The Use of Coronary Computed Tomography Angiography for Patients Presenting with Acute Coronary Syndrome
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | طب الأشعة |
| كتاب: | The Use of Coronary Computed Tomography Angiography for Patients Presenting with Acute Coronary Syndrome |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:01 AM |
الوصف
"last update: 30 March 2026" Download Guideline
- Executive Summary
· The clinician properly evaluates the patient before requesting CTA guided by the patient's history, clinical presentation, ECG, and initial biomarker assessment. Good Practice Statement
· The clinician should acquire ECG and review it for STEMI and Cardiac troponin should be measured as soon as possible. Good Practice Statement
· The clinician should categorize patients into low-, intermediate- and high-risk according to risk stratification tools. The clinician should indicate the appropriate criteria for performing CCTA. Good Practice Statement
· The clinician may request non-contrast coronary calcium scoring for asymptomatic individuals and intermediate-risk individuals (Framingham Risk Score 10%-20%) to document atherosclerotic cardiovascular disease risk stratification and guide preventive measures. Conditional recommendation
· The clinician should not request non-contrast coronary calcium scoring for high-risk individuals, patients already receiving statin treatment or asymptomatic low-risk adults: Strong recommendation.
·
The radiologist should report
non-contrast coronary calcium scoring and categorize patients as no CAC
(Agatston score 0), mild (1-100), moderate (101-400), or severe (>400). Strong
recommendation
· Clinicians should request CCTA as the first line test for evaluating patients with or without history of CAD who present with stable typical or atypical chest pain, or other symptoms that are thought to represent a possible anginal equivalent (e.g., dyspnea on exertion, jaw pain). Strong recommendation
· Clinicians should request CCTA following a non-conclusive functional test to obtain more precision regarding diagnosis and prognosis if such information will influence subsequent patient management. Strong recommendation
· Clinicians should request CCTA for patients at higher pretest risk for ACS, including patients with non-ST elevation myocardial infarction (NSTEMI) when the invasive strategy is not preferred (e.g., bleeding risk, vascular access issues, patient preference). Strong recommendation
· Clinicians should not recommend CTA for low-risk patients or patients with high probability (cardiac catheterization is recommended). Strong recommendation
· Clinicians should request CTA for the assessment of coronary stents in symptomatic patients with coronary stents >3mm, with current generation drug-eluting stents that have struts <3mm, and with current generation drug-eluting stents that have struts <100µm. Strong recommendation
· Clinicians may request CTA for the assessment of stents with smaller diameters (<3mm) as they are more challenging to assess, yet CTA may still be a reasonable test for assessing proximal, non-bifurcation thin strut stents that are <3mm. Conditional recommendation
· Clinicians should request CCTA for the assessment patency of coronary artery bypass grafts in symptomatic patients. Strong recommendation
· Clinicians should request CCTA for assessment of graft patency, anastomotic sites, and stenosis, in presurgical planning of redo bypass graft. Strong recommendation
· Clinicians should request CCTA for assessment of coronary grafts and not for assessment of the native coronary arteries in patients with prior CABG as it is of limited value due to severe calcification of the native coronary artery. Strong recommendation
· Clinicians may request CT-FFR for evaluation of lesion-specific physiology from a coronary CTA dataset using computational flow dynamic modeling and some hemodynamic assumptions, increasing the specificity of CCTA. Conditional recommendation
· Clinicians may request CCTA for measuring extracellular volume fraction (ECV), yet the gold standard test for measuring ECV is Cardiac MRI. Conditional Recommendation
· Clinicians may request CCTA for estimation of myocardial perfusion and viability as an alternative modality to Cardiac MR in patients with MRI contraindications. Conditional recommendation
· Clinicians should educate the patient about the nature of the examination, its objectives, possible risks including radiation dose, their required cooperation, and the sensations they are likely to feel. Patients should be given a chance to request an alternative diagnostic strategy if they feel unable or unwilling to proceed. Good Practice Statement
· The radiologist should repeat the educational process after premedication, just before scanning, to ensure patients remember instructions on breath-holding and are prepared for the sensations likely to occur from nitroglycerin and contrast administration. Good Practice Statement
· The radiologist/radiographer should obtain CTA in minimum CT scanner specifications as 64-detector row or greater or dual-source scanners, axial resolution ≤0.5×0.5mm, Z-axis resolution ≤1mm and temporal resolution ≤250ms. Strong recommendation
· The radiologist/radiographer should obtain Prospective ECG-triggering CCTA (the most commonly protocol) when the heart rate is regular and low (< 65 BPM). Strong recommendation;
· The radiologist/radiographer should obtain Retrospective ECG gating for coronary artery evaluation when the heart rate is high and in cases of arrhythmia. Strong recommendation
· The radiologist/radiographer may obtain Retrospective ECG gating for ventricular functional assessment when other modalities are not available. Conditional recommendation
