the Management of Ventral Hernia
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحه عامه |
| كتاب: | the Management of Ventral Hernia |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:02 AM |
الوصف
"last update: 10 March 2026" Download Guideline
- Executive Summary
This guideline describes the management of ventral hernia.
· We recommend that all midline laparotomies should be closed with non-absorbable or long-term absorbable sutures, (Strong recommendation).
· We advise closing all midline laparotomies with a small bite continuous technique achieving a wound to suture length ratio of at least 4:1. Prophylactic mesh may be advised in high-risk patients, (Conditional recommendation).
· We recommend that the decision for surgery in patients with asymptomatic hernias should individualized based on patient risk, co-morbidities, life expectancy and type of hernia, (Strong recommendation).
· We recommend repair for all symptomatic hernias, unless there are contra-indications to surgery or anesthesia, (Strong recommendation).
· We recommend performing emergency surgery for strangulated hernia without delay, aiming for the simplest procedure with the lowest complication rate, (Strong recommendation).
· Where technically feasible laparoscopic ventral hernia surgery is the preferred and advised approach for patients with BMI >35kg/m2, (Conditional recommendation).
· We advise performing laparoscopic repair in the setting of incarcerated or strangulated hernias. The risk reduction in SSI rates is noted though the surgeon's experience will dictate the approach, (Conditional recommendation).
· We recommend performing concurrent umbilical hernia repair during laparoscopic cholecystectomy, (Strong recommendation).
· We advise performing umbilical hernia repair with mesh as a concurrent procedure when performing laparoscopic groin hernia repair, (Conditional recommendation).
· We advise performing concomitant repair of an incisional or ventral hernia as a single stage procedure during bariatric surgery, (Conditional recommendation).
· In patients with liver disease, we advise performing an early elective mesh repair of umbilical hernia. Preoperative control of ascites is especially critical to a successful outcome, (Conditional recommendation).
· We advise performing mesh repair for hernia at the time of Caesarean Section, (Conditional recommendation).
· We recommend repairing rectus diastasis accompanied by a midline hernia during the hernia repair, (Strong recommendation).
· We recommend administration of a single dose preoperative prophylactic antibiotic before hernia repair, (Strong recommendation).
· We recommend the general surgical principles of DVT prophylaxis before the hernia repair, (Strong recommendation).
· Care should be taken to optimize the patient both medically and surgically preoperatively in order to ensure the best surgical and anesthetic outcome, (Strong recommendation).
· A minimum overlap of 5 cm before defect closure should be planned in all mesh repairs, (Strong recommendation).
· We recommend performing extra-peritoneal repairs in ventral hernia with plain large pore polypropylene or polyester mesh, (Strong recommendation).
· We recommend performing intraperitoneal mesh repairs with a composite barrier mesh or strand coated anti-adhesion mesh, (Strong recommendation).
· We do not advise the use of polypropylene mesh in grade 3A wounds, as it carries a high risk for septic complications, (Conditional recommendation).
· There is no evidence to support the routine use of biologic meshes. We may advise the use of biologics or delayed fully re-absorbable meshes in grade 3A and 3B wounds, (Conditional recommendation).
· We recommend performing every incisional hernia with a mesh repair because there is a significantly lower recurrence rate, (Strong recommendation).
· We recommend performing mesh repair for primary ventral hernias with a defect greater than 2 cm, (Strong recommendation).
· For primary hernias less than 2 cm in patients with risk factors for recurrence (obesity, concurrent hernia, recurrent hernia, concurrent diastasis or aneurysmal disease), we recommend a mesh repair, (Strong recommendation).
· Mesh placement for small hernias less than 2 cm is advised as the treatment of choice based on less recurrence rate, (Conditional recommendation).
· Patients presenting with a para-stomal hernia are recommended to have an elective repair, (Strong recommendation).
· We recommend careful inspection of the bowel pre, intra and post dissection to avoid missed enterotomy, (Strong recommendation).
· We recommend management of superficial wound sepsis with standard conservative means, (Strong recommendation).
· For deep surgical site infection with the possibility of mesh sepsis, we advise removal of the mesh, (Conditional recommendation).
· We recommend conservative management of post-operative seroma, (Strong recommendation).
· We advise performing laparoscopic ventral hernia repair as it had has a lower rate of wound infections and complications compared to open repair, (Conditional recommendation).
· We recommend against laparoscopic ventral hernia repair in special situations such as loss of domain, active entero-cutaneous fistula, the need to remove previously placed prosthetic mesh, (Strong recommendation).
