the Management of Diverticular Disease
| Site: | EHC | Egyptian Health Council |
| Course: | General surgery Guidelines |
| Book: | the Management of Diverticular Disease |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:02 AM |
Description
"last update: 9 March 2026" Download Guideline
- Executive summary
This guideline offers evidence-based recommendations on the targeted levels of Clinical practice guidelines and provide healthcare professionals with practical guidance on the diagnosis and treatment of diverticular disease and its complications.
· Modification of dietary habits, lifestyle, body weight and medications are recommended to decrease the development of diverticulosis as they are risk factors, (Strong recommendation).
· We recommend treatment of the first attack of acute complicated diverticulitis thoroughly as the incidence of complications and mortality is higher, (Strong recommendation).
· We recommend suspecting acute diverticulitis on the basis of problem-specific history and physical examination and appropriate laboratory evaluation, (Strong recommendation).
· We recommend against depending solely on the clinical findings to judge the severity of the disease, (Strong recommendation).
· We recommend CECT scan of the abdomen and pelvis as the most appropriate initial imaging modality in the assessment of suspected diverticulitis, (Strong recommendation).
· We advise performing ultrasound and MRI in the initial evaluation of a patient with suspected acute diverticulitis, as a useful alternatives, when CT imaging is contraindicated, (Conditional recommendation).
· Tobacco cessation, reduced meat intake, physical activity and weight loss are recommended interventions to potentially reduce the risk of diverticulitis, (Strong recommendation).
· We advise against dietary restrictions and bed rest in acute stage of diverticulitis, (Conditional recommendation).
· For patients tolerating oral intake, we advise outpatient treatment of uncomplicated diverticulitis in the absence of sepsis, significant comorbidity and immunosuppression, (Conditional recommendation).
· We advise treatment with antibiotics for patients with radiological signs of complicated diverticulitis, (Conditional recommendation).
· Antibiotic treatment should be offered for immunocompromised patients and patients with sepsis, (Strong recommendation).
· We recommend against the use of amino salicylate to prevent recurrent AD, (Strong recommendation).
· We advise against endoscopic follow-up for patients with symptom-free recovery after a single episode of CT verified uncomplicated diverticulitis, (Conditional recommendation).
· For patients treated without resection for acute diverticulitis, we advise follow up with endoscopic examination of the colon at least 6 weeks after the acute episode, if not done within the last 3 years, (Conditional recommendation).
· Image-guided percutaneous drainage is recommended for stable patients with diverticular abscesses, (Strong recommendation).
· Immediate surgery is advised in hemodynamically unstable or septic patients, (Conditional recommendation).
· Urgent abdominal exploration is recommended for patients with diffuse peritonitis or for those in whom non-operative management of acute diverticulitis fails, (Strong recommendation).
· We recommend against elective surgery to prevent complicated disease, irrespective of the number of previous attacks, (Strong recommendation).
· We advise against colonic resection in symptomatic patients without radiological or endoscopic signs of ongoing inflammation, stenosis or fistula, (Conditional recommendation).
· After successful non-operative treatment of a diverticular abscess, elective resection should be recommended, (Strong recommendation).
· The decision for elective resection after an acute episode of diverticulitis in immunocompromised and younger patients is the same as in other patients, (Conditional recommendation).
· When expertise is available, a minimally invasive approach to colectomy for diverticulitis is recommended, (Strong recommendation).
· In patients with purulent or feculent peritonitis, colectomy, (open or laparoscopic) is recommended over laparoscopic lavage, (Strong recommendation).
· The extent of elective resection should include the entire sigmoid colon with margins of healthy colon and rectum, (Strong recommendation).
· In the emergency setting, we advise to focus on the control of sepsis and resecting the perforated segment, (Conditional recommendation).
· Elective colectomy, (open or laparoscopic) is recommended for patients with diverticulitis complicated by fistula, persistent abscesses, obstruction, or stricture, (Strong recommendation).
- Recommendations
Section 1: Risk factors for diverticulosis, diverticulitis and its complications:
· Modification of dietary habits, lifestyle, body weight and medications are recommended to decrease the development of diverticulosis as they are risk factors, (Strong recommendation, moderate certainty evidence, (9)).
· We recommend treatment of the first attack of acute complicated diverticulitis thoroughly as the incidence of complications and mortality is higher, (Strong recommendation, moderate certainty evidence, (9)).
Section 2: Diagnosis of diverticulitis:
· We recommend suspecting acute diverticulitis on the basis of problem-specific history and physical examination and appropriate laboratory evaluation, (Strong recommendation, moderate certainty evidence, (10)).