· The radiologist is responsible for safety considerations of coronary CTA related to radiation exposure using the principle of As Low As Reasonably Achievable (ALARA). Strong recommendation
· The radiologist/radiographer should perform CCTA with the minimum accepted radiation dose (approximately 3 mSv), by applying the radiation protection measures as ECG-based tube current modulation , a high-pitch helical scan , reducing the tube potential from 120 to 100 kVp, noise reduction methods such as iterative reconstruction and suitable Z-axis coverage . Strong recommendation
· The radiologist/radiographer should perform CCTA after administration of intravenous iodinated water-soluble contrast media to ensure optimal vascular enhancement between 250 and 300HU in the ascending aorta. Strong recommendation
· The radiologist is responsible for safety considerations of coronary CTA related to allergic reactions to iodinated contrast agents, and contrast-induced nephropathy. Strong recommendation
· The radiologist should check the renal function tests before administration of the contrast media. If the eGFR value is greater than 30 the patient can receive IV iodinated contrast. If eGFR is less than or equal to 30 the case will need approval by the radiologist before IV contrast is used to minimize the risk of contrast-related AKI. Strong recommendation
·
The radiologist should ensure the
presence of patient safety equipment includings: advanced cardiovascular life support
(ACLS) equipment in the patient preparation and scanner areas. Properly trained ACLS-certified
nurses or similar qualified staff should supervise the premedication of
patients as administration of beta blockers and nitrates. A rapid response team
and/or an ACLS-certified physician should be readily available for prompt
response to urgent or emergent complications. Strong recommendation
· The radiologist should perform CCTA after preparing the patient by Beta-blocker (metoprolol) to control the heart rate for maximum image quality during low and regular heart rates. Strong recommendation
· The radiologist should be familiar with the common contra-indications for beta-blockers such as heart block, hypotension, systolic dysfunction, poorly controlled asthma, severe aortic valve stenosis, severe bradycardia. Strong recommendation
· The radiologist may perform CCTA after preparing the patient by giving oral (sublingual) nitroglycerin Conditional recommendations
· The radiologist should be familiar with the common contraindications for nitroglycerin as erectile dysfunction medication (sildenafil, tadalafil, etc.) taken within the last 24-48 hr., increased intracranial pressure, right-sided myocardial infarction, severe anemia, known allergy or hypersensitivity . Conditional recommendations
· The radiologist should process the axial source image in a dedicated workstation and get more advanced post-processing techniques to assess cardiac anatomy such as multiplanar reformats, curved multiplanar reformats, volume-rendered three-dimensional images, and cinematic rendering. If functional information is obtained, then segmentation of the ventricular cavities can be used to quantify ventricular volumes and systolic function. Good Practice Statement
· The interpreting radiologist must be a physician adequately trained in cardiac CT as defined in recent training guidelines issued by the Society of Cardiovascular CT. The interpreting radiologist should be promptly available in place or by phone for consultation about patient preparation and scan protocol. Good Practice Statement
· The radiologist should report the radiological findings of CTA in one of the following formats: The Written Conventional Report or The Coronary Artery Disease-Reporting and Data System (CAD-RADS 2.0). The report should contain the relevant imaging findings, their interpretation, an overall summary/conclusion, and recommendations for further management. Good Practice Statement
- Recommendations
1- Patient evaluation before CTA
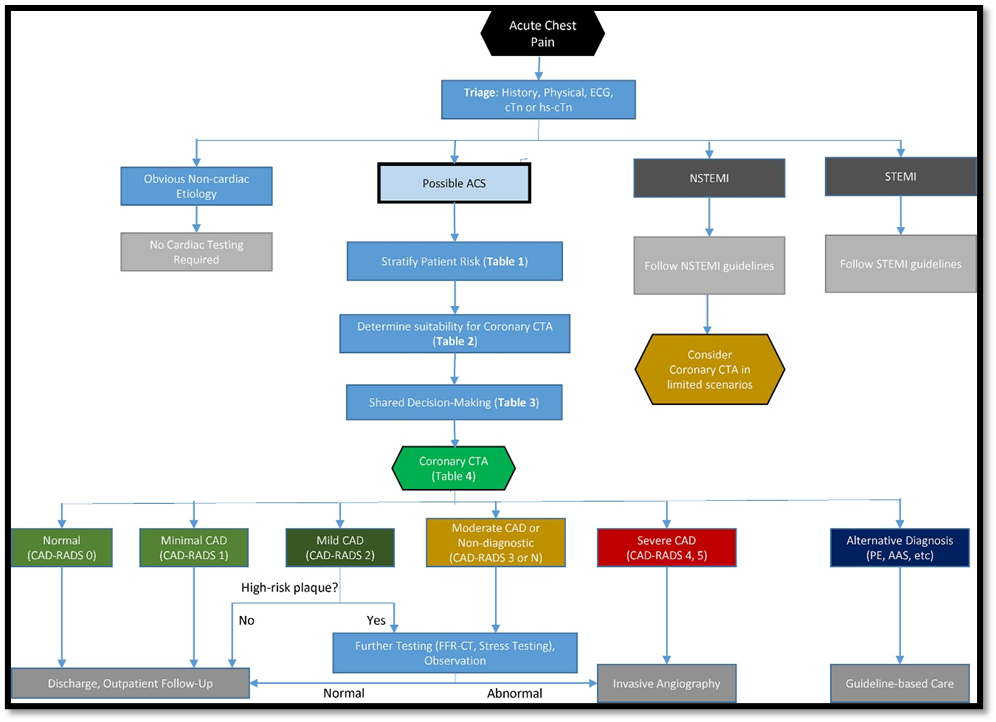
1.1 The clinician properly evaluates the patient before requesting CTA guided by the patient's history, clinical presentation, ECG, and initial biomarker assessment. Clinically appropriate patients should have reasonable clinical pre-test likelihood of ACS and exclude alternative non-coronary diagnoses as shown in (Fig.1).
Good Practice Statement (5.6)
1.2 The clinician should acquire ECG and review it for STEMI and Cardiac troponin should be measured as soon as possible.
Good Practice Statement (5.6)
1.3 The clinician should categorize patients into low-, intermediate- and high-risk according to the risk stratification tools. The clinician should indicate the appropriate criteria for performing CCTA.
Good Practice Statement (5.6)
2. Non-contrast Coronary Calcium Scoring (Coronary Agatston Scoring)
2.1 The clinician may request non-contrast coronary calcium scoring for asymptomatic individuals and intermediate-risk individuals (Framingham Risk Score 10% to 20 to document atherosclerotic cardiovascular disease risk stratification and guide preventive measures in
Conditional recommendation
High-Quality Evidence (7,8).
2.2 The clinician should not request non-contrast coronary calcium scoring for high-risk individuals, patients already receiving statin treatment or asymptomatic low-risk adults
Strong recommendation
High-quality evidence (7,8).
2.3 The radiologist should report and categorize patients as no CAC (Agatston score 0), mild (1-100), moderate (101-400), or severe (>400).
Strong recommendation
High-quality evidence (7,8).
