Management of Crohn’s Disease in Adults
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحه عامه |
| كتاب: | Management of Crohn’s Disease in Adults |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:02 AM |
الوصف
"last update: 10 March 2026" Download Guideline
- Executive summary
These guidelines offer evidence-based recommendations on the targeted levels of clinical practice guidelines and provide healthcare professionals with practice guidance on the surgical management of Crohn’s disease and its complications.
· Surgical treatment for CD must consider disease location, severity of symptoms, clinical manifestations, and nutritional status. The decision must be the result of a common agreement between gastroenterologists, surgeons, and patients, (Good practice statement).
· We recommend for patients who demonstrate an inadequate response to, develop complications from, or are non-adherent with medical therapy, they should typically be considered for surgery, (Strong recommendation).
· We advise performing a de-functioning stoma for non-acute refractory CD colitis, to delay or avoid the need for colectomy, (Good practice statement).
· We advise conservative treatment following successful percutaneous, image-guided drainage of an intra-abdominal abscess in carefully selected cases. A low threshold for surgery is advised in the event of medically refractory cases, (Conditional recommendation).
· We recommend for patients with severe acute colitis who do not adequately respond to medical therapy or who have signs or symptoms of impending or actual perforation to undergo surgery, (Strong recommendation).
· In localized ileocaecal CD, we advise performing surgical treatment as a therapeutic option, (Conditional recommendation).
· In cases of recurrent ileocaecal CD after initial treatment with steroids and/or immunosuppressants, surgical resection or biological therapy is recommended, (Strong recommendation).
· We advise performing endoscopic dilation for patients with short-segment, non-inflammatory, symptomatic small bowel or anastomotic strictures when feasible, (Conditional recommendation).
· We recommend surgical intervention for patients with symptomatic small-bowel or anastomotic strictures that are not amenable to medical therapy and/or endoscopic dilation, (Strong recommendation).
· We recommend surgical resection for patients with strictures of the colon that cannot be adequately surveyed endoscopically, (Strong recommendation).
· We advise the use of cross-sectional imaging tests when CD complications result in abdominal abscess formation, especially when the condition is complex, recurrent, or associated with previous surgery. For these cases, magnetic resonance imaging (MRI) is better, due to its sensitivity and specificity, (Conditional recommendation).
· We recommend surgical resection of the perforated segment for patients with a free perforation, (Strong recommendation).
· We advise managing of patients with penetrating Crohn’s disease with abscess formation with antibiotics with or without drainage followed by interval elective resection or medical therapy depending on the clinical situation and patient preferences, (Conditional recommendation).
· We recommend surgical intervention for patients with enterocutaneous fistulas with short tracts and high output. However, proper timing of surgery must be decided after full preoperative optimization, including nutritional status. Caution must be taken in patients previously submitted to small bowel resection(s), at risk for intestinal failure, (Strong recommendation).
· We recommend for stable patients with gastrointestinal hemorrhage to be evaluated and treated by endoscopic and/or interventional radiologic techniques. Unstable patients, despite resuscitation efforts, should typically undergo operative exploration, (Strong recommendation).
· We recommend endoscopic surveillance at regular intervals for patients with long-standing Crohn’s colitis involving at least one-third of the colon or more than 1 segment, (Strong recommendation).
· We recommend endoscopic surveillance for patients with visible dysplasia that is completely excised endoscopically. If dysplasia is not amenable to endoscopic excision, is also found in the surrounding flat mucosa, or is multifocal, or if colorectal adenocarcinoma is diagnosed, total colectomy or total proctocolectomy is typically recommended, (Strong recommendation).
· We recommend for patients with invisible, indefinite dysplasia, they should typically be referred to an experienced endoscopist for repeat colonoscopy using enhanced imaging with repeat random biopsies within 3 to 12 months, (Strong recommendation).