· We recommend against depending solely on the clinical findings to judge the severity of the disease, (Strong recommendation, moderate certainty evidence, (9)).
· We recommend CECT scan of the abdomen and pelvis as the most appropriate initial imaging modality in the assessment of suspected diverticulitis, (Strong recommendation, moderate certainty evidence, (10)).
· We advise performing ultrasound and MRI in the initial evaluation of a patient with suspected acute diverticulitis, as a useful alternatives, when CT imaging is contraindicated, (Conditional recommendation, low certainty evidence, (10)).
Section 3: Non-operative treatment of acute diverticulitis:
· Tobacco cessation, reduced meat intake, physical activity and weight loss are recommended interventions to potentially reduce the risk of diverticulitis, (Strong recommendation, high certainty evidence, (10)).
· We advise against dietary restrictions and bed rest in acute stage of diverticulitis, (Conditional recommendation, low certainty evidence, (9)).
· For patients tolerating oral intake, we advise outpatient treatment of uncomplicated diverticulitis in the absence of sepsis, significant comorbidity and immunosuppression, (Conditional recommendation, moderate certainty evidence, (9)).
· We advise treatment with antibiotics for patients with radiological signs of complicated diverticulitis, (Conditional recommendation, low certainty evidence, (9)).
· Antibiotic treatment should be offered for immunocompromised patients and patients with sepsis, (Strong recommendation, high certainty evidence, (9)).
· We recommend against the use of amino salicylate to prevent recurrent AD, (Strong recommendation, moderate certainty evidence, (10)).
Section 4: Follow-up after an episode of uncomplicated and complicated diverticulitis:
· We advise against endoscopic follow-up for patients with symptom-free recovery after a single episode of CT verified uncomplicated diverticulitis, (Conditional recommendation, low certainty evidence, (9)).
· For patients treated without resection for acute diverticulitis, we advise follow up with endoscopic examination of the colon at least 6 weeks after the acute episode, if not done within the last 3 years, (Conditional recommendation, low certainty evidence, (9)).
Section 5: Role of percutaneous drainage for patients with a diverticular abscess:
· Image-guided percutaneous drainage is recommended for stable patients with diverticular abscesses, (Strong recommendation, moderate certainty evidence, (10)).
Section 6: Indications for abdominal exploration in patients with acute diverticulitis:
· Immediate surgery is advised in hemodynamically unstable or septic patients, (Conditional recommendation, low certainty evidence, (9)).
· Urgent abdominal exploration is recommended for patients with diffuse peritonitis or for those in whom non-operative management of acute diverticulitis fails, (Strong recommendation, moderate certainty evidence, (10)).
· We recommend against elective surgery to prevent complicated disease, irrespective of the number of previous attacks, (Strong recommendation, moderate certainty evidence, (9)).
· We advise against colonic resection in symptomatic patients without radiological or endoscopic signs of ongoing inflammation, stenosis or fistula, (Conditional recommendation, low certainty evidence, (9)).
· After successful non-operative treatment of a diverticular abscess, elective resection should be recommended, (Strong recommendation, moderate certainty evidence, (10)).
· The decision for elective resection after an acute episode of diverticulitis in immunocompromised and younger patients is the same as in other patients, (Conditional recommendation, low certainty evidence, (9)).
Section 7: Surgical treatment of diverticulitis:
· When expertise is available, a minimally invasive approach to colectomy for diverticulitis is recommended, (Strong recommendation, high certainty evidence, (10)).
· In patients with purulent or feculent peritonitis, colectomy, (open or laparoscopic) is recommended over laparoscopic lavage, (Strong recommendation, high certainty evidence, (10)).
· The extent of elective resection should include the entire sigmoid colon with margins of healthy colon and rectum, (Strong recommendation, moderate certainty evidence, (10)).
· In the emergency setting, we advise to focus on the control of sepsis and resecting the perforated segment, (Conditional recommendation, low certainty evidence, (9)).
Section 8: Surgery of persisting abscesses and fistulas:
· Elective colectomy, (open or laparoscopic) is recommended for patients with diverticulitis complicated by fistula, persistent abscesses, obstruction, or stricture, (Strong recommendation, moderate certainty evidence, (10)).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for
developing this guideline.