3. Coronary CT of the Native Coronary Arteries
3.1 Clinicians should
request CTA as the first line test for evaluating patients with or without
history of CAD who present with stable typical or
atypical chest pain, or other symptoms that are thought to represent a possible
angina equivalent (e.g., dyspnea on exertion, jaw pain).
3.2 Clinicians should request CTA following a non-conclusive functional test, to obtain more precision regarding diagnosis and prognosis if such information will influence subsequent patient management.
3.3 Clinicians should request CTA for patients at higher pretest risk for ACS, including patients with non-ST elevation myocardial infarction (NSTEMI) when the invasive strategy is not preferred (e.g., bleeding risk, vascular access issues, patient preference).
3.4 Clinician should not recommend CTA for low-risk patients or patients with high probability (cardiac catheterization is recommended).
Strong recommendation
High-quality evidence (9,10)
4. Coronary CTA for Coronary Artery Stents
4.1 Clinicians should request CTA for the assessment of coronary stents in symptomatic patients with coronary stents >3mm, with current generation drug-eluting stents that have struts <3mm, and with current generation drug-eluting stents that have struts <100µm
Strong recommendation
High-quality evidence (11).
4.2 Clinicians should not request CTA for the assessment of stents with smaller diameters (<3mm) as they are more challenging to assess, yet CTA may still be a reasonable test for assessing proximal, non-bifurcation thin strut stents that are <3mm.
Conditional recommendation
High-quality evidence (11).
5. Coronary CT for Coronary Artery Bypass Grafts
5.1 Clinicians should request CCTA for the assessment patency of coronary artery bypass grafts in symptomatic patients. CTA offers a non-invasive and reliable method to assess the patency of coronary artery bypass grafts, including both arterial and venous grafts.
Strong recommendation
High-quality evidence (12).
5.2 Clinicians should request CCTA for assessment of graft patency, anastomotic sites, and stenosis, in presurgical planning of redo bypass graft.
Strong recommendation
High-quality evidence (12)
5.3 Clinicians should request CCTA for assessment of coronary grafts and not for assessment of the native coronary arteries in patients with prior CABG as it is of limited value due to severe calcification of the native coronary artery.
Strong recommendation
High-quality evidence (12)
6. Computed Tomography-Fractional Flow Reserve (CT-FFR)
6.1 Clinicians may request CT-FFR for evaluation of lesion-specific physiology from a coronary CTA dataset using computational flow dynamic modeling and some hemodynamic assumptions, increasing the specificity of CCTA (if available).
CT-FFR estimates the pressure drop across a stenosis providing a ratio indicative of lesion-specific ischemia. It reduces the proportion of patients referred to ICA with anatomical stenoses on CCTA that are not hemodynamically significant. CT-FFR is not widely available as it requires high-quality computational resources, leading to off-site analyses, increased cost of testing, and consequently time delays.
Conditional Recommendation
High-quality evidence (13,14)
7. CCT-Extracellular Volume Fraction (CCT-ECV)
7.1 Clinicians may request CCTA for measuring extracellular volume fraction (ECV), which is an important imaging parameter to estimate the expansion of the myocardial extracellular space secondary to myocardial fibrosis. Yet, the gold standard for measuring ECV is Cardiac MRI.CT-based ECV measurements involve the acquisition of pre- and post-contrast images (or post-contrast images and virtual unenhanced images if acquired using dual-energy CT), allowing for the calculation of hematocrit-corrected ECV.
Conditional Recommendation
Moderate-quality evidence (15,16)
8. CCTA Myocardial Perfusion and Viability
8.1 Clinicians may request CCTA for estimation of myocardial perfusion and viability as an alternative modality to Cardiac MR in patients with MRI contraindications.
Myocardial computed tomography perfusion (CTP), to evaluate the presence and extent of myocardial ischemia by visualizing myocardial distribution of iodinated contrast material at rest and after pharmacologically induced stress
There are many associated challenges of myocardial CTP, including the need for pharmacological stress agents and additional radiation exposure, making careful patient selection critical. Cardiac MR is the gold standard for assessing myocardial perfusion and viability
Conditional recommendation
Moderate-quality evidence: (15, 17)
9. Patient Education
9.1- The clinician should inform the patient about the nature of the examination, its objectives, possible risks including radiation dose, their required cooperation, and the sensations they are likely to feel. This is a critical component of shared decision-making. Patients should be given a chance to request an alternative diagnostic strategy if they feel unable or unwilling to proceed.
9.2- The radiologist should repeat the educational process after premedication, just before scanning, to ensure patients remember instructions on breath-holding and are prepared for the sensations likely to occur from nitroglycerin and contrast administration.
Good Practice Statement (5.6)
10- CT Scanner Requirements
10.1 The radiologist/radiographer should obtain CTA according to the minimum CT scanner specifications which meet or exceed criteria outlined by the American College of Radiology, North American Society for Cardiovascular Imaging, and the Society for Pediatric Radiology practice parameters as listed below:
· 64-detector row or greater or dual-source scanners
· Axial resolution ≤0.5×0.5mm
· Z-axis resolution ≤1mm
· Temporal resolution ≤250ms
Strong recommendation
High-quality evidence (18,19).
11. Coronary CTA Acquisition Protocol
11.1 The radiologist/radiographer should obtain Prospective
ECG-triggering CCTA (the most commonly protocol) when the heart rate is regular
and low (< 65 BPM) .
The data acquisition in best diastole phase when there is less motion to
minimize cardiac motion blurring.
Strong recommendation;
High-quality evidence (18, 20).
11.2 The radiologist/radiographer should obtain Retrospective ECG gating is for coronary artery evaluation when the heart rate is high and in cases of arrhythmia
Strong recommendation;
High-quality evidence (18,20).
11.3 The radiologist/radiographer may obtain Retrospective ECG gating is for ventricular functional assessment when other modalities are not available.
Conditional recommendation;
High-quality evidence (18,20)
12. Radiation Safety
12.1 The radiologist is responsible for safety considerations of coronary CTA related to radiation exposure using the principle of As Low As Reasonably Achievable (ALARA). The radiologist/radiographer should perform CCTA with the minimum accepted radiation dose (approximately 3 mSv), by applying the radiation protection measures:
- ECG-based tube current modulation, whereby the mAs is reduced to 20% or 40% during part of the cardiac cycle, typically systole.