· We advise for patients with invisible, low- or high-grade dysplasia on routine surveillance colonoscopy, to be referred to an experienced endoscopist for high-definition colonoscopy with chromoendoscopy with repeat random biopsies within 3 to 6 months. Patients found to have invisible, low- or high-grade dysplasia at the time of high-definition colonoscopy with chromoendoscopy should typically undergo total colectomy or proctocolectomy, (Conditional recommendation).
· We recommend biopsy from any suspicious lesions (eg, mass, ulcer) identified in patients with Crohn’s disease, especially when considering small-bowel or colonic strictureplasty, (Strong recommendation).
· We recommend for patients with symptomatic disease of the stomach or duodenum despite medical therapy to consider for endoscopic dilation, bypass, or strictureplasty, (Strong recommendation).
· We advise performing strictureplasty for stenosis of the second and third duodenal portions, as it has better outcomes. Duodenal resection or pancreatoduodenectomy are options used as a last therapeutic resource, (Conditional recommendation).
· We recommend for patients with medically refractory disease isolated to the jejunum, ileum, or ileocolon without existing or anticipated short-bowel syndrome, to undergo escalation of medical therapy or resection of the affected bowel, ideally, as determined by a multidisciplinary team, (Strong recommendation).
· We recommend strictureplasty for patients undergoing an operation with multifocal disease, (Strong recommendation).
· We recommend performing a total abdominal colectomy with end ileostomy, as the procedure of choice, for emergency surgery in Crohn’s colitis is, (Strong recommendation).
· For patients with colonic disease and rectal sparing who proceed with elective surgery, we recommend performing segmental colectomy for single-segment disease or total colectomy for more extensive disease, (Strong recommendation).
· For patients undergoing elective surgery for rectal disease, we recommend performing total proctocolectomy with end ileostomy or proctectomy with creation of a colostomy, (Strong recommendation).
· We recommend elective bowel resection over emergency surgery in patients with CD, (Strong recommendation).
· We recommend control of sepsis prior to abdominal surgery for CD, (Strong recommendation).
· Preoperative high-dose glucocorticoids increase the risk of postoperative infectious complications and we recommend weaning glucocorticoids before surgical intervention. Immunomodulators are not associated with increased risk of postoperative infectious complications and do not typically need to be held before surgery, (Strong recommendation).
· We do not advise to delay surgical intervention, based on monoclonal antibody therapy alone, (Conditional recommendation).
· Preoperative nutritional support for patients with malnutrition may decrease postoperative morbidity and pre-operative optimization is advised, followed by re-assessment of the patient for surgical intervention, (Conditional recommendation).
· Smoking cessation is recommended to reduce postoperative morbidity in patients with Crohn’s disease, (Strong recommendation).
· We advise performing CD surgery is in high-volume IBD centers, (Conditional recommendation).
· We recommend when feasible, a minimally invasive approach, such as laparoscopy, is preferred, particularly for primary procedures for ileocolonic CD. Nevertheless, it may not always be feasible in patients with recurrent or complex disease, (Strong recommendation).
· We advise a de-functioning stoma for non-acute refractory CD colitis, to delay or avoid the need for colectomy, (Good practice statement).
· We recommend a diverting ileostomy when performing ileocolectomy in patients who have Crohn’s disease with multiple risk factors, (Strong recommendation).
· We advise performing stapled side-to-side anastomoses in small bowel or ileocolic resections for CD, (Conditional recommendation, moderate certainty evidence, (8)).
· We advise performing the Kono-S anastomosis as an alternative surgical approach to other types of anastomoses after ileocaecal resection, (Conditional recommendation).
· We recommend strictureplasty as an alternative treatment option to resection in small-bowel CD, (Strong recommendation).
· We advise performing segmental colectomy in selected cases of colonic CD, (Conditional recommendation).
· After surgery for CD, the patients are recommended to be on medical therapy to treat residual active disease or to maintain disease remission, (Strong recommendation).
· We recommend endoscopic surveillance within 6–12 months after surgical resection in CD, (Strong recommendation).
· We recommend extended thromboembolism prophylaxis following hospital discharge after CD surgery, (Strong recommendation).
· We recommend management of symptomatic anorectal fistula associated with Crohn’s disease, with a combination of surgical and medical approaches, (Strong recommendation).
