Prevention of Surgical Site Infection
| Site: | EHC | Egyptian Health Council |
| Course: | Infection Prevention and Control Guidelines |
| Book: | Prevention of Surgical Site Infection |
| Printed by: | Guest user |
| Date: | Sunday, 26 July 2026, 8:26 AM |
Description
"last update: 10 Feb 2026" Download Guideline
- Executive Summary
Many factors in the patient’s journey through surgery have been identified as contributing to the risk of surgical site infection (SSI). Therefore, the prevention of these infections is complex and requires the integration of a range of preventive measures before, during and after surgery.
|
Recommendations |
|
Preoperative and Intraoperative Measures |
|
Preoperative bathing |
|
Ensure that the patient has showered (or bathed/washed if unable to shower) using either a plain or antimicrobial soap on day of or day before surgery (Conditional Recommendation) |
|
Screening and decolonization of MRSA |
|
patients undergoing cardiothoracic or orthopaedic surgery with known nasal carriage of MRSA should receive perioperative intranasal applications of mupirocin 2% ointment with or without a combination of CHG body wash (Strong Recommendation) |
|
treat also patients with known nasal carriage of MRSA undergoing other types of surgery with perioperative intranasal applications of mupirocin 2% ointment with or without a combination of CHG body wash (Conditional Recommendation) |
|
Optimal timing for preoperative surgical antibiotic prophylaxis |
|
We recommend administration of SAP prior to the surgical incision when indicated (depending on the type of operation) (Strong Recommendation) |
|
We recommend administration of SAP within 120 minutes before incision, while considering the half-life of the antibiotic (Strong Recommendation) |
|
Mechanical bowel preparation and the use of oral antibiotics |
|
Consider the use of oral antimicrobial prophylaxis prior to elective colorectal surgery to reduce the risk of SSI (Conditional Recommendation) |
|
Consider the use of mechanical bowel preparation (MBP) should be used to reduce the risk of SSI in adult patients undergoing elective colorectal surgery (Conditional Recommendation) |
|
Orthopedic and cardiothoracic procedures |
|
Decolonize surgical patients with an anti-staphylococcal agent in the preoperative setting for orthopedic and cardiothoracic procedures (Strong Recommendation) |
|
Hair removal |
|
In patients undergoing any surgical procedure, hair should either not be removed or, if absolutely necessary, it should be removed only with a clipper. Shaving is strongly discouraged at all times, whether preoperatively or in the operating room (OR) (Strong Recommendation) |
|
Surgical site preparation |
|
We recommend using alcohol-based antiseptic solutions based on CHG for surgical site skin preparation in patients undergoing surgical procedures (Strong Recommendation) |
|
Surgical hand preparation |
|
Surgical hand preparation should be performed either by scrubbing with a suitable antimicrobial soap and water or using a suitable ABHR before donning sterile gloves (Strong Recommendation) |
|
Maintaining normal body temperature (normothermia) |
|
Use of warming devices in the operating room and during the surgical procedure for patient body warming with the purpose of reducing SSI (Conditional Recommendation) |
|
For procedures not requiring hypothermia, maintain normothermia (temperature > 35.5°C) during the perioperative period (Strong Recommendation) |
|
Postoperative Measures |
|
Surgical antibiotic prophylaxis prolongation |
|
Control blood-glucose level during the immediate postoperative period for all patients (Strong Recommendation) |
|
It’s recommended against the prolongation of SAP administration after completion of the operation for the purpose of preventing SSI (Strong Recommendation) |
|
Use a checklist and/or bundle to ensure compliance with best practices to improve surgical patient safety. (Strong Recommendation) |
|
Perform surveillance for SSI. (Strong Recommendation) |
|
Provide ongoing SSI rate feedback to surgical and perioperative personnel and leadership (Strong Recommendation) |
|
Observe and review practices in the preoperative clinic, postanesthesia care unit, surgical intensive care unit and surgical ward (Moderate Recommendation) |
- Recommendations
|
Recommendations |
|
Preoperative and Intraoperative Measures |
|
Preoperative bathing |
|
Ensure that the patient has showered (or bathed/washed if unable to shower) using either a plain or antimicrobial soap on day of or day before surgery (Conditional Recommendation, Moderate Grade Evidence) |
|
Screening and decolonization of MRSA |
|
patients undergoing cardiothoracic or orthopaedic surgery with known nasal carriage of MRSA should receive perioperative intranasal applications of mupirocin 2% ointment with or without a combination of CHG body wash (Strong Recommendation, Moderate Grade Evidence) |
|
Treat also patients with known nasal carriage of MRSA undergoing other types of surgery with perioperative intranasal applications of mupirocin 2% ointment with or without a combination of CHG body wash (Conditional Recommendation, Moderate Grade Evidence) |
|
Optimal timing for preoperative surgical antibiotic prophylaxis |
|
We recommend administration of SAP prior to the surgical incision when indicated (depending on the type of operation) (Strong Recommendation, Low Grade Evidence) |
|
We recommend administration of SAP within 120 minutes before incision, while considering the half-life of the antibiotic (Strong Recommendation, Moderate Grade Evidence) |
|
Mechanical bowel preparation and the use of oral antibiotics |
|
Consider the use of oral antimicrobial prophylaxis prior to elective colorectal surgery to reduce the risk of SSI (Conditional Recommendation, Moderate Grade Evidence) |
|
Consider the use of mechanical bowel preparation (MBP) should be used to reduce the risk of SSI in adult patients undergoing elective colorectal surgery (Conditional Recommendation, Moderate Grade Evidence) |
|
Hair removal |
|
In patients undergoing any surgical procedure, hair should either not be removed or, if absolutely necessary, it should be removed only with a clipper. Shaving is strongly discouraged at all times, whether preoperatively or in the operating room (OR) (Strong Recommendation, Moderate Grade Evidence) |