- A high-pitch helical scan (pitch of 3.2-3.4) is available on dual-source CT scanners that enable imaging of the entire heart during a single beat, which reduces radiation exposure.
- Reducing the tube potential from 120 to 100 kVp, it is possible to reduce the radiation dose while improving vascular enhancement. N.B., The ability to reduce kVp is often guided by the patient’s weight. Larger patients require a higher kVp for optimal image quality.
- Noise reduction methods such as iterative reconstruction were introduced as an effective radiation dose reduction strategy.
- Suitable Z-axis coverage should be limited to the minimum clinically required. For coronary imaging, scanning from the carina to just beyond the bottom of the heart is generally sufficient. If there is a history of coronary artery bypass surgery, the coverage should begin at the lung apices to include the entire course of internal mammary grafts
Strong recommendation
High-quality evidence (21,22).
13- Contrast Medium Administration
13.1 The radiologist is responsible for safety considerations of coronary CTA related to allergic reactions to iodinated contrast agents, and contrast-induced nephropathy. The radiologist/radiographer should perform CCTA after administration of intravenous iodinated water-soluble contrast media to ensure optimal vascular enhancement between 250 and 300HU in the ascending aorta by applying the following measures.
- The concentration of the contrast medial used should be 300-350 mg Iodine/ml
- In adult patients, the injection rate should be from 5 to 7mL/s using an 18G size needle recommended in an antecubital vein, preferably on the right
- The timing of contrast administration should be determined by using a test injection or bolus tracking technique
- Both dual injectors, biphasic (contrast followed by saline) and triphasic (contrast followed by mix of diluted contrast and then saline) protocols are used
- Check the renal function tests. If the eGFR value is greater than 30 the patient can receive IV iodinated contrast. If eGFR is less than or equal to 30 the case will need approval by the radiologist before IV contrast is used to minimize the risk of contrast-related AKI.
Strong recommendation
High-quality evidence (23,24).
13.2 The radiologist should ensure the presence of patient safety equipment including:
- Advanced cardiovascular life support (ACLS) equipment in the patient preparation and scanner areas.
- Properly trained ACLS-certified nurses or similar qualified staff should supervise the premedication of patients as administration of beta blockers and nitrates.
- A rapid response team and/or an ACLS-certified physician should be readily available for prompt response to urgent or emergent complications.
· Strong recommendation
· High-quality evidence (23,24).
14 - Patient Pre-medication
14.1 Beta-blocker
14.1.1 The radiologist should perform CCTA after preparing the patient by Beta-blocker (metoprolol) to control the heart rate for maximum image quality during low and regular heart rates.
-
Oral Beta-blocker : 50-100mg oral metoprolol given at
least 1h prior to CCTA; some suggest giving 24 h prior to CCTA for more
effective heart rate reduction
-
Intravenous Beta-blocker : 5mg intravenous metoprolol given
with repeated checks of blood pressure and heart rate up to a maximum of 25mg.
14.1.2 The radiologist should be familiar with the common contra-indications for beta-blockers such as heart block, hypotension, systolic dysfunction, poorly controlled asthma, severe aortic valve stenosis, severe bradycardia.
Strong recommendation
High-quality evidence (25.26).
14.2- Nitroglycerin
14.2.1 The radiologist may perform CCTA after preparing the patient by giving oral
(sublingual) nitroglycerin :
0.4-0.8mg (1-2 tablets), 5min prior to CCTA as the coronary vasodilatation usually
lasts for 20-30min
14.2.2 The radiologist should be familiar with the common contraindications for nitroglycerin which is erectile dysfunction medication (sildenafil, tadalafil, etc.) taken within the last 24-48 hr., increased intracranial pressure, right-sided myocardial infarction, severe anemia, known allergies or hypersensitivity
Conditional recommendations
Moderate-quality evidence (27).
15. Post-Processing Methods
15.1 The radiologist should process the axial source image in a dedicated workstation and get more advanced post-processing techniques to assess cardiac anatomy. These include multiplanar reformats, curved multiplanar reformats, volume-rendered three-dimensional images, and cinematic rendering. If functional information is obtained, then segmentation of the ventricular cavities can be used to quantify ventricular volumes and systolic function
Good Practice Statement (28).
16. Reporting Standard
16.1 The interpreting radiologist must be a physician adequately trained in cardiac CT as defined in recent training guidelines issued by the Society of Cardiovascular CT.
The interpreting radiologist should be promptly available in place or by phone for consultation about patient preparation and scan protocol.
Good Practice Statement (29)
16.2- The Written Conventional Report:
The written comprehensive report should contain the relevant imaging findings, their interpretation, an overall summary/conclusion, and recommendations for further management. A sample report is included in table 3.
Table 3. Sample structured report for coronary CTA. The structure may require modification depending on coronary anatomy, the presence of bypass grafts, etc. The CAD-RADS score may be included but should not replace the conclusion
|
CTA CORONARY REPORT |
||
|
INDICATION: |
|
|
|
COMPARISON: |
|
|
|
TECHNIQUE: |
Coronary CTA performed with [ECG gating, or prospective ECG triggering].
|
|
|
MEDICATION: |
|
|
|
QUALITY: |
|
|
|
CORONARY FINDINGS: |
Coronary origins: |
|
|
|
Coronary Dominance: |
|
|
|
Left main: |
|
|
|
Left anterior descending and branches: |
|
|
|
Left circumflex and branches: |
|
|
|
Right coronary and branches: |
|
|
INCIDENTAL FINDINGS:
|
|
|
|
CONCLUSION:
|
[Summary including most severe stenosis, the extent of plaque, recommendations, and significant incidental findings if any]. |
|
Good Practice Statement (30,31).