- Recommendations
Section 1: Prevention of incisional hernia:
· We recommend that all midline laparotomies should be closed with non-absorbable or long-term absorbable sutures, (Strong recommendation, high certainty evidence, (18)).
· We advise closing all midline laparotomies with a small bite continuous technique achieving a wound to suture length ratio of at least 4:1. Prophylactic mesh may be advised in high-risk patients, (Conditional recommendation, high certainty evidence, (18)).
Section 2: Indications for surgery:
· We recommend that the decision for surgery in patients with asymptomatic hernias should individualized based on patient risk, co-morbidities, life expectancy and type of hernia, (Strong recommendation, high certainty evidence, (18)).
· We recommend repair for all symptomatic hernias, unless there are contra-indications to surgery or anesthesia, (Strong recommendation, high certainty evidence, (18)).
· We recommend performing emergency surgery for strangulated hernia without delay, aiming for the simplest procedure with the lowest complication rate, (Strong recommendation, high certainty evidence, (18)).
· Where technically feasible laparoscopic ventral hernia surgery is the preferred and advised approach for patients with BMI >35kg/m2, (Conditional recommendation, high certainty evidence, (18)).
· We advise performing laparoscopic repair in the setting of incarcerated or strangulated hernias. The risk reduction in SSI rates is noted though the surgeon's experience will dictate the approach, (Conditional recommendation, moderate certainty evidence, (18)).
· We recommend performing concurrent umbilical hernia repair during laparoscopic cholecystectomy, (Strong recommendation, moderate certainty evidence, (18)).
· We advise performing umbilical hernia repair with mesh as a concurrent procedure when performing laparoscopic groin hernia repair, (Conditional recommendation, low certainty evidence, (18)).
· We advise performing concomitant repair of an incisional or ventral hernia as a single stage procedure during bariatric surgery, (Conditional recommendation, moderate certainty evidence, (18)).
· In patients with liver disease, we advise performing an early elective mesh repair of umbilical hernia. Preoperative control of ascites is especially critical to a successful outcome, (Conditional recommendation, moderate certainty evidence, (18)).
· We advise performing mesh repair for hernia at the time of Caesarean Section, (Conditional recommendation, moderate certainty evidence, (18)).
· We recommend repairing rectus diastasis accompanied by a midline hernia during the hernia repair, (Strong recommendation, high certainty evidence, (18)).
Section 3: Perioperative management:
· We recommend administration of a single dose preoperative prophylactic antibiotic before hernia repair, (Strong recommendation, high certainty evidence, (18)).
· We recommend the general surgical principles of DVT prophylaxis before the hernia repair, (Strong recommendation, moderate certainty evidence, (18)).
· Care should be taken to optimize the patient both medically and surgically preoperatively in order to ensure the best surgical and anesthetic outcome, (Strong recommendation, high certainty evidence, (18)).
Section 4: Use of mesh:
· A minimum overlap of 5 cm before defect closure should be planned in all mesh repairs, (Strong recommendation, high certainty evidence, (18)).
· We recommend performing extra-peritoneal repairs in ventral hernia with plain large pore polypropylene or polyester mesh, (Strong recommendation, high certainty evidence, (18)).
· We recommend performing intraperitoneal mesh repairs with a composite barrier mesh or strand coated anti-adhesion mesh, (Strong recommendation, moderate certainty evidence, (18)).
· We do not advise the use of polypropylene mesh in grade 3A wounds, as it carries a high risk for septic complications, (Conditional recommendation, moderate certainty evidence, (18)), (table 7).
· There is no evidence to support the routine use of biologic meshes. We may advise the use of biologics or delayed fully re-absorbable meshes in grade 3A and 3B wounds, (Conditional recommendation, Low certainty evidence, (18)).
· We recommend performing every incisional hernia with a mesh repair because there is a significantly lower recurrence rate, (Strong recommendation, high certainty evidence, (18)).
· We recommend performing mesh repair for primary ventral hernias with a defect greater than 2 cm, (Strong recommendation, high certainty evidence, (18)).
· For primary hernias less than 2 cm in patients with risk factors for recurrence (obesity, concurrent hernia, recurrent hernia, concurrent diastasis or aneurysmal disease), we recommend a mesh repair, (Strong recommendation, high certainty evidence, (18)).
· Mesh placement for small hernias less than 2 cm is advised as the treatment of choice based on less recurrence rate, (Conditional recommendation, high certainty evidence, (18)).
· Patients presenting with a para-stomal hernia are recommended to have an elective repair, (Strong recommendation, high certainty evidence, (18)).
Section 5: Complications:
· We recommend careful inspection of the bowel pre, intra and post dissection to avoid missed enterotomy, (Strong recommendation, high certainty evidence, (18)).