|
Surgical site preparation |
|
We recommend using alcohol-based antiseptic solutions based on CHG for surgical site skin preparation in patients undergoing surgical procedures (Strong Recommendation, Low Grade Evidence) |
|
Surgical hand preparation |
|
Surgical hand preparation should be performed either by scrubbing with a suitable antimicrobial soap and water or using a suitable ABHR before donning sterile gloves (Strong Recommendation, Moderate Grade Evidence) |
|
Decolonize surgical patients with an anti-staphylococcal agent in the preoperative setting for orthopedic and cardiothoracic procedures (Strong Recommendation, High Grade Evidence) |
|
Maintaining normal body temperature (normothermia) |
|
Use of warming devices in the operating room and during the surgical procedure for patient body warming with the purpose of reducing SSI (Conditional Recommendation, Moderate Grade Evidence) |
|
For procedures not requiring hypothermia, maintain normothermia (temperature > 35.5°C) during the perioperative period (Strong Recommendation, High Grade Evidence) |
|
Postoperative Measures |
|
Surgical antibiotic prophylaxis prolongation |
|
Control blood-glucose level during the immediate postoperative period for all patients (Strong Recommendation, High Grade Evidence) |
|
It’s recommended against the prolongation of SAP administration after completion of the operation for the purpose of preventing SSI (Strong Recommendation, Moderate Grade Evidence) |
|
Use a checklist and/or bundle to ensure compliance with best practices to improve surgical patient safety. (Strong Recommendation, High Grade Evidence) |
|
Perform surveillance for SSI. (Strong Recommendation, Moderate Grade Evidence) |
|
Provide ongoing SSI rate feedback to surgical and perioperative personnel and leadership (Strong Recommendation, Moderate Grade Evidence) |
|
Observe and review practices in the preoperative clinic, postanesthesia care unit, surgical intensive care unit and surgical ward (Moderate Recommendation, Moderate Grade Evidence) |
➡️Rationale
Surgical site infections (SSIs) are potential complications associated with any type of surgical procedure. Although SSIs are among the most preventable HAIs. they still represent a significant burden in terms of patient morbidity and mortality and additional costs to health systems and service payers worldwide. Up to 60% of SSIs are preventable using evidence-based guidelines. When not prevented, SSIs can result in a significant increase in postoperative hospital days and many also require reoperation, both during the initial surgical admission and during hospital readmission. For these reasons, the prevention of SSI has received considerable attention from surgeons, infection control professionals and health care authorities.
· Factors increasing the risk of SSI
Many factors influence surgical wound healing and determine the potential for infection. These include patient-related (endogenous) and process/procedural-related (exogenous) variables that affect a patient’s risk of developing an SSI. Some variables are obviously not modifiable, such as age and gender. However, other potential factors can be improved to increase the likelihood of a positive surgical outcome, such as nutritional status, high body mass index, tobacco use, correct use of antibiotics and the intraoperative technique. Some other burden identified as diabetes, the absence or >1 hour administration of antibiotic prophylaxis and the type of wound classification (contaminated or dirty) are associated with SSI.
· Infrastructure requirements
Facilities performing surgery should have the following elements in place:
1. Trained infection prevention personnel on methods of SSI surveillance and case definitions of SSIs
2. Education for healthcare partitioners as a surgeon leader or champion who can be a critical partner in changing culture and improving adherence to prevention practices. Regularly provide education to surgeons and perioperative personnel through continuing education activities directed at minimizing perioperative SSI risk through implementation of recommended process measures.
3. Education of patients and families. Provide education for patients and patients’ families to reduce risk associated with intrinsic patient-related SSI risk factors
· Preoperative Measures
In most cases, hair removal at the surgical site should be avoided unless it interferes with the operation. If hair removal is necessary, it should be done with clippers or depilatory cream, ideally on the day of surgery and as close to the procedure as possible. Razors should not be used due to the increased risk of surgical site infections.
· Preoperative surgical antibiotic prophylaxis
Begin administration within 1 hour prior to incision to maximize tissue concentration. Administering an antimicrobial agent <1 hour prior to incision is effective. Two hours are allowed for the administration of vancomycin and fluoroquinolones according to drug bioavailability due to longer infusion times.
Select appropriate antimicrobial agents based on the surgical procedure, the most common pathogens known to cause SSI for the specific procedure, and published recommendations and adjust dosing based on patient weight. Although it is not recommended to routinely use vancomycin, this agent should be considered in patients who are known to be methicillin resistant staph aureus (MRSA) colonized (including those identified on preoperative screening), particularly if the surgery involves prosthetic material.
· Combination parenteral and oral antimicrobial agents
Use of combination parenteral and oral antimicrobial agents to reduce the risk of SSI should be considered in any surgical procedure where entry into the colon is possible or likely, as in gynecologic oncology surgery. Mechanical bowel preparation without use of oral antimicrobial agents does not decrease the risk of SSI.
· Decolonize surgical patients for orthopedic and cardiothoracic procedures.
Decolonization refers to the practice of treating patients with an antimicrobial and/or antiseptic agent to suppress MRSA. The strongest data recommend up to 5 days of intranasal mupirocin (twice daily) and bathing with chlorhexidine gluconate (CHG) (daily).