16.3 The Coronary Artery Disease-Reporting and Data System (CAD-RADS 2.0).
Recently (CAD-RADS 2.0 was created to standardize reporting and interpretation (table 4). It includes management recommendations based on the most severe coronary plaque stenosis and the overall burden of coronary atherosclerosis. The CAD-RADS provides a structured framework to interpret and report CTA findings and aims to improve communication between cardiac imagers and referring physicians, standardize reporting practices, provide a framework for patient management decisions, and facilitate research in CAD.
Table 4. CAD-RADS Reporting and Data System for Patients Presenting With Acute Coronary Chest Pain
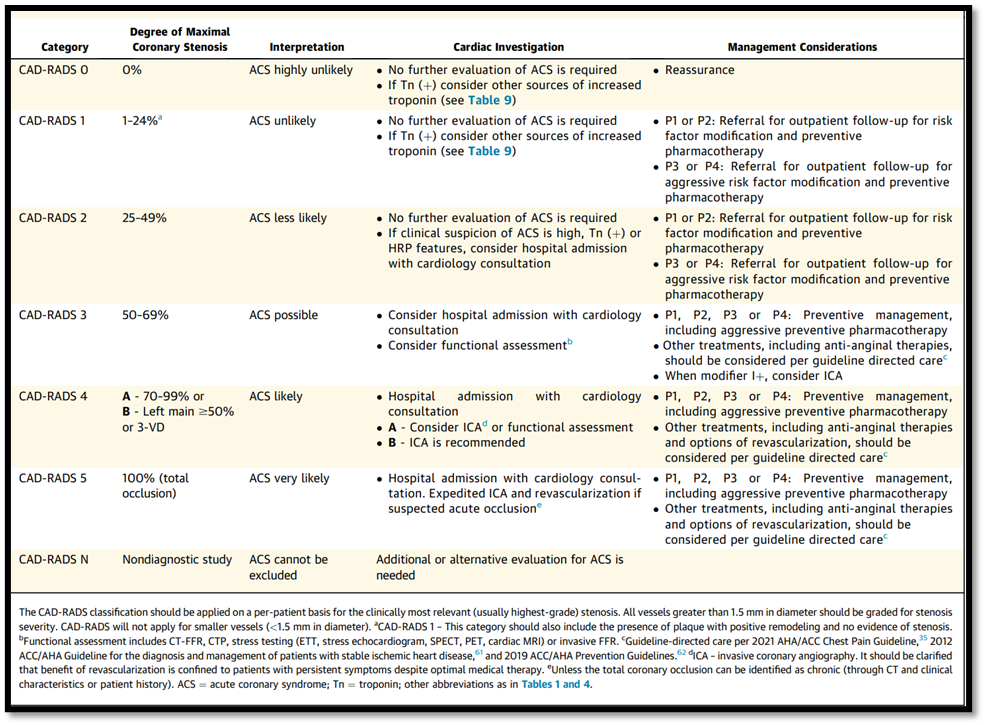
Good Practice Statement (32,33).
- Acknowledgment
The authors would like to thank the Egyptian Health Council- Committee of National Egyptian Guidelines and Radiology Scientific Guidelines Group who took the time to provide their feedback and peer review during the drafting of these guidelines
Chair of the Panel:
Tarek Eldiasty
Scientific Group Members:
Ragab Hani Donkol, IHab Reda, Khaled Matrawy, Maha Hussein Helal, Mohamed Fawzi, Mohamed Shaker, Wael Elshawaf, Wahid Tantawy, Ekram Hamed , Hadeel Saif ,Alaa Ragab Hani, Samira Saraya ,Ahmed Ramadan, Hassan A. Ibrahim
- Abbreviations
ACLS: advanced cardiovascular life support
ACP: Acute chest pain
ACR: American College of Radiology
ACS: Acute coronary syndrome
ASCVD: Atherosclerotic cardiovascular disease
CAD: Coronary artery disease
CCTA: Coronary computed tomography angiography
CHD: Coronary heart disease
CTA: Coronary computed tomography angiography
CVD: Cardiovascular disease
ED: Emergency department
IHD: Ischemic heart disease
MI: Myocardial infarction
NSTEMI: Non-ST-elevation myocardial infarction
STEMI: ST-elevation myocardial infarction
- Glossary
Acute chest pain requires urgent evaluation to rule out life-threatening causes, including acute coronary syndrome (ACS), aortic dissection, pulmonary embolism, and tension pneumothorax
Acute coronary syndrome (ACS): describes a range of symptoms related to acute myocardial ischemia or infarction. The three traditional types of ACS are non-ST-elevation myocardial infarction (NSTEMI), ST-elevation MI (STEMI), and unstable angina
Characters of acute coronary syndrome pain (cardiac angina):
· Pressure, fullness, burning, or tightness in the chest.
· Crushing or searing pain that spreads to the back, neck, jaw, shoulders, and one or both arms.
· Pain that lasts more than a few minutes, gets worse with activity, goes away and comes back, or varies in intensity.
· Shortness of breath.
- Introduction
Acute coronary syndrome is characterized by myocardial ischemia, typically secondary to Coronary Artery Disease (CAD). This condition often manifests during exertion and is directly related to impaired myocardial function.
The primary cause of CAD is the atherosclerosis of coronary arteries. It occurs when atherosclerotic plaque builds up within the walls of coronary arteries leading to the luminal narrowing and presentation with clinical manifestations of Acute Coronary Syndrome (ACS) that include unstable angina and myocardial infarction.
Risk factors of CAD exist among many individuals in the general population, which include hypertension, dyslipidemia, diabetes mellitus, chronic kidney disease, age, gender, lifestyle, cigarette smoking, diet, obesity, and family history.
Coronary Artery Disease is the most important cause of heart disease. Coronary artery disease (CAD) is one of the primary causes of death. The incidence of CAD is related to age, gender, and economic status. Cardiovascular Disease (CVD) has become the largest single cause of death worldwide. It is responsible for an estimated 17 million deaths and led to 151 million disability-adjusted life years (DALYs) lost (~30.0% of all deaths and 14.0% of all DALYs lost). It is a leading cause of morbidity, disability, and mortality worldwide. Further, by 2020, 32.0% of the world population deaths will be caused by CVD, and by 2030; it will be responsible for 33.0% of all deaths (24.2 million) (1).