Chair of GDG: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GDG: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AD |
Acute Diverticulitis |
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
ASCRS |
American Society of Colon and Rectal Surgeons |
|
CECT |
Contrast Enhanced Computerized Tomography. |
|
CRC |
Colorectal Carcinoma |
|
CRP |
C Reactive Protein |
|
CT |
Computerized Tomography. |
|
DD |
Diverticular Disease |
|
ESCP |
European Society of Coloproctology |
|
GDG |
Guideline Development Group. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation |
|
IBD |
Inflammatory Bowel Disease |
|
MRI |
Magnetic resonance imaging |
|
QoL |
Quality of life |
|
SUDD |
Symptomatic Uncomplicated Diverticular Disease |
- Glossary
Definition of diverticular disease and classification
We found that there is a great importance to establish clear definitions in the area of diverticular disease. Numerous classifications and modifications describe the various stages of diverticular disease. The first widely used classification by Hinchey was intended as an intra-operative stratification of perforated diverticulitis with abscess or peritonitis enabling surgeons to adjust the surgical approach. It was later modified to preoperative use, incorporating CT findings, (1).
Diverticulosis versus diverticular disease
Diverticulosis of the colon (existence of false diverticula – outpouchings of mucosa and serosa through openings in the muscular layer of the bowel) develops in the majority of individuals in western countries with increasing age and usually remains asymptomatic. Diverticulosis per se should not therefore be considered a disease. The term diverticular disease implies that there are symptoms related to the diverticula, (2).
Symptomatic uncomplicated diverticular disease (SUDD)
The term symptomatic uncomplicated diverticular disease (SUDD) is used in some countries for patients with diverticula who experience abdominal symptoms (e.g. abdominal pain and bloating) and changes in bowel habit (e.g. diarrhea, constipation or alternating bowel habit) in the absence of inflammation. However, the term has not found general acceptance and a uniform definition does not exist. Currently, there is little evidence on how to manage SUDD, (1).
Diverticulitis
The term diverticulitis describes a peri-diverticular inflammation of the bowel wall and usually the surrounding tissue. Diverticulitis can be acute or chronic and complicated or uncomplicated with possible complications including abscess, perforation, fistulas, obstruction and bleeding. The severity of acute diverticulitis, mainly determined by cross-sectional imaging (CT scan, ultrasound) and laboratory tests (C-reactive protein), is decisive and guides management and treatment. In general, uncomplicated acute diverticulitis is differentiated from complicated acute diverticulitis. The cut-off is poorly defined but depends on the degree of inflammation, (3).
Acute uncomplicated diverticulitis is inflammation in a diverticula-bearing bowel segment and the surrounding tissue without signs of perforation (extraluminal air) or abscess formation, (4).
Acute complicated diverticulitis: Typical complications of acute diverticulitis occur if the inflammatory process extends beyond the colonic wall. However, peridiverticulitis alone is not considered complicated disease. A covered perforation with air bubbles in proximity to the bowel, intra-abdominal abscess adjacent to the inflamed segment (Hinchey Ib, according to Wasvary) or distant (Hinchey II) and free perforations with purulent or faecal peritonitis (Hinchey III and IV) represent the major manifestations of acute complicated diverticulitis, (4), (tables 1 & 2).
Acute complicated diverticulitis comes with considerable mortality. Mortality risk increases even more in the case of free perforations with peritonitis. Both the risk of a subsequent free perforation and the risk of death decrease with the number of previous episodes. The first episode of complicated diverticulitis is by far the most dangerous, (4).
Chronic diverticulitis: If an acute diverticulitis does not resolve completely, chronic diverticulitis can develop. Wall thickening or chronic mucosal inflammation in the absence of stenosis is called chronic uncomplicated diverticulitis. Complicated chronic diverticulitis may progress to include either stenotic disease, which may lead to acute bowel obstruction, or fistulation most commonly to the urinary tract, or both, (4).
Diverticular bleeding: According to ESCP statement, diverticular bleeding is reported to account for about 35% of painless lower gastrointestinal bleeding and occurs in up to 50% of elderly patients with diverticulosis. Frequently, the bleeding site cannot be identified, and coexisting diverticula may then falsely be reported as the bleeding cause. Diverticular bleeding is arterial and occurs from rupture of the intramural branches of the marginal artery at the dome or neck of the diverticulum. Trauma from mechanical or chemical causes within the lumen of the diverticulum leads to injury to the penetrating vessels and bleeding. Histopathological examination of diverticular bleeding sites has shown absence of diverticulitis, but bleeding may occur during inflammation as well. If surgery is required, precise localization of the bleeding site is crucial for any surgical procedure. Colonic resections in patients with diverticular bleeding and an unclear localization have shown a postoperative mortality of 43% in comparison to 7% in patients with defined bleeding localization. There are separate guidelines for the management of lower gastrointestinal bleeding which is therefore not part of this guideline, (5).