· Alcohol-containing preoperative skin preparatory agents in combination with an antiseptic
Alcohol is highly bactericidal and effective for preoperative skin antisepsis, but it does not have persistent activity when used alone. Rapid, persistent, and cumulative antisepsis can be achieved by combining alcohol with CHG or an iodophor. Be aware of the risks of using skin antiseptics in babies, in particular the risk of severe chemical injuries with the use of chlorhexidine (both alcohol-based and aqueous solutions) in preterm babies. If diathermy is to be carried out: Use evaporation to dry antiseptic skin preparations and avoid pooling of alcohol-based preparations. Alcohol is contraindicated for certain procedures due to fire risk, including procedures in which the preparatory agent may pool or not dry (e.g., involving hair). Alcohol may also be contraindicated for procedures involving mucosa, cornea, or ear.
The most effective antiseptic to combine with alcohol remains unclear; however, data from recent trials favor the use of CHG–alcohol over povidone-iodine–alcohol. CHG- alcohol is the antiseptic of choice for patients with MRSA colonization. In the absence of alcohol, CHG may have advantages over povidone-iodine, including longer residual activity and activity in the presence of blood or serum.
When deciding which antiseptic skin preparation to use, options may include those in annex 1 (table 1).
· Maintain normothermia (temperature >35.5°C) during the perioperative period for procedures not requiring hypothermia,
Even mild hypothermia can increase SSI rates. Hypothermia may directly impair neutrophil function or impair it indirectly by triggering subcutaneous vasoconstriction and subsequent tissue hypoxia. Hypothermia may increase blood loss, leading to wound hematomas or the need for transfusion - both of which can increase SSI rates.
· Control blood-glucose level during the immediate postoperative period for all patients.
Monitor and maintain postoperative blood-glucose level regardless of diabetes status. Maintain postoperative blood-glucose level between 110 and 150 mg/dL. Increased glucose levels during the operational procedure are associated with higher levels in the postoperative setting.
· Use a checklist and/or bundle to ensure compliance with best practices to improve surgical patient safety
The World Health Organization (WHO) checklist is a 19- item surgical safety checklist to improve adherence with best practices. Studies demonstrated that use of the WHO checklist led to lower surgical complication rates, including SSI and death.
· Perform surveillance for SSI.
The surveillance of HAI is one of the core components of an effective IPC program. The primary aim of surveillance is the collection of data on SSI rates in order to obtain a measure of the magnitude of the problem. These data must then be analysed to identify and investigate trends, including a careful interpretation of results. Finally, surveillance data should guide the identification of improvement actions and evaluate the effectiveness of these interventions. In this context, the feedback of SSI rates to relevant stakeholders is important.
Identify high-risk, high-volume operative procedures to be targeted for SSI surveillance based on a risk assessment of patient populations, operative procedures performed, and available SSI surveillance data. Identify, collect, store, and analyze data needed for the surveillance program. Develop a database for storing, managing, and accessing data collected on SSIs. Implement a system for collecting data needed to identify and report SSIs.
· Observe and review practices in the preoperative clinic, postanesthesia care unit, surgical intensive care unit, and/or surgical ward
a. Perform direct observation audits of hand-hygiene practices among all healthcare personnel with direct patient contact.
b. Evaluate wound care practices.
c. Perform direct observation audits of environmental cleaning practices.
d. Provide feedback and review infection control measures with healthcare personnel in these perioperative care settings.
- Acknowledgements
We would like to acknowledge the Infection Control Guidelines Committee for developing these guidelines.
Head of IPC Guidelines Committee
Professor Ghada Ismail (Professor of Clinical Pathology (Clinical Microbiology), Faculty of Medicine, Ain Shams University, Secretary of Supreme IPC Committee, SCUH, Member of WHO Global Guidelines Groups (GDG) for Infection Prevention)
Secretary of IPC Guidelines Committee
Professor Walaa Abd El-Latif (Professor of Medical Microbiology and Immunology, Faculty of Medicine Ain Shams University, IPC Consultant)
Members of the Committee
▪ Professor Amal Sayed (Deputy Manager of Environmental Affair, Infection Control Director, Cairo University Hospitals)
▪ Professor Amani El-Kholy (Clinical Pathology Department (Microbiology), Faculty of Medicine, Cairo University, Infection Control Consultant)
▪ Dr Asmaa Mohamed Abdelfatah Mohamed (Lecturer, Faculty of Nursing MTI University)
▪ Dr Gehan Mohamed Fahmy (Professor clinical microbiology ASUSH consultant infection control, Board member of IFIC EMERO region)
▪ Professor Hebatallah Gamal Rashed (Clinical Pathology Department (Microbiology), Faculty of Medicine, Assuit University, Infection Control Consultant)
▪ Dr Iman Afifi (Consultant Clinical Pathology (Microbiology) and IPC, Ain Shams University, Director IPC units of Ain Shams internal medicine and Geriatric hospitals
▪ Professor Maha El Touny (Department of internal medicine. Faculty of Medicine, Ain Shams University. Infection Control Consultant)
▪ Brigadier Dr. Mohamed Bakr Al-Attar (Assistant Commander of Military Fever Hospital for Therapeutic Affairs, Tropical Medicine Consultant)
▪ Professor Nagwa Khamis (Emeritus Consultant Clinical Pathology (Microbiology) and IPC, ASU Director IPC Department and CEO Consultant IPC, CCHE-57357)
▪ Professor Nesrine Fathi Hanafi (Professor in Medical Microbiology and Immunology Faculty of Medicine Alexandria University, Head of Infection Prevention and Control, Alexandria University Hospitals)
▪ Dr. Reham Lotfy Abdel Aziz (Environmental Health Director, EEAA, Hazardous Waste Consultant, WMRA, Ministry of Environment)
▪ Professor Sherin ElMasry (Professor of Clinical Pathology, Ain Shams University, Chief Director of IPC ASU, Health Care Quality & Patient Safety Consultant)
▪ Dr Shimaa El-Garf: Clinical Pathology Specialist, Coordinator of HAI Surveillance and Audit Electronic System for University Hospitals, RLEUH- SCUH
- Abbreviations
·
ABHR: Alcohol based hand rub
·
CABG: Coronary Artery Bypass Grafting
·
CDC: Centers for Disease Control and Prevention
·
CHG: Chlorhexidine gluconate
·
HAIs: Healthcare Associated Infections
·
HCP: Healthcare Personnel
·
IPC: Infection prevention and control
·
KPIs: Key Performance indicators
·
MBP: Mechanical bowel preparation
·
MRSA: methicillin
resistant staph aureus
· NICE: National Institute for Health and Care Excellence
·
NHSN: National Healthcare Safety Network
·
OR: Operating room
·
PAP: Perioperative antibiotic prophylaxis
·
SAP: Surgical antibiotic prophylaxis
·
SSI: Surgical Site Infection
·
WHO: World Health Organization
- Glossary
· Primary closure: It is defined as
closure of the skin level during the original surgery, regardless of the
presence of wires, wicks, drains, or other devices or objects extruding through
the incision. This
category includes surgeries where the skin is closed by some means. Thus, if
any portion of the incision is closed at the skin level, by any manner, a
designation of primary closure should be assigned to the surgery.