In Egypt, the National Hypertension Project (NHP) found an adjusted overall prevalence of CAD is 8.3% (2). In Egypt, WHO reports showed in 2014 that CAD deaths reached 107,232 (23.14%) of all deaths. Age-adjusted death rate is186.36/100,000 population; this ranks Egypt #23 in the world]. CAD deaths were 78,897 (21.73%) of all deaths, which made CAD the first killer in Egypt in 2013 (3).
Complications of acute myocardial infarction include left ventricular dysfunction, cardiogenic shock, and structural complications. Other risks include arrhythmia, recurrent chest discomfort, recurrent ischemia or re-infarction, pericardial effusion, pericarditis, and post-myocardial infarction syndrome. Additionally, patients may experience venous thrombosis, pulmonary embolism, left ventricular aneurysm, left ventricular thrombus, and arterial embolism
The combination of rising usage of sensitive myocardial infarction biomarkers and precise imaging techniques, including electrocardiograph (ECG), computed tomography, and cardiac magnetic resonance imaging, made diagnosis of CHD easy and early. During the last 40 years, a decrease in global coronary heart disease mortality has been seen to decline by up to 50% (4).
Diagnosis and triage of patients with suspected acute chest pain secondary to ACS consume a large and increasing amount of healthcare resources. Further, the consequences of missing ACS are both a source of morbidity and mortality in such patients and remain a source of significant malpractice litigation. Therefore, expeditious, safe evaluation of ACP is a pressing need to increase healthcare providers’ efficiency, contain costs, and improve outcomes.
Coronary computed tomography angiography (CTA) has been shown to be very good for prognosticating risk, excluding significant coronary artery disease in stable patients with chest pain, and has a high sensitivity for the identification of significant coronary stenosis. CTA improves the quality of care for patients presenting with acute chest pain, particularly in patients with low to intermediate likelihood of acute coronary syndrome. Coronary CTA offers a rapid evaluation of the degree of coronary stenosis and atherosclerosis, allows a significant reduction in time-to-discharge, and ensures high-risk patients are appropriately triaged to cardiac catheterization.
Because of the increasing use of coronary CTA testing for the evaluation of ACP patients. These recommendations were produced as an educational tool for practitioners evaluating acute chest pain patients, in the interest of developing systematic standards of practice for coronary CTA based on the best available data or broad expert consensus. Due to the highly variable nature of medical care, approaches to patient selection, preparation, protocol selection, interpretation, or reporting that differ from these guidelines may represent an appropriate variation based on a legitimate assessment of an individual patient's needs.
- Scope and Purpose
This guideline targets adult and elderly patients who present with acute chest pain secondary to coronary heart disease. This guideline does not apply to pediatric patients. This Guideline is concerned with the diagnosis of acute chest pain using Cardiac CT and to create clear and actionable recommendations to implement these opportunities in clinical practice.
- The Target Audience
The guideline is intended for:
- Clinicians who are likely to diagnose and manage patients with acute chest pain as Cardiologist, Emergency Department Physicians, Intense Care Physicians, General Medicine Physicians
- Radiologists who interpret CCTA.
- Radiographers who perform CCTA.
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria were followed in the search and retrieval of guidelines to be adapted:
- Selecting only evidence-based guidelines (guidelines must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
· Selecting only national and/or international guidelines
· Selecting peer-reviewed publications only
· Selecting guidelines written in the English language
· Excluding guidelines written by a single author, not on behalf of an organization, to be valid and comprehensive, a guideline ideally requires multidisciplinary input
· Excluding guidelines published without references, as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
· Developing organization/authors
· Date of publication, posting, and release
· Country/language of publication
· Date of posting and/or release
· Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained).
The guidelines development group decided to adopt this guidline from the Society of Cardiovascular Computed Tomography (SCCT), American College of Radiology (ACR) and North American Society for Cardiovascular Imaging (NASCI) (4, 5, 6).