· We recommend management of superficial wound sepsis with standard conservative means, (Strong recommendation, high certainty evidence, (18)).
· For deep surgical site infection with the possibility of mesh sepsis, we advise removal of the mesh, (Conditional recommendation, moderate certainty evidence, (18)).
· We recommend conservative management of post-operative seroma, (Strong recommendation, moderate certainty evidence, (18)).
Section 6: Laparoscopic versus Open:
· We advise performing laparoscopic ventral hernia repair as it had has a lower rate of wound infections and complications compared to open repair, (Conditional recommendation, moderate certainty evidence, (19)).
· We recommend against laparoscopic ventral hernia repair in special situations such as loss of domain, active entero-cutaneous fistula, the need to remove previously placed prosthetic mesh, (Strong recommendation, moderate certainty evidence, (19)).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for developing this guideline.
Chair of GDG: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GDG: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
|
AGREEII |
Appraisal of Guidelines for Research and Evaluation II |
|
BMI |
Body Mass Index. |
|
COPD |
Chronic Obstructive Pulmonary Disease. |
|
DVT |
Deep Vein Thrombosis. |
|
EHS |
European Hernia Society. |
|
GDG |
Guideline Development Group. |
|
GRADE |
Grading of Recommendations, Assessment, Development and Evaluation. |
|
SSI |
Surgical site infection. |
- Introduction
Ventral hernia is one of the most common general surgical pathologies. An estimated 20 million patients with hernias are operated on worldwide every year, of which approximately 30% are ventral. An incisional hernia will develop in 10–15% of patients with an abdominal incision and the risk increases to up to 23% in those who develop surgical site infection, (1&2). Incidence rates up to 69% have been reported in high-risk patients, (3).
Ventral hernias are defined as a defect of the fascia in the anterior abdominal wall with or without a bulge, (4). Clinical presentation varies from small incidental defects to giant and complicated hernias with fistulas and viscera located outside the abdominal cavity covered only by peritoneum and skin (loss of domain), (4). The symptoms range from minor cosmetic concerns to severe pain and life-threatening conditions such as bowel obstruction, incarceration, strangulation and perforation, (4).
Ventral hernia repairs are mostly elective (90%) procedures, but the repair methods are highly variable, (5).
Any injury or incision to the abdominal wall could lead to a hernia. Surgical technique and wound infection are considered the most important preventable causes of an incisional hernia, (6).
Many patient-related risk factors have been implicated. Surgical site infections (SSI) are independent risk factors that significantly increase the risk of incisional hernias, (7). Other factors are male gender, obesity, (8) old age, (9) diabetes mellitus, jaundice, (10) anaemia, the use of vasopressor drugs, (11) smoking, (12) postoperative respiratory failure, aneurysmal disease, malnutrition, steroids, kidney failure, malignancy, (6). Abdominal distention,(13) postoperative peritonitis, (14) and multiple operations through the same incision, (10). Chronic Obstructive Pulmonary Disease (COPD), benign prostatic hypertrophy, constipation and ascites increase the intra-abdominal pressure, increasing the risk of incisional hernias, but they are not considered independent risk factors. Diastasis of the rectus muscles also predisposes to an incisional hernia, (15&16).
According to the European Hernia Society (EHS) classification, it divides hernias into primary and incisional (secondary) and then further subdivides them by anatomical location and size. Incisional hernias are also categorized by recurrence in a binary fashion, (17), (see Tables 1-4).
- Scope and Purpose
The scope of this guideline is to set recommendations for the diagnose and treatment of ventral hernia
The main purpose of these guidelines is to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the good surgical practice to our patients, and finally to be cost effective.
- Target Audience
The principle targeted candidates are the practicing surgeons, however radiologists, ICU specialists and nursing staff may be included.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2014 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the HIG (SA) Guidelines for the Management of Ventral Hernias. 2016 and Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias. 2014.