· Surgical antibiotic prophylaxis refers to the prevention of infectious complications by administering
an effective antimicrobial agent prior to exposure to contamination during
surgery.
· Surgical hand preparation refers to an antiseptic handwash or antiseptic handrub performed
preoperatively by the surgical team to eliminate transient flora and reduce resident
skin flora. Such antiseptics often have persistent antimicrobial activity.
· Surgical wounds are divided into four classes:
-
Clean
refers to an uninfected operative wound in which no inflammation is encountered
and the respiratory, alimentary, genital or uninfected urinary tracts are not
entered. In addition, clean wounds are primarily closed and, if necessary,
drained with closed drainage. Operative incisional wounds that follow
non-penetrating (blunt) trauma should be included in this category if they meet
the criteria.
- Clean-contaminated
refers to operative wounds in which the respiratory, alimentary, genital or
urinary tracts are entered under controlled conditions and without unusual
contamination. Specifically, operations involving the biliary tract, appendix,
vagina and oropharynx are included in this category, provided no evidence of
infection or major break in technique is encountered.
- Contaminated
refers to open, fresh, accidental wounds. In addition, operations with major
breaks in sterile technique (for example, open cardiac massage) or gross
spillage from the gastrointestinal tract, and incisions in which acute,
non-purulent inflammation is encountered ,including necrotic tissue without
evidence of purulent drainage (for example, dry gangrene), are included in this
category.
- Dirty
or infected includes old traumatic wounds with retained devitalized tissue and
those that involve existing clinical infection or perforated viscera. This
definition suggests that the organisms causing postoperative infection were
present in the operative field before the operation.
· Surgical procedure refers to an operation where at least one incision
(including a laparoscopic approach) is made through the skin or mucous
membrane, or reoperation via an incision that was left open during a prior
operative procedure AND takes place in an operating room
- Introduction
The aim of these guidelines is to provide a comprehensive range of evidence-based recommendations for interventions to be applied during the pre-, intra- and postoperative periods for the prevention of SSI, while also considering aspects related to resource availability and values and preferences.
Surgical site infections (SSIs) are potential complications associated with any type of surgical procedure. Although SSIs are among the most preventable HAIs. they still represent a significant burden in terms of patient morbidity and mortality and additional costs to health systems and service payers worldwide. Up to 60% of SSIs are preventable using evidence-based guidelines. When not prevented, SSIs can result in a significant increase in postoperative hospital days and many also require reoperation, both during the initial surgical admission and during hospital readmission. For these reasons, the prevention of SSI has received considerable attention from surgeons, infection control professionals and health care authorities.
A Surgical Site Infection prevention bundle is a structured approach that combines several evidence-based practices to reduce the risk of infections occurring at or near the surgical incision. SSIs are a significant complication of surgery, leading to increased patient suffering, prolonged hospital stays, higher healthcare costs, and even mortality.
The introduction of an SSI prevention bundle guideline aims to:
● Reduce the incidence of SSIs: By implementing a set of proven strategies, the bundle minimizes the chances of bacteria or other microorganisms contaminating the surgical site during, before, or after an operation.
● Standardize care: The guideline provides a consistent and evidence-based framework for all healthcare professionals involved in surgical procedures. This ensures that all patients receive the same high level of preventative care.
● Improve patient outcomes: Lowering the rate of SSIs leads to fewer complications, faster recovery times, and a decreased risk of readmission for patients undergoing surgery.
● Promote a multidisciplinary approach: Successful implementation of an SSI bundle requires collaboration and adherence from surgeons, nurses, anesthesiologists, and other members of the surgical team.
● Provide a basis for quality improvement: The bundle's components can be monitored and audited to assess compliance and identify areas for improvement in surgical practices.
● Educate healthcare professionals: The guideline highlights key preventative measures, reinforcing their importance and ensuring that staff are knowledgeable about best practices.