- Introduction
By far the majority of individuals with diverticulosis remain asymptomatic throughout life, (6). Therefore, the incidence of diverticulosis is difficult to estimate.
Diverticulosis and associated clinical problems are most likely to occur in older age groups. However, although there is quite a variability of frequency rates for diverticulitis in the literature, there is some evidence that the incidence of diverticulitis has risen over the last years particularly in younger adults and women (younger than 45). There are almost no population-based data. Nearly all studies refer to the number of hospital admissions. An Italian study found an overall rate of 48 hospital admissions for acute diverticular disease per 100 000 inhabitants in 2015, and a yearly increase of over 3% from 2008. Interestingly, the age-specific rate was constant for older ages and there was only a slight increase for the younger age groups; thus, some of the increase of the overall rate might be attributed to the aging population. The overall rate of hospital admissions for acute diverticular disease per 100 000 hospitalizations was 248 with an annual increase of 7.5% from 190 in 2008 to 310 in 2015, (7). From the USA, a prevalence of 92/100 000 persons with a preponderance of women has been report, (8).
Currently several national guidelines are available, most of which are not updated. The guidelines committee of GGS decided in 2025 to develop a national guideline for the management of diverticular disease and its complications, acknowledging that it will be a compromise of European society of coloproctology (ESCP), (9), and American Society of Colon and Rectal Surgeons (ASCRS) guidelines, (10), and different accessibilities to healthcare and medical procedures in different healthcare systems, (11 & 12).
- Scope and purpose
The scope of these guidelines is to diagnose diverticular disease and its complications and to manage these problems accurately and without any hesitation.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to
improve the quality of medical care and surgical service, to provide the best clinical practice to
our patients, and finally to reduce the cost of medical service.
- Target audience
The principle targeted audiences are the practicing surgeons, however, gastroenterologists, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
· Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Specific range of dates for publication (using Guidelines published or updated in 2020 and later)
· Selecting peer reviewed publications only
· Selecting guidelines written in English language
· Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
· The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the European Society of Coloproctology guidelines, 2020,(9) and the American Society of Colon and Rectal Surgeons clinical practice guidelines 2020,(10).
➡️Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (tables 3& 4).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
➡️Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
➡️When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research needs
1. The prevalence of DD in Egypt among different age groups.
2. The need and timing of surgery after resolution of acute diverticulitis
- Clinical indicators for monitoring