· We recommend against surgical treatment of asymptomatic fistulae in patients with Crohn’s disease, (Strong recommendation)
· We recommend draining Setons in the multimodality therapy of fistulizing anorectal CD and may be used for long-term disease control, (Strong recommendation)
· Endorectal advancement flaps and the LIFT procedure are recommended to treat fistula-in-ano associated with CD, (Strong recommendation).
· We advise to treat symptomatic, simple, single, low anal fistulae in patients with Crohn’s disease, by lay-open fistulotomy, (Conditional recommendation).
· Fecal diversion or proctectomy, is recommended for patients with uncontrolled symptoms from complex anorectal fistulizing CD, (Strong recommendation).
- Recommendations
Section 1: Operative indications:
1. Medically refractory disease:
· Surgical treatment for CD must consider disease location, severity of symptoms, clinical manifestations, and nutritional status. The decision must be the result of a common agreement between gastroenterologists, surgeons, and patients, (Good practice statement).
· We recommend surgical treatment for patients who demonstrate an inadequate response to, develop complications from, or are non-adherent with medical therapy, (Strong recommendation, low certainty evidence, (1)).
· We advise performing a de-functioning stoma for non-acute refractory CD colitis, to delay or avoid the need for colectomy, (Good practice statement).
· We advise conservative treatment following successful percutaneous, image-guided drainage of an intra-abdominal abscess in carefully selected cases, (Conditional recommendation, low certainty evidence, (8)).
2. Inflammation:
· We recommend for patients with severe acute colitis who do not adequately respond to medical therapy or who have signs or symptoms of impending or actual perforation to undergo surgery, (Strong recommendation, low certainty evidence, (1)).
· In localized ileocaecal CD, we advise performing surgical treatment as a therapeutic option, (Conditional recommendation, low certainty evidence, (9)).
· In cases of recurrent ileocaecal CD after initial treatment with steroids and/or immunosuppressants, surgical resection is recommended, (Strong recommendation, low certainty evidence, (9)).
· In cases of recurrent ileocaecal CD after initial treatment with steroids and/or immunosuppressants, biological therapy is an alternative option, (Conditional recommendation, low certainty evidence, (9)).
3. Stricture:
· We advise performing endoscopic dilation for patients with short-segment, non-inflammatory, symptomatic small bowel or anastomotic strictures when feasible, (Conditional recommendation, low certainty evidence, (1)).
· We recommend surgical intervention for patients with symptomatic small-bowel or anastomotic strictures that are not amenable to medical therapy and/or endoscopic dilation, (Strong recommendation, low certainty evidence, (1)).
· We recommend surgical resection for patients with strictures of the colon that cannot be adequately surveyed endoscopically, (Strong recommendation, low certainty evidence, (1)).
4. Penetrating disease:
· We advise the use of cross-sectional imaging tests when CD complications result in abdominal abscess formation, especially when the condition is complex, recurrent, or associated with previous surgery. For these cases, magnetic resonance imaging (MRI) is better, due to its sensitivity and specificity, (Conditional recommendation, low certainty evidence, (9)).
· We recommend surgical resection of the perforated segment for patients with a free perforation, (Strong recommendation, moderate certainty evidence, (1)).
· We advise managing of patients with penetrating Crohn’s disease with abscess formation with antibiotics with or without drainage followed by interval elective resection or medical therapy depending on the clinical situation and patient preferences, (Conditional recommendation, moderate certainty evidence, (1)).
· We recommend surgical intervention for patients with enterocutaneous fistulas with short tracts and high output. However, proper timing of surgery must be decided after full preoperative optimization, including nutritional status. Caution must be taken in patients previously submitted to small bowel resection(s) because of the risk of intestinal failure, (Strong recommendation, low certainty evidence, (9)).
5. Hemorrhage:
· We recommend for stable patients with gastrointestinal hemorrhage to be evaluated and treated by endoscopic and/or interventional radiologic techniques. Unstable patients, despite resuscitation efforts, should typically undergo operative exploration, (Strong recommendation, low certainty evidence, (1)).