A typical SSI prevention bundle often includes interventions across the perioperative period (before, during, and after surgery). While the specific components can vary depending on the type of surgery and the healthcare setting, common elements often include:
➡️Preoperative Phase:
● Patient education: Informing patients about the importance of hygiene and what to expect before and after surgery.
● Preoperative showering or bathing with antiseptic soap (e.g., chlorhexidine): Reducing the bacterial load on the patient's skin.
● Proper hair removal (if necessary) using medical clippers: Avoiding razors, which can cause skin micro-abrasions. Use hair removal cream after doing sensitivity test for the patient if medical clipper is not available.
● Appropriate and timely administration of prophylactic antibiotics: Giving antibiotics within a specific timeframe before the incision to prevent bacterial growth during the procedure.
● Glycemic control: Managing blood sugar levels, especially in diabetic patients, as hyperglycemia can increase infection risk.
● Smoking cessation counseling: Encouraging patients to stop smoking before surgery, as smoking impairs wound healing and increases infection risk.
● Nutritional optimization: Ensuring patients are adequately nourished to support their immune system and wound healing.
➡️Intraoperative Phase:
● Surgical hand antisepsis: Surgeons and surgical staff performing thorough hand hygiene.
● Skin preparation with an antiseptic solution (e.g., chlorhexidine with alcohol): Cleaning the surgical site immediately before the incision.
● Maintaining normothermia: Keeping the patient warm during surgery, as hypothermia can impair immune function.
● Appropriate surgical attire and draping: Using sterile gowns, gloves, and drapes to maintain a sterile field.
● Minimizing traffic in the operating room: Reducing the number of people entering and exiting the surgical area.
● Using sterile instruments and supplies: Ensuring all equipment used during the surgery is properly sterilized.
● Gentle tissue handling: Minimizing tissue trauma during the procedure to promote healing.
● Appropriate wound irrigation: Washing the surgical site with sterile solution.
● Considering the use of wound protectors: Devices that can help prevent contamination of the wound edges.
● Glove and instrument changes: Changing gloves and instruments at specific points during the procedure, especially after handling contaminated areas.
Postoperative Phase:
● Proper wound care: Following established protocols for dressing changes and wound assessment.
● Early mobilization: Encouraging patients to move as soon as safely possible to improve circulation and healing.
● Pain management: Adequate pain control can contribute to better overall recovery.
● Continued glycemic control: Maintaining stable blood sugar levels postoperatively.
● Judicious use of postoperative antibiotics: Avoiding routine use of antibiotics after surgery unless there is a clear indication of infection.
● Surveillance for infection: Monitoring the surgical site for signs and symptoms of infection.
● Patient education on wound care and signs of infection: Empowering patients to recognize and report potential problems after discharge.
- Scope and Purpose
The scope of a SSI prevention bundle guideline typically encompasses all surgical procedures performed across various healthcare settings, including:
● Acute care hospitals (inpatient and outpatient surgical departments)
● Ambulatory surgery centers
● Office-based surgical suites
The guidelines are intended for all healthcare professionals involved in the surgical process
The purpose of an SSI prevention bundle guideline is to:
● Substantially decrease the incidence of Surgical Site Infections: This is the overarching goal, as SSIs are a major source of postoperative morbidity, prolonged hospitalization, increased healthcare costs, and, in some cases, mortality.
● Promote the consistent implementation of evidence-based practices: The bundle consolidates the most effective preventative measures into a practical and standardized approach.
● Improve patient safety and outcomes following surgical procedures: By reducing SSIs, patients experience fewer complications, recover more quickly, and have a lower risk of readmission.
● Provide a structured framework for perioperative care: The bundle addresses critical interventions throughout the patient's surgical journey, from the preoperative phase through the postoperative period.
● Facilitate a collaborative and multidisciplinary approach to infection prevention: Successful implementation requires the active participation and adherence of all members of the surgical team.
● Serve as a valuable tool for education and training: The guidelines highlight essential preventative measures, ensuring that all staff are knowledgeable about and competent in applying best practices.
● Establish measurable elements for performance monitoring and quality improvement: The components of the bundle can be tracked to assess compliance, identify areas for improvement, and measure the impact of interventions.
● Foster a culture of proactive prevention in surgical care: By emphasizing the importance of consistent adherence to the bundle, healthcare organizations can cultivate an environment where SSI prevention is a top priority.
- Target Audience
●
Surgical
Team: Surgeons, nurses, anesthesiologists and any professionals directly
providing surgical care.
●
Pharmacists
●
Sterilization Unit Staff
●
Infection
Prevention and Control Team
●
All
Healthcare Workers: Including Clinicians, Nurses, Head Nurses
●
Healthcare
associated infections (HAIs) Surveillance Officers
●
Health
care professionals responsible for developing national and local infection
prevention protocols and policies, such as policymakers and infection
prevention and control (IPC) professional’s patient safety and those
responsible for staff
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
● Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
● Selecting only national and/or international guidelines
● Specific range of dates for publication (using Guidelines published or updated in 2020 and later)
● Selecting peer reviewed publications only
● Selecting guidelines written in English language
● Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
● Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations.
The following characteristics of the retrieved guidelines were summarized in:
● Developing organization/authors
● Date of publication, posting, and release
● Country/language of publication
● Date of posting and/or release
● Dates of the search used by the source guideline developers.
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained). The committee decided to adapt from:
● Calderwood MS, Anderson DJ, Bratzler DW, Dellinger EP, Garcia-Houchins S, Maragakis LL, et al. Strategies to prevent surgical site infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2023;44(5):695-720. doi:10.1017/ice.2023.67
● World Health
Organization. Global guidelines for the prevention of surgical site infection.