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
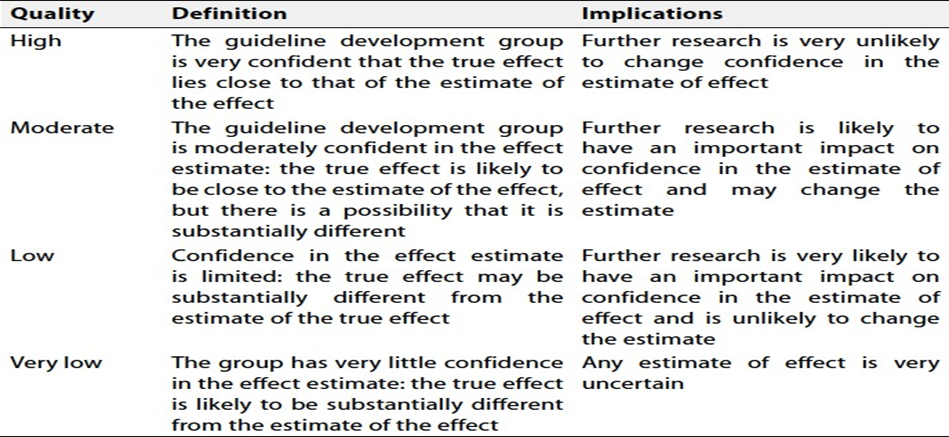
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (tables 5& 6).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
these are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research Needs
1. Management of ventral hernia with loss of domain.
2. Management of ventral hernia in morbidly obese patients.
3. Management of infected mesh.
4. Prevention and management of postoperative seroma after ventral hernia repair.
- Clinical Indicators for Monitoring
1. Pre-operative US and /or CT.
2. Documentation of the site of hernia.
3. Documentation of the size of Hernia.
4. Documentation of the associated co-morbidities.
5. Documentation of surgical steps.
- Updating of the Guidelines
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about ventral hernia. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1. Primary ventral hernia classification, (17)
|
Primary ventral hernia classification |
Diameter (cm). |
|
Midline Epigastric Umbilical |
Small Medium Large < 2 cm 2 – 4 cm > 4 cm
|
|
Lateral Spigelian Lumbar |
|
Table 2. Incisional hernia classification, (17)
|
Midline Sub-xiphoid M1 Epigastric M2 Umbilical M3 Infra-umbilical M4 Suprapubic M5
|
|
Lateral Subcostal L1 Flank L2 Iliac L3 Lumbar L4 |
|
Recurrent incisional hernia Yes No |
|
Length (cm) |
|
Width (cm) < 4cm W1 4 - 10 cm W2 >4 cm W3
|
Table 3. Incisional hernia anatomical location borders, (17)
|
Borders of Borders of Midline area Lateral area ______________________________________________
Cranial Xiphoid process Costal margin Caudal Pubic bone Inguinal ligament Lateral Linea semilunaris Lumbar region Medial Linea semilunaris
|
Table 4. M and L zones for incisional hernia, (17)
|
Medial |
Lateral |
||||
|
M1 |
Sub-xiphoidal |
Xiphoid to 3 cm caudally |
L1 |
Subcostal |
Between the costal margin and a horizontal line 3 cm above the umbilicus |
|
M2 |
Epigastric |
3 cm below the xiphoid to 3 cm above the umbilicus |
L2 |
Flank |
Latera to the rectal sheath in the area 3 cm above and below the umbilicus |
|
M3 |
Umbilical |
3 cm above to 3 cm below the umbilicus |
L3 |
Iliac |
Between a horizontal line 3 cm below the umbilicus and the inguinal region |
|
M4 |
Infra-umbilical |
3 cm below the umbilicus To 3 cm above the pubis |
L4 |
Lumbar |
Latero dorsal to the anterior axillary line |
|
M5 |
Supra-pubic |
Pubic symphysis to 3 cm Cranially |
|
|
|
Table
5. Quality and Significance of the four levels of evidence in GRADE
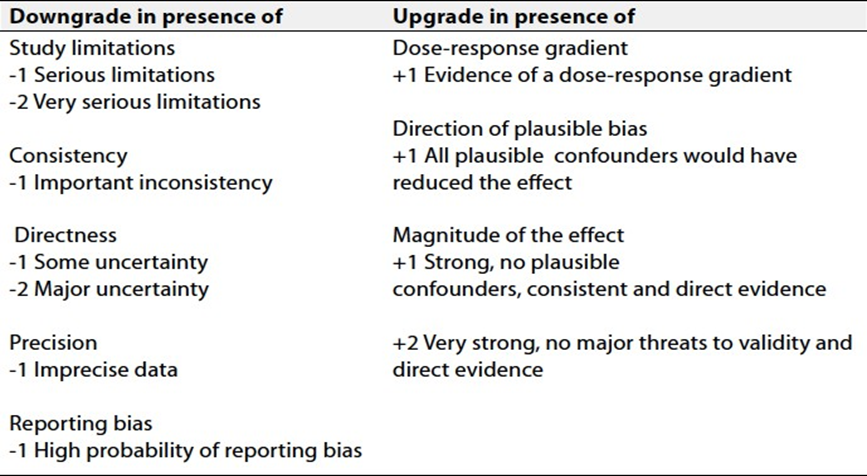
Table 6.
