain Shams University, Egypt Founder and Chair of EPG |
Overseeing the adolopment process of the guidelines, training and education of new members, revision of the final draft, and organizing online meetings of GDG |
|||
|
Dr. Yasser Sami Amer |
2. Pediatrics Department and Clinical Practice Guidelines and Quality Research Unit, Quality Management Department, King Saud University Medical City, Riyadh, Saudi Arabia; 3. Research Chair for Evidence-Based Health Care and Knowledge Translation, King Saud University, Riyadh, Saudi Arabia; 4. Chair, Adaptation Working Group, Guidelines International Network (GIN), Perth, Scotland 5. Department of Internal Medicine, Ribeirão Preto Medical School, University of São Paulo (FMRP-USP), Ribeirão Preto, São Paulo, Brazil. |
Overseeing the adolopment process of the guidelines, training and education of new members, participating in writing up the methodology of adaptation process, guideline appraisal, and revision of the final draft |
|||
|
Dr. Nahla Gamaleldin |
Lecturer of pediatrics, Faculty of Medicine, Modern University for Technology and Information (MTI), Egypt |
Participating in multiple steps of the guideline adaptation process, Writing the methodology of adaptation process and revised the whole document. |
|||
|
External Reviewers Group (ERG) |
|||||
|
External Reviewer(s) for Clinical Content |
|||||
|
|||||
|
Dr. Mohamed El Guindy |
MD, Menofiya University |
||||
|
Dr. Mostafa Hodhod |
MD, Ain Shams University |
||||
|
Dr. Ahmed Megahed |
MD, Mansoura University |
||||
|
International Peer Reviewers |
|||||
|
External Reviewer(s) for methodology |
|||||
|
Prof. Iván D. Flórez |
Department of Pediatrics, University of Antioquia, Medellín, Colombia, Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada, Leader, AGREE Collaboration (Appraisal of Guidelines for Research & Evaluation) Director, Cochrane Colombia |
||||
|
Prof. Airton Tetelbom Stein
|
Professor Titular de Saúde Coletiva, Fundação Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, Brazil Professor Adjunto, Universidade Luterana do Brasil (Ulbra), Canoas, Brazil Coordenador de Diretrizes Clínicas, Grupo Hospitalar Conceição, Porto Alegre, Brazil 4. Member, Board of Trustees, Guidelines International Network (G-I-N) |
||||
➡️Web annexes
The following annexes can be added as a package of standalone supplementary documents.
Keywords: The MeSH terms for "Guideline for the diagnosis and management of H. Pylori in related diseases in children and adolescent" on PubMed are: H. pylori. Children, adolescent, guidelines