➡️Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of
Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because they represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Table 1 Quality and Significance of the four levels of evidence in GRADE:
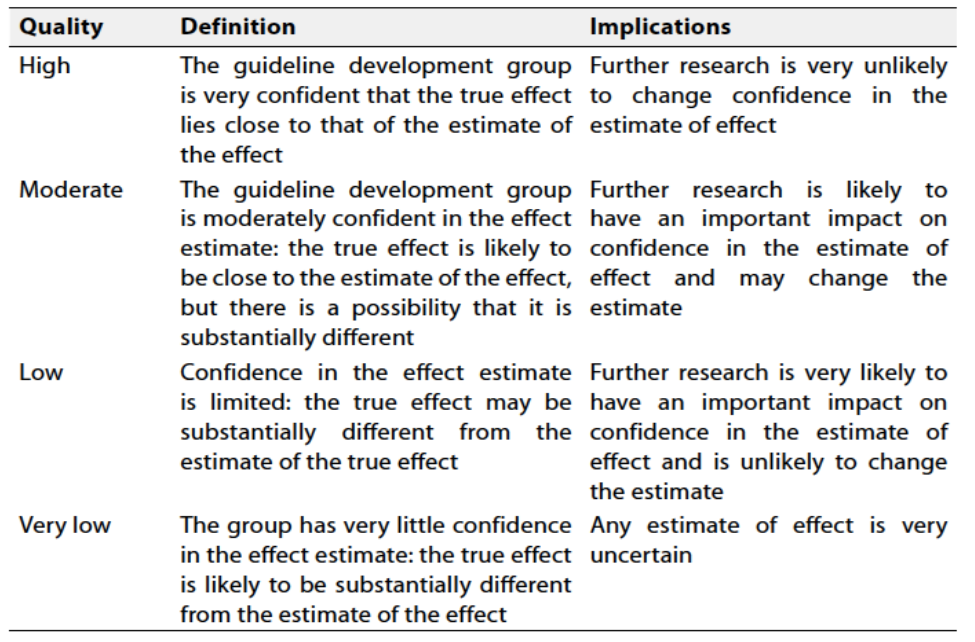
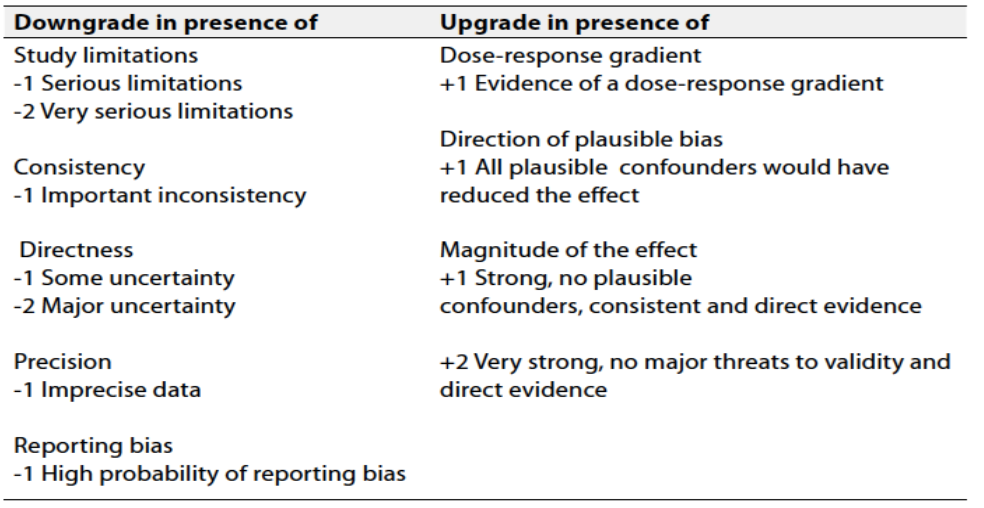
Table 2 Factors that determine How to upgrade or downgrade the quality of evidence
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation should account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
Good practice statements
Statements based on opinions of respected authorities and the guidelines development group.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Clinical Indicators for Monitoring
1. Documentation of acute chest pain in the request form:
- Indicator: The clinician should document the presence of acute chest pain in the radiology request form by writing patient's history, clinical presentation, ECG, and initial biomarker assessment
2. Adequately performing CCTA:
- Indicator: The radiologist should document the main steps of CCTA as preparation of patient , drug administration, CT protocol and post examination care.
3. Structured CCTA report:
- Indicator: In the radiology report ,the radiologist should document technique, medication used ,quality of the study ,imaging findings and radiation dose
4. Timely communicating the CCTA report:
- Indicator: The radiologist should document time of reporting, presence of critical findings and method of communication with the clinician.
These indicators cover aspects such as documentation, diagnostic procedures, drug administration, structural report and method of communication, providing a comprehensive approach to monitoring physician and radiologist’s adherence to the clinical guidelines.
- Implementation and Considerations
- Training courses and hands-on Workshops for radiologists and radiographers
- Research Needs
1. The use of Artificial Intelligence (AI) in enhancing e the use of cardiac CT in clinical practice.
2. Assess the usefulness of algorithms combining non-invasive imaging tests as echocardiography, cardiac CT, MR, and nuclear medicine for evaluation acute coronary syndrome in clinical practice.
- Updating the Guideline
To keep these recommendations up to date and ensure their validity it will be periodically updated. This will be done whenever a piece of strong new evidence is available and necessitates updating.
- Annexes
Fig. 1. Patient-centric algorithm for acute chest pain (6).
- References
1. Centers for Disease Control and Prevention. Coronary Artery Disease (CAD): CDC; 2021 [Available from: https://www.cdc.gov/heartdisease/coronary_ad.htm.
2.WORLD HEALTH RANKINGS. EGYPT: CORONARY HEART DISEASE 2020 [Available from: https://www.worldlifeexpectancy.com/egypt-coronary-heart-disease.
3.Hassanin A, Hassanein M, Bendary A, Maksoud MA. Demographics, clinical characteristics, and outcomes among hospitalized heart failure patients across different regions of Egypt. The Egyptian Heart Journal. 2020;72:1-9.
4.Jia S, Liu Y, Yuan J. Evidence in guidelines for treatment of coronary artery disease. Coronary Artery Disease: Therapeutics and Drug Discovery. 2020:37-73.
5.Narula J, Chandrashekhar Y, Ahmadi A, Abbara S, Berman DS, Blankstein R, et al. SCCT 2021 expert consensus document on coronary computed tomographic angiography: a report of the society of cardiovascular computed tomography. Journal of cardiovascular computed tomography. 2021;15(3):192-217.
6.Maroules CD, Rybicki FJ, Ghoshhajra BB, Batlle JC, Branch K, Chinnaiyan K, et al. 2022 use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: An expert consensus document of the Society of cardiovascular computed tomography (SCCT): Endorsed by the American College of Radiology (ACR) and North American Society for cardiovascular Imaging (NASCI). Journal of cardiovascular computed tomography. 2023;17(2):146-63.
7.Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte Jr M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. Journal of the American college of cardiology. 1990;15(4):827-32.
8.Hecht HS, Blaha MJ, Kazerooni EA, Cury RC, Budoff M, Leipsic J, Shaw L. CAC-DRS: coronary artery calcium data and reporting system. An expert consensus document of the society of cardiovascular computed tomography (SCCT). Journal of cardiovascular computed tomography. 2018;12(3):185-91.
9.Gonzalez JA, Lipinski MJ, Flors L, Shaw PW, Kramer CM, Salerno M. Meta-analysis of diagnostic performance of coronary computed tomography angiography, computed tomography perfusion, and computed tomography-fractional flow reserve in functional myocardial ischemia assessment versus invasive fractional flow reserve. The American journal of cardiology. 2015;116(9):1469-78.