Geneva: WHO; 2016 [last accessed 2025 Jun].
➡️Evidence assessment
According to World Health Organization (WHO) Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
● GRADE working group: http://www.gradeworkinggroup.org
● GRADE online training modules: http://cebgrade.mcmaster.ca/
Table (1) Quality and Significance of the four levels of evidence in GRADE
|
Quality |
Definition |
Implications |
|
High |
The guideline development group is very confident that the true effect lies close to that of the estimate of the effect |
Further research is very unlikely to change confidence in the estimate effect |
|
Moderate |
The guideline development group is moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibly that it is substantially different |
Further research is likely to have an important impact on confidence in the estimate of the effect and may change the estimate |
|
Low |
Confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the true effect |
Further research is very likely to have an important on confidence in the estimate of effect and is unlikely to change the estimate |
|
Very low |
The group has very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of the effect |
Any estimate of the effect is very uncertain |
Table (2) Factors that determine How to upgrade or downgrade the quality of evidence.
|
Downgrade in presence of |
Upgrade in presence of |
|
Study limitations. 1- Serious limitations 2- Very serious limitations |
Dose- response gradient. +1 Evidence of a dose-response gradient |
|
Consistency 1- Important inconsistency |
Direction of plausible bias + All plausible confounders would have reduced the effect |
|
Directness 1- Some uncertainty 2- Major uncertainty |
Magnitude of the effect +1 Strong, no plausible Confounder, consistent and direct evidence |
|
Precision 1- Imprecise data |
+2 very strong, no major threats to validity and direct evidence |
|
Reporting bias 1. High probability of reporting bias |
|
The strength of the recommendations
The strength of a recommendation communicates the importance of adherence to the recommendation.
● Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
● Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations?
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Indicators for Monitoring
To ensure the appropriate prevention of surgical site infections in hospitals and reduce the risk of readmission, specific indicators should be monitored regularly. These are some indicators which focus on measuring and improving the prevention and management of infections occurring at surgical sites. These key performance indicators (KPIs) help track the effectiveness of infection control measures and identify areas for improvement, ultimately aiming to reduce SSIs and enhance patient outcomes. Here are some key indicators that can be included in hospital guidelines for prevention of SSI.
1) Process indicators for SSI prevention
The selected KPIs can be categorized into three groups: 1) Perioperative antibiotic prophylaxis (PAP) indicators, 2) Preoperative skin preparation indicators, and 3) other SSI prevention indicators.
a. Perioperative antibiotic prophylaxis
Two PAP indicators have been added to the SSI protocol:
For the first PAP indicator, the compliance with the administration appropriateness includes (1) correct antibiotic for specific surgery, (2) correct antibiotic dose, (3) administration start time within 1 hour of incision (2 hours allowed for vancomycin and fluoroquinolones) will be assessed for all surgical procedures where PAP was indicated (according to the local protocol) and administered
● Numerator: Number of patients who appropriately received PAP
● Denominator: Total number of all selected operations performed
● Multiply by 100 so that measure is expressed as a percentage.
- For the second PAP indicator the compliance with the discontinuation of PAP within 24 hours after initiation of surgery will be assessed for all surgical procedures where PAP was indicated (according to the local protocol) and administered
● Numerator: Number of patients who discontinued PAP within 24 hours after initiation of surgery
● Denominator: Total number of all selected operations performed
● Multiply by 100 so that measure is expressed as a percentage
b. Preoperative skin preparation
The following preoperative skin preparation indicators have been added to the protocol:
o No hair removal, or if hair removal was necessary, only clipping.
o Use of alcohol-based antiseptic solutions based on CHG for surgical site skin preparation in the operating room (OR) (if no patient contraindication exists)
- The compliance with no hair removal (or if hair removal was necessary, only clipping) will be assessed for all surgeries in the selected operation type
● Numerator: Number of surgical procedures with no hair removal, or only clipping
● Denominator: Number of all surgical procedures in the procedure type
c. Other prevention indicators
The last group of indicators that are collected aggregated per operation type include two indicators:
- Ensuring the patient's normothermia in the perioperative period (within one hour of the end of operation) (36-38°C (rectal measurement) or 35,5-37,5 °C (non-rectal measurement)), if no contraindication.
● Numerator: Number of all surgical procedures where patient normothermic within one hour after surgery
● Denominator: Number of all surgical procedures in the procedure type where no contraindication
* Normothermia should NOT be assessed for surgical procedures where normothermia is contraindicated, as for example in the case of induced hypothermia for Coronary Artery Bypass Grafting (CABG).
- Using a protocol for intensive perioperative blood glucose control and blood glucose levels monitored for adult patients undergoing surgical procedures
o Numerator: Number of all surgical procedures where a protocol for intensive blood glucose control is used and the blood glucose levels monitored
o Denominator: Number of all surgical procedures in the procedure type
2) Outcome Measures:
a. Percentage of SSIs by category
The percentage of patients who develop SSIs using center of disease control and prevention / national healthcare safety network (CDC/NHSN) case definitions after a surgical procedure. The first indicator (% SSIs) gives the most complete picture for a given operative procedure but is highly dependent on the intensity of post-discharge surveillance, which varies considerably between hospitals and between countries.
● Numerator: All first SSI* in that category
● Denominator: Total number of operations in that category
● Standardization factor: Multiply by 100 so that the measure is expressed as percentage
*SSIs are included, if {Date of Onset} − {Date of Operation} +1 ≤31 or ≤91 days if implant is in place
- Plan to Update this National Clinical Guideline
This guideline will be reviewed and updated when new evidence emerges that is likely to influence the recommendations.