Factors that determine How to upgrade
or downgrade the quality of evidence
|
Table 7: Recommendations for mesh placed in the EXTRAPERITONEAL POSITION, (17). |
|
VHWG 2013 grade11 Risk Factors Recommended mesh Mesh to consider Contra-indicated mesh |
|
Low risk Composite, Biologic, Grade 1: Low risk No history of wound Plain mesh Fully absorbable PTFE infections Co-morbidities: Grade 2: Smoker, obese, Composite, Biologic, Intermediate risk diabetic, COPD, Plain mesh Fully absorbable PTFE previous wound infection Grade 3A Clean contaminated No mesh Plain Mesh*, Fully Composite, PTFE absorbable, Biologic Grade 3B Contaminated No mesh Fully absorbable, Composite, PTFE Biologic Grade 3C Dirty contaminated No mesh Fully absorbable Composite, Biologic, PTFE *It is recommended that if proceeding with a mesh repair after enterotomy, it should be large pore and placed in the retro-rectus position which is away from the peritoneal cavity and skin and is a well vascularized plane. |
- References
1. Kingsnorth A, LeBlanc K. Hernias: Inguinal and incisional. The Lancet. 2003;362(9395):1561-1571.
2. Rutkow IM. Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am. 2003;83(5):1045-1051.
3. Alnassar S, Bawahab M, Abdoh A, Guzman R, Al Tuwaijiri T, Louridas G. Incisional hernia postrepair of abdominal aortic occlusive and aneurysmal disease: Five-year incidence. Vascular. 2012;20(5):273-277.
4. Helgstrand F, Rosenberg J, Bay-Nielsen M, et al. Establishment and initial experiences from the Danish ventral hernia database. Hernia. 2010;14(2):131-135.
5. Korenkov M, Paul A, Sauerland S, et al. Classification and surgical treatment of incisional hernia. Langenbeck's Arch Surg. 2001;386(1):65-73.
6. Shell DH, De La Torre J, Andrades P, Vasconez LO. Open repair of ventral incisional hernias. Surg Clin North Am. 2008;88(1):61-83.
7. Bucknall TE, Cox PJ, Ellis H. Burst abdomen and incisional hernia: A prospective study of 1129 major laparotomies. Br Med J (Clin Res Ed). 1982;284(6320):931-933.
8. Israelsson LA, Jonsson T. Overweight and healing of midline incisions: The importance of suture technique. Eur J Surg. 1997;163(3):175-180.
9. Bevis P, Windhaber R, Lear P, Poskitt K, Earnshaw J, Mitchell D. Randomized clinical trial of mesh versus sutured wound closure after open abdominal aortic aneurysm surgery. Br J Surg. 2010;97(10):1497-1502.
10. Lamont P, Ellis H. Incisional hernia in re-opened abdominal incisions: An overlooked risk factor. Br J Surg. 1988;75(4):374- 376.
11. Hoer J, Lawong G, Klinge U, Schumpelick V. Factors influencing the development of incisional hernia. A retrospective study of 2,983 laparotomy patients over a period of 10 years. Chirurg. 2002;73(5):474-480.
12. Sørensen LT, Hemmingsen UB, Kirkeby LT, Kallehave F, Jørgensen LN. Smoking is a risk factor for incisional hernia. Arch Surg. 2005;140(2):119-123.
13. Jenkins T. The burst abdominal wound: A mechanical approach. Br J Surg. 1976;63(11):873-876.
14. Moussavian MR, Schuld J, Dauer D, et al. Long term follow up for incisional hernia after severe secondary peritonitis— incidence and risk factors. Am J Surg. 2010;200(2):229-234.
15. Cheesborough JE, Dumanian GA. Simultaneous prosthetic mesh abdominal wall reconstruction with abdominoplasty for ventral hernia and severe rectus diastasis repairs. Plast Reconstr Surg. 2015;135(1):268-276.
16. Köhler G, Luketina R, Emmanuel K. Sutured repair of primary small umbilical and epigastric hernias: Concomitant rectus diastasis is a significant risk factor for recurrence. World J Surg. 2015;39(1):121-126.
17. Muysoms F, Miserez M, Berrevoet F, et al. Classification of primary and incisional abdominal wall hernias. Hernia. 2009;13(4):407-414.
18. Bougard H, Coolen D, De Beer R, et al. HIG (SA) Guidelines for the Management of Ventral Hernias. 2016;[ vol 54 No 3: 1- 29.
19. Bittner R, Bingener-Casey J, Dietz U, et al. Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias. 2014, (International Endohernia Society (IEHS)-Part 1. Surg Endosc 28:2-29.