6. Colorectal dysplasia and cancer:
· We recommend endoscopic surveillance at regular intervals for patients with long-standing Crohn’s colitis involving at least one-third of the colon or more than 1 segment, (Strong recommendation, moderate certainty evidence, (1)).
· We recommend endoscopic surveillance for patients with visible dysplasia that is completely excised endoscopically. If dysplasia is not amenable to endoscopic excision, is also found in the surrounding flat mucosa, or is multifocal, or if colorectal adenocarcinoma is diagnosed, total colectomy or total proctocolectomy is typically recommended, (Strong recommendation, moderate certainty evidence, (1)).
· We recommend for patients with invisible, indefinite dysplasia, they should typically be referred to an experienced endoscopist for repeat colonoscopy using enhanced imaging with repeat random biopsies within 3 to 12 months, (Strong recommendation, low certainty evidence, (1)).
· We advise for patients with invisible, low- or high-grade dysplasia on routine surveillance colonoscopy, to be referred to an experienced endoscopist for high-definition colonoscopy with chromoendoscopy with repeat random biopsies within 3 to 6 months. Patients found to have invisible, low- or high-grade dysplasia at the time of high-definition colonoscopy with chromoendoscopy should typically undergo total colectomy or proctocolectomy, (Conditional recommendation, moderate certainty evidence, (1)).
· We recommend biopsy from any suspicious lesions (eg, mass, ulcer) identified in patients with Crohn’s disease, especially when considering small-bowel or colonic strictureplasty, (Strong recommendation, low certainty evidence, (1)).
Section 2: Site specific operations:
· We recommend for patients with symptomatic disease of the stomach or duodenum despite medical therapy to consider for endoscopic dilation, bypass, or strictureplasty, (Strong recommendation, low certainty evidence, (1)).
· We advise performing strictureplasty for stenosis of the second and third duodenal portions, as it has better outcomes. Duodenal resection or pancreatoduodenectomy are options used as a last therapeutic resource, (Conditional recommendation, low certainty evidence, (9)).
· We recommend for patients with medically refractory disease isolated to the jejunum, ileum, or ileocolon without existing or anticipated short-bowel syndrome, to undergo escalation of medical therapy or resection of the affected bowel, ideally, as determined by a multidisciplinary team, (Strong recommendation, low certainty evidence, (1)).
· We recommend strictureplasty for patients undergoing an operation with multifocal disease, (Strong recommendation, low certainty evidence, (1)).
· We recommend performing a total abdominal colectomy with end ileostomy, as the procedure of choice, for emergency surgery in Crohn’s colitis, (Strong recommendation, low certainty evidence, (1)).
· For patients with colonic disease and rectal sparing who proceed with elective surgery, we recommend performing segmental colectomy for single-segment disease or total colectomy for more extensive disease, (Strong recommendation, moderate certainty evidence, (1)).
· For patients undergoing elective surgery for rectal disease, we recommend performing total proctocolectomy with end ileostomy or proctectomy with creation of a colostomy, (Strong recommendation, low certainty evidence, (1)).
Section 3: Preoperative considerations:
· We recommend elective bowel resection over emergency surgery in patients with CD, (Strong recommendation, high certainty evidence, (8)).
· We recommend control of sepsis prior to abdominal surgery for CD, (Strong recommendation, moderate certainty evidence, (8)).
· Preoperative high-dose glucocorticoids increase the risk of postoperative infectious complications and we recommend weaning glucocorticoids before surgical intervention. Other immunomodulators are not associated with increased risk of postoperative infectious complications and do not typically need to be held before surgery, (Strong recommendation, low certainty evidence, (1)).
· Preoperative nutritional support for patients with malnutrition may decrease postoperative morbidity and pre-operative optimization is advised, followed by re-assessment of the patient for surgical intervention, (Conditional recommendation, low certainty evidence, (1)).
· Smoking cessation is recommended to reduce postoperative morbidity in patients with Crohn’s disease, (Strong recommendation, low certainty evidence, (1)).