- Annex
Annex 1. Table (1) Options for antiseptic skin preparation (NICE guideline, Surgical site infections: prevention and treatment, updated 2020)
|
When |
Choice of antiseptic skin preparation |
|
First choice unless contraindicated or the surgical site is next to a mucous membrane |
Alcohol-based solution of chlorhexidine 0.5% chlorhexidine in 70% alcohol solution for ‘preoperative skin disinfection prior to minor surgical procedures’ and 2.0% chlorhexidine in 70% alcohol applicators for ‘disinfection of the skin prior to invasive medical procedures. |
|
Alternative if the surgical site is next to a mucous membrane |
Aqueous solution of chlorhexidine 4.0% aqueous chlorhexidine for ‘preoperative and postoperative skin antisepsis for patients undergoing elective surgery’; however, relevant instructions were limited to use as a body wash to be used before the person enters the operating theatre. |
|
Alternative if chlorhexidine is contraindicated |
Alcohol-based solution of povidone-iodine 10% povidone-iodine alcoholic solution for ‘topical application’. 10% povidone-iodine (Betadine Alcoholic solution) was licensed for ‘antiseptic skin cleanser for major and minor surgical procedures. |
|
If both an alcohol- based solution and chlorhexidine are unsuitable |
Aqueous solution of povidone-iodine 7.5% povidone-iodine surgical scrub solution for disinfecting the site of incision prior to elective surgery’ and 7.5% povidone-iodine (Betadine surgical scrub) for ‘preoperative preparation of patients’ skin’. 10% iodine antiseptic solution for ‘disinfection of intact external skin or as a mucosal antiseptic’ and 10% povidone-iodine solution (Standardised Betadine antiseptic solution) for ‘preoperative and postoperative antiseptic skin cleanser for major and minor surgical procedures. |