1. Documentation of the clinical symptoms and signs.
2. CT.
3. Colonoscopy.
4. Documentation of the type of treatment, (medical, aspiration, surgical).
- Updating of the guideline
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about diverticulosis and diverticular disease. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1 Hinchy classification, (1).
|
Stage |
Description |
|
I |
Pericolic abscess or phlegmon |
|
II |
Pelvic, distant intraabdominal, or retroperitoneal abscess |
|
III |
Generalized purulent peritonitis |
|
IV |
Generalized fecal peritonitis |
Table 2 Modified Hinchy classification (Wasvary), (1).
|
Stage |
Description |
|
0 |
Mild clinical acute diverticulitis |
|
Ia |
confined pericolic inflammation phlegmon |
|
Ib |
Pericolic or mesocolic abscess |
|
II |
Pelvic, distant intraabdominal, or retroperitoneal abscess |
|
III |
Generalized purulent peritonitis |
|
IV |
Generalized fecal peritonitis |
Table 3. Quality and Significance of the four levels of evidence in GRADE:
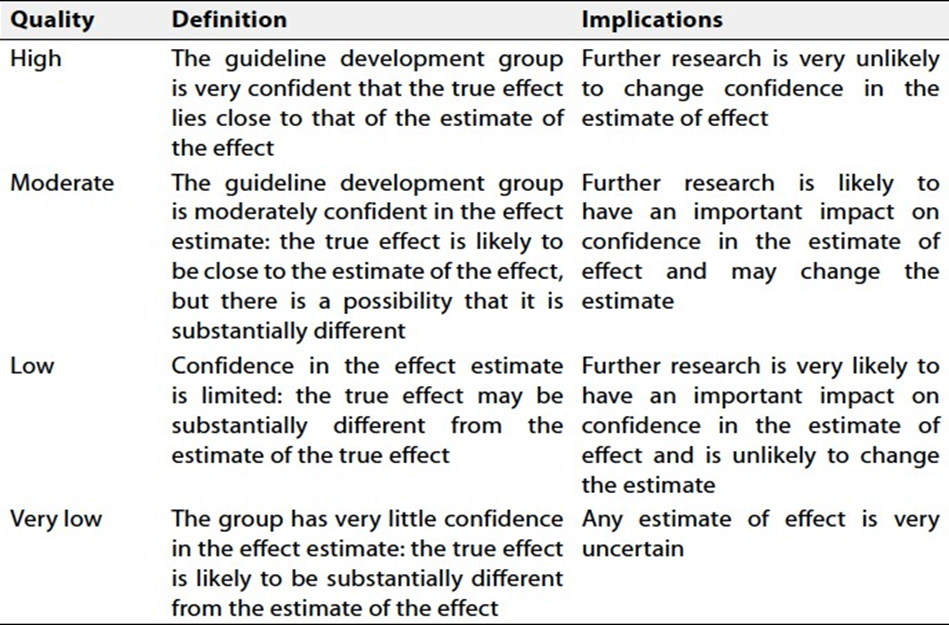
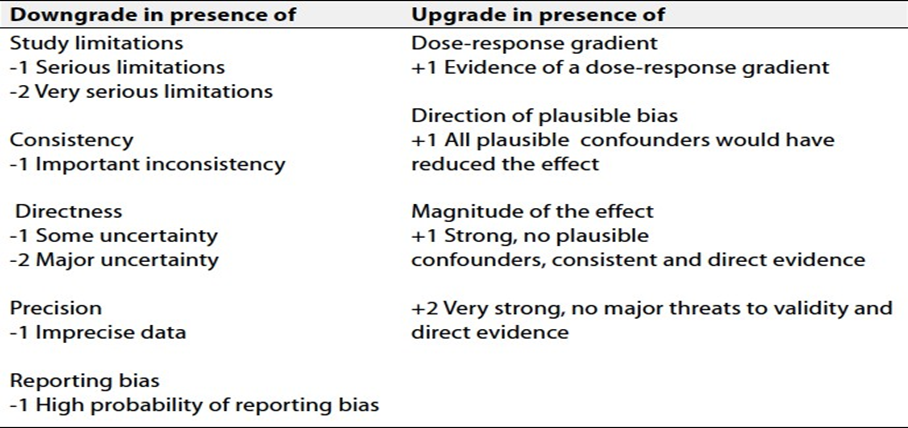
Table 4. Factors that determine How to upgrade or downgrade the quality of evidence.
- References
1 Wasvary H, Turfah F, Kadro O, Beauregard W. Same hos- pitalization resection for acute diverticulitis. Am Surg 1999; 65: 632–5; discussion 636.
2 Rustom LBO, Sharara AI. The natural history of colonic diverticulosis: much ado about nothing? Inflamm Intest Dis 2018; 3: 69–74.
3 Strate LL, Morris AM. Epidemiology, pathophysiology, and treatment of diverticulitis. Gastroenterology 2019; 156, 1282–98. e1281.
4 Wasvary H, Turfah F, Kadro O, Beauregard W. Same hos- pitalization resection for acute diverticulitis. Am Surg 1999; 65: 632–5; discussion 636.
5 Mohammed Ilyas MI, Szilagy EJ. Management of diver- ticular bleeding: evaluation, stabilization, intervention, and recurrence of bleeding and indications for resection after control of bleeding. Clin Colon Rectal Surg 2018; 31: 243– 50.
6 Pfutzer RH, Kruis W. Management of diverticular disease. Nat Rev Gastroenterol Hepatol 2015; 12: 629–38.
7 Binda GA, Mataloni F, Bruzzone M et al. Trends in hospital admission for acute diverticulitis in Italy from 2008 to 2015. Tech Coloproctol 2018; 22: 597–604.
8 Wheat CL, Strate LL. Trends in hospitalization for diverticulitis and diverticular bleeding in the United States from 2000 to 2010. Clin Gastroenterol Hepatol 2016; 14, 96–103. e101.
9 Schultz JK, Azhar N, Binda GA et al. European Society of Coloproctology: guidelines for management of diverticular disease of the colon. Colorectal Disease 2020; 22,5-28.
10 Jason H, Hardiman K, Lightner A, Stocchi S, Feingold D. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Left Sided Colonic Diverticulitis. Diseases of the Colon & Rectum 2020; 63(6), 728-47.
11 Kruis W, Germer CT, Bohm S et al. German guideline diverticular disease/diverticulitis Part I: Methods, pathogenesis, epidemiology, clinical characteristics (definitions), natural course, diagnosis and classification. United European Gastroenterol J Wily. AWMF online 2022; 1-17.
12 Carabotti M, Sgamato C, Amato A et al. Italian guidelines for the diagnosis and management of colonic diverticulosis and diverticular disease. Digestive and Liver Disease 2024; 56, 1989-2003.