Section 4: Operative considerations:
· We advise performing CD surgery in high-volume tertiary centers, (Conditional recommendation, moderate certainty evidence, (8)).
· Laparoscopy is the preferred option, particularly for primary procedures for ileocolonic CD. Nevertheless, it may not always be feasible in patients with recurrent or complex disease, (Conditional recommendation, moderate certainty evidence, (9)).
· We advise performing a de-functioning stoma for non-acute refractory CD colitis, to delay or avoid the need for colectomy, (Good practice statement).
· We recommend a diverting ileostomy when performing ileocolectomy in patients who have Crohn’s disease with multiple risk factors, (Strong recommendation, moderate certainty evidence, (1)).
· We advise performing stapled side-to-side anastomoses in small bowel or ileocolic resections for CD, (Conditional recommendation, moderate certainty evidence, (8)).
· We advise performing the Kono-S anastomosis as an alternative surgical approach to other types of anastomoses after ileocaecal resection, (Conditional recommendation, moderate certainty evidence, (8)).
· We recommend strictureplasty as an alternative treatment option to resection in small-bowel CD, (Strong recommendation, high certainty evidence, (8)).
· We advise performing segmental colectomy in selected cases of colonic CD, (Conditional recommendation, low certainty evidence, (8)).
Section 5: Postoperative considerations:
· After surgery for CD, patients are recommended to be on medical therapy to treat residual active disease or to maintain disease remission, (Strong recommendation, moderate certainty evidence, (1)).
· We recommend endoscopic surveillance within 6–12 months after surgical resection in CD, (Strong recommendation, high certainty evidence, (8)).
· We recommend thromboembolism prophylaxis following hospital discharge after CD surgery, (Strong recommendation, high certainty evidence, (8)).
Section 6: Perianal Crohn’s disease:
• We recommend management of symptomatic anorectal fistula associated with Crohn’s disease, with a combination of surgical and medical approaches, (Strong recommendation, moderate certainty evidence (10, 11)).
• We recommend against surgical treatment of asymptomatic fistulae in patients with Crohn’s disease, (Strong recommendation, low certainty evidence (10, 11)).
• We recommend draining Setons in the multimodality therapy of fistulizing anorectal CD and may be used for long-term disease control, (Strong recommendation, moderate certainty evidence (10, 11)).
• Endorectal advancement flaps and the LIFT procedure are recommended to treat fistula-in-ano associated with CD, (Strong recommendation, moderate certainty evidence (10, 11)).
• We advise to treat symptomatic, simple, single, low anal fistulae in patients with Crohn’s disease, by lay-open fistulotomy, (Conditional recommendation, low certainty evidence (10, 11)).
• Fecal diversion or proctectomy, is recommended for patients with uncontrolled symptoms from complex anorectal fistulizing CD, (Strong recommendation, moderate certainty evidence (10, 11)).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for developing these guidelines.
Chair of GDG: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GDG: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
CD |
Crohn’s Disease |
|
CT scan LIFT |
Computed Tomography Scan Ligation of intersphinctreric fistula tract. |
|
GIT |
Gastro-Intestinal Tract |
|
GRADE |
Grade of Recommendations, Assessment, Development and Evaluation |
|
GDG |
Guideline Development Group |
|
IBD |
Inflammatory Bowel Disease |
|
IPAA |
Ileal Pouch-Anal Anastomosis |
|
MRI |
Magnetic Resonance Imaging |
|
WHO |
World Health Organization |
- Introduction
Crohn’s disease (CD) is an idiopathic, incurable chronic inflammatory disease of the GI tract. The characteristic transmural inflammation of CD can occur anywhere along the GI tract, resulting in an inflammatory, fibro-stenotic, or penetrating phenotype. Although the degree of symptoms is variable and may wax and wane throughout the disease course, patients can require chronic immunosuppression and operations to treat the disease symptoms, but both are unable to cure the disease, (1).