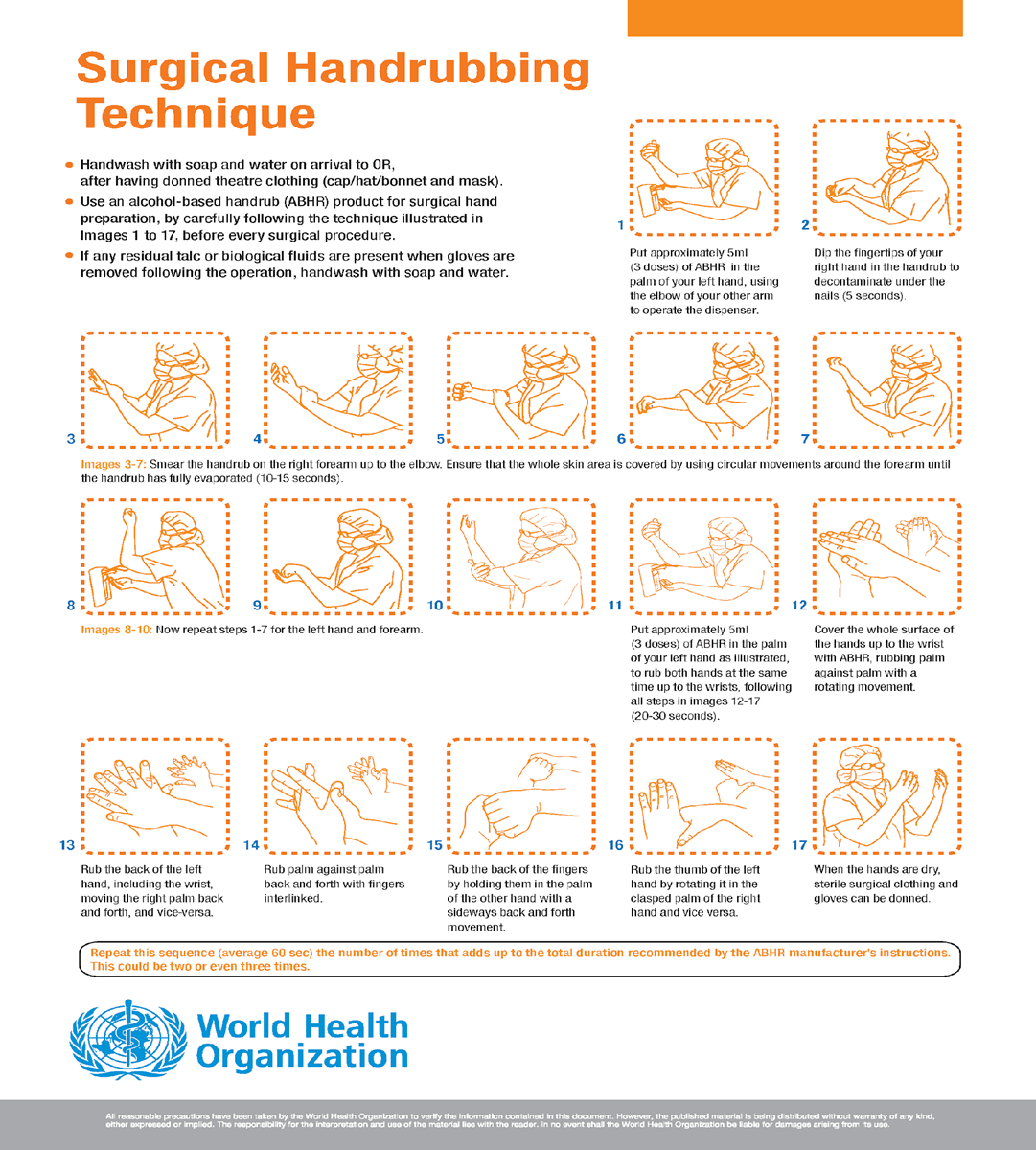
Annex2. Surgical Hand rubbing Technique, World Health Organization
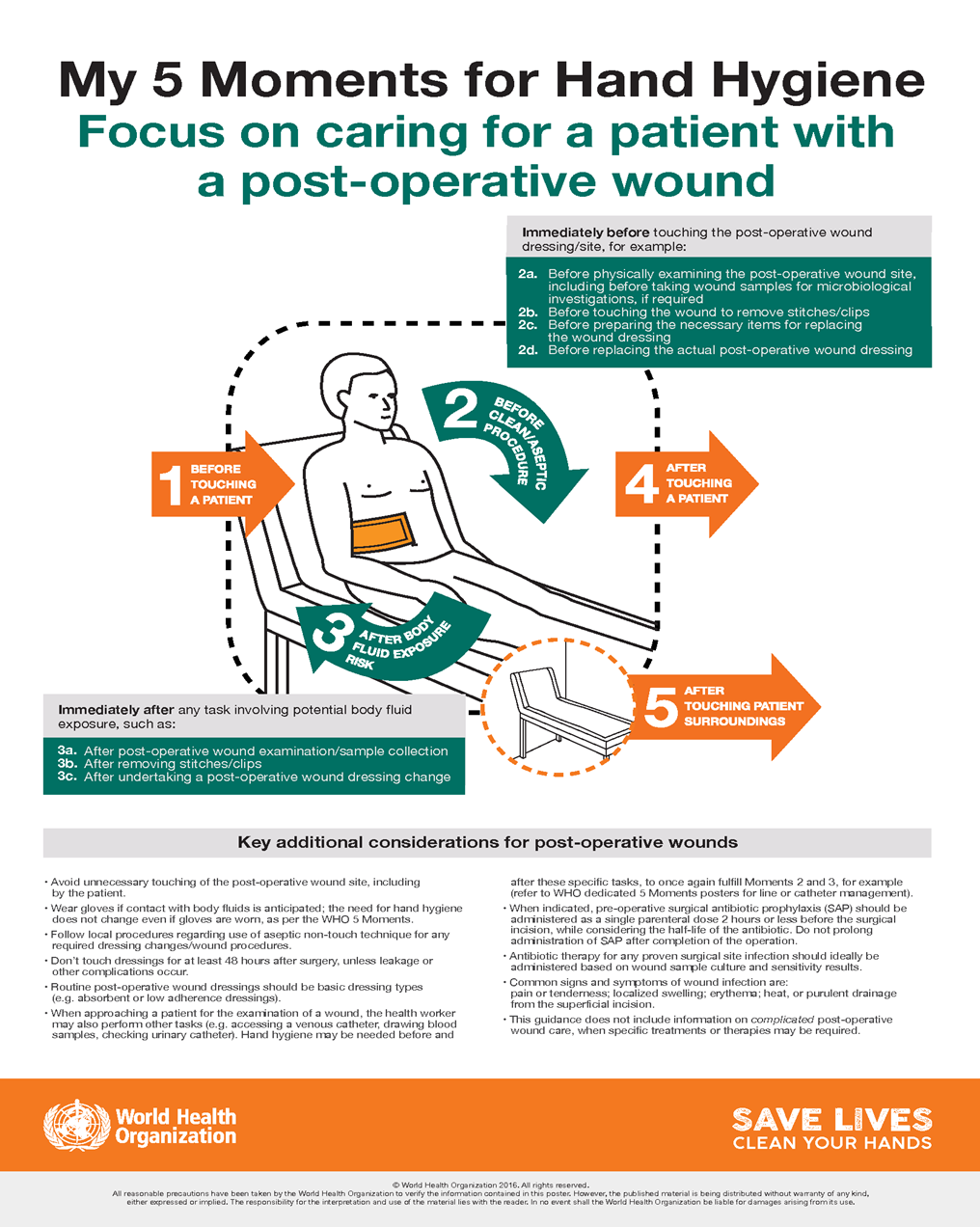
Annex 3. The 5 Moments for Hand Hygiene for a patient with post- operative wound, World Health Organization
- References
1. Calderwood MS, Anderson DJ, Bratzler DW, Dellinger EP, Garcia-Houchins S, Maragakis LL, et al. Strategies to prevent surgical site infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2023;44(5):695–720. doi:10.1017/ice.2023.67
2. Sartelli M. Guidelines for the prevention of surgical site infections. How to implement them. In: Sartelli M, Coimbra R, Pagani L, Rasa K, editors. Infections in Surgery. Hot Topics in Acute Care Surgery and Trauma. Cham: Springer; 2021. p. 77–86. doi:10.1007/978-3-030-62116-2_5
3. European Centre for Disease Prevention and Control. Surveillance of surgical site infections and prevention indicators in European hospitals – HAI-Net SSI protocol, version 2.2. Stockholm: ECDC; 2017.
4. Allegranzi B, Bischoff P, de Jonge S, Kubilay NZ, Zayed B, Gomes SM, et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e288–303.
5. Allegranzi B, Bischoff P, de Jonge S, Kubilay NZ, Zayed B, Gomes SM, et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e276–87.
6. World Health Organization. Global guidelines for the prevention of surgical site infection. Geneva: WHO; 2016 [last accessed 2025 Jun]. Available from: https://apps.who.int/iris/handle/10665/250680
7. National Institute for Health and Care Excellence (NICE) guideline, Surgical site infections: prevention and treatment, updated 2020