10.Hoffmann U, Truong QA, Schoenfeld DA, Chou ET, Woodard PK, Nagurney JT, et al. Coronary CT angiography versus standard evaluation in acute chest pain. New England Journal of Medicine. 2012;367(4):299-308.
11.Dai T, Wang J-r, Hu P-f. Diagnostic performance of computed tomography angiography in the detection of coronary artery in-stent restenosis: evidence from an updated meta-analysis. European Radiology. 2018;28:1373-82
12.Weustink AC, Nieman K, Pugliese F, Mollet NR, Meijboom BW, van Mieghem C, et al. Diagnostic accuracy of computed tomography angiography in patients after bypass grafting: comparison with invasive coronary angiography. JACC: Cardiovascular imaging. 2009;2(7):816-24.
13.Nørgaard BL, Gaur S, Fairbairn TA, Douglas PS, Jensen JM, Patel MR, et al. Prognostic value of coronary computed tomography angiographic derived fractional flow reserve: a systematic review and meta-analysis. Heart. 2022;108(3):194-202.
14.Branch KR, Haley RD, Bittencourt MS, Patel AR, Hulten E, Blankstein R. Myocardial computed tomography perfusion. Cardiovascular diagnosis and therapy. 2017;7(5):452.
15.Lee H-J, Im DJ, Youn J-C, Chang S, Suh YJ, Hong YJ, et al. Myocardial extracellular volume fraction with dual-energy equilibrium contrast-enhanced cardiac CT in nonischemic cardiomyopathy: a prospective comparison with cardiac MR imaging. Radiology. 2016;280(1):49-57.
16.Cook CM, Petraco R, Shun-Shin MJ, Ahmad Y, Nijjer S, Al-Lamee R, et al. Diagnostic accuracy of computed tomography–derived fractional flow reserve: a systematic review. JAMA cardiology. 2017;2(7):803-10.
17.Patel AR, Bamberg F, Branch K, Carrascosa P, Chen M, Cury RC, et al. Society of cardiovascular computed tomography expert consensus document on myocardial computed tomography perfusion imaging. Journal of cardiovascular computed tomography. 2020;14(1):87-100.
18.American College of Radiology NASoCI, Society for Pediatric Radiology. . ACR–NASCI–SPR practice parameter for the performance and interpretation of cardiac computed tomography (CT). 2021 [Available from: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/CardiacCT.pdf.
19.Lewis MA, Pascoal A, Keevil SF, Lewis CA. Selecting a CT scanner for cardiac imaging: the heart of the matter. The British journal of radiology. 2016;89(1065):20160376.
20.Ghekiere O, Salgado R, Buls N, Leiner T, Mancini I, Vanhoenacker P, et al. Image quality in coronary CT angiography: challenges and technical solutions. The British journal of radiology. 2017;90(1072):20160567.
21.Huda W, Rowlett WT, Schoepf UJ. Radiation dose at cardiac computed tomography: facts and fiction. Journal of thoracic imaging. 2010;25(3):204-12.
22.Hedgire S, Ghoshhajra B, Kalra M. Dose optimization in cardiac CT. Physica Medica. 2017;41:97-103.
23.Abbara S, Blanke P, Maroules CD, Cheezum M, Choi AD, Han BK, et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: A report of the society of Cardiovascular Computed Tomography Guidelines Committee: Endorsed by the North American Society for Cardiovascular Imaging (NASCI). Journal of cardiovascular computed tomography. 2016;10(6):435-49.
24.Scholtz J-E, Ghoshhajra B. Advances in cardiac CT contrast injection and acquisition protocols. Cardiovascular Diagnosis and Therapy. 2017;7(5):439.
25.Sadamatsu K, Koide S, Nakano K, Yoshida K. Heart rate control with single administration of a long-acting β-blocker at bedtime before coronary computed tomography angiography. Journal of Cardiology. 2015;65(4):293-7.
26.Clayton B, Raju V, Roobottom C, Morgan‐Hughes G. Safety of intravenous β‐adrenoceptor blockers for computed tomographic coronary angiography. British Journal of Clinical Pharmacology. 2015;79(3):533-6.
27.Scholtz J-E, Baliyan V, Hedgire S, Mercaldo ND, Pierce TT, Missine GZS, et al. Randomized trial comparing transdermal with sublingual nitroglycerin administration for coronary vasodilation in CTA. JACC: Cardiovascular Imaging. 2019;12(9):1890-3.
28.Nguyen ET, Green CR, Adams SJ, Bishop H, Gleeton G, Hague CJ, et al. CAR and CSTR Cardiac Computed Tomography (CT) Practice Guidelines: Part 2-Non-Coronary Imaging. Canadian Association of Radiologists Journal. 2024:08465371241233228.
29. 2020 SCCT Guideline for Training Cardiology and Radiology Trainees as Independent Practitioners (Level II) and Advanced Practitioners (Level III) in Cardiovascular Computed Tomography: A Statement from the Society of Cardiovascular Computed Tomography , Choi, Andrew D. et al. Journal of Cardiovascular Computed Tomography, Volume 15, Issue 1, 2 - 15
30.Hartung MP, Bickle IC, Gaillard F, Kanne JP. How to create a great radiology report. Radiographics. 2020;40(6):1658-70.
31.American College of Radiology. ACR practice parameter for communication of diagnostic imaging findings. 2020 [Available from: https://www.acr.org/-/media/ACR/Files/PracticeParameters/CommunicationDiag.pdf.
32.Cury RC, Leipsic J, Abbara S, Achenbach S, Berman D, Bittencourt M, et al. CAD-RADS™ 2.0–2022 coronary artery disease-reporting and data system: an expert consensus document of the society of cardiovascular computed tomography (SCCT), the American college of cardiology (ACC), the American college of radiology (ACR), and the North America society of cardiovascular imaging (NASCI). Cardiovascular Imaging. 2022;15(11):1974-2001.
33.Leipsic J, Abbara S, Achenbach S, Cury R, Earls JP, Mancini GJ, et al. SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. Journal of cardiovascular computed tomography. 2014;8(5):342-58.