The incidence and prevalence of Crohn’s disease (CD) is on the rise globally, with increases in incidence ranging from 4% to 15% yearly over the past three decades, (2).
Many different medications and combinations thereof are reshaping clinical practice, and refined surgical techniques, tailored approaches, and a wider acceptance of a surgical alternative benefit patients. Hence, the best possible outcomes are currently achieved within dedicated expert centers providing personalized medicine, (3 & 4).
Although the rate of surgical intervention for medically refractory disease has decreased over the past 6 decades and less emergent surgery is being performed, a meta-analysis of population-based studies reported that rates of surgical intervention for medically refractory disease remain high at 16%, 33%, and 47% at 1, 3, and 5 years from diagnosis, (5 & 6).
After resection, because surgery is not curative, 70% to 90% of patients will have endoscopic recurrence by 1 year and up to 35% of patients will have a repeat intestinal resection within 10 years, (7).
Given the typical complexity of patients with CD requiring surgical intervention, multidisciplinary care with gastroenterologists, surgeons, radiologists, pathologists, and other ancillary team members is critical for optimizing patient care, (1).
Management of CD involves different medical disciplines working in conjunction with one another. These guidelines represent only a portion of the treatment necessary for the optimal care of these patients. This clinical practice guideline will focus on the surgical management of patients with CD.
- Scope and purpose
The scope of these guidelines is to select Crohn’s disease patients whom get the maximum benefit from surgical intervention.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to
improve the quality of medical care and surgical service, to provide the best clinical practice to
our patients, and finally to reduce the cost of medical service.
- Target audience
The principle targeted audiences are the practicing surgeons, however, gastroenterologists, ICU specialists, radiologists, nutritionists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2020 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the American Society of Colon and Rectal Surgeons Clinical Practice Guidelines, 2020,(1), the European Crohn’s and Colitis Organization Guidelines, 2024,(8), the Brazilian Organization of Crohn’s Disease and Colitis Guidelines, 2022,(9), The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula, 2022, (10) and Clinical practice guideline for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula, 2016, (11).
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 5& 6).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
these are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research needs
1. The prevalence of Crohn’s disease in Egypt.
2. The long-term outcome after surgical management of Crohn’s disease.
3. Outcome of video assisted anal fistula treatment.
4. Fistula-tract laser closure.
5. Over-the-scope clip for achieving healing in complex perianal fistulae in CD.
- Clinical indicators for monitoring
1. Documentation of the clinical symptoms and signs.
2. Radiology (ultrasonography, CT scan and/or MRI)
3. Colonoscopy.
4. Documentation of the type of treatment, (medical, aspiration, surgical).
5. Documentation of the surgical details (stricturoplasty, type of resection, type of anastomosis and type of diversion if done)
- Updating of the guideline
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about surgical management of Crohn’s disease. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1. Quality and Significance of the four levels of evidence in GRADE:
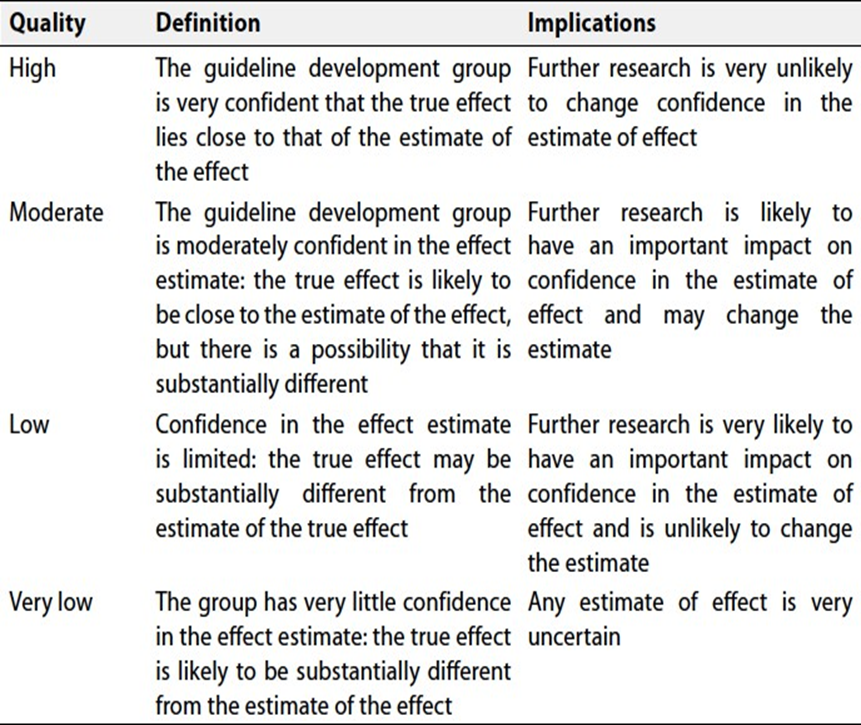
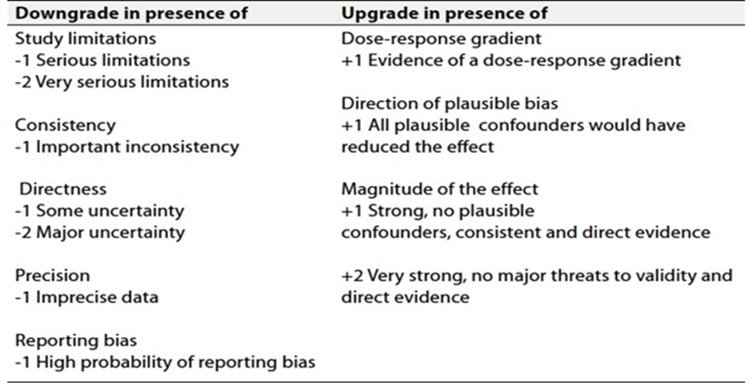
Table 2. Factors that determine How to upgrade or downgrade the quality of evidence
- References
1. Lightner AL, Vogel JD, Joseph C. Carmichael JC, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Surgical Management of Crohn’s Disease. Dis Colon Rectum 2020; 63: 1028–52.
2. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2018; 390:2769–78.
3. Bemelman WA; S-ECCO collaborators. Evolving role of IBD surgery. J Crohn’s Colitis 2018; 12:1005–7.
4. Koltun WA. Better together: improved care of the IBD patient using the multi-disciplinary IBD center. Expert Rev Gastroenterol Hepatol 2017; 11:491–3.
5. Frolkis AD, Dykeman J, Negrón ME, et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology. 2013; 145:996–1006.
6. Ma C, Moran GW, Benchimol EI, et al. Surgical rates for Crohn’s disease are decreasing: a population-based time trend analysis and validation study. Am J Gastroenterol. 2017; 112:1840–8.
7. Frolkis AD, Lipton DS, Fiest KM, et al. Cumulative incidence of second intestinal resection in Crohn’s disease: a systematic review and meta-analysis of population-based studies. Am J Gastroenterol. 2014; 109:1739–48.
8. Michel Adamina M, Silvia Minozzi S, Warusavitarne J, et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. Journal of Crohn's and Colitis, 2024, 18, 1556–1582.
9. Zabot GP, Cassol OS, Quaresma AB, et al. Surgical management of adult Crohn’s disease and ulcerative colitis patients: a consensus from the Brazilian Organization of Crohn’s Disease and Colitis (GEDIIB). Arq Gastroenterol • 2022. v. 59. Suplemento. AG-2022-120 doi.org/10.1590/S0004-2803.2022005S1-01.
10. Gaertner, WB, Burgess, PL, Davids, JS, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula, Dis Colon Rectum 2022 Aug 1;65(8):964-985. doi: 10.1097/DCR.0000000000002473.
11. Vogel, JD, Johnson, EK,.Morris, AM, et al. Clinical practice guideline for the management of anorectal abscess, fistula-in-ano, and rectovaginal fistula. Dis Colon Rectum 2016; 59: 1117–1133 DOI: 10.1097/DCR.0000000000000733.