Surgical Management of Ulcerative Colitis
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | جراحه عامه |
| كتاب: | Surgical Management of Ulcerative Colitis |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:51 AM |
الوصف
"last update: 19 May 2026" Download Guideline
- Executive summary
These guidelines offer evidence-based recommendations on the targeted levels of clinical practice guidelines and provide healthcare professionals with practice guidance on the surgical management of ulcerative colitis disease and its complications.
· We advise diagnosing UC through the correlation of clinical, biochemical, endoscopic, and histopathologic aspects, (Conditional recommendation).
· We advise clinically diagnosing UC by the presence of chronic diarrhea with mucus and blood, straining and rectal tenesmus, nocturnal stools, weight loss, fever, and abdominal pain, (Conditional recommendation).
· We advise performing a complete blood count, acute-phase reactants (erythrocyte sedimentation rate, C-reactive protein), liver function tests, and stool tests as the initial laboratory approach in patients suspected of presenting with UC, (Conditional recommendation).
· We advise performing fecal calprotectin and fecal lactoferrin levels to assess mucosal cicatrization or endoscopy to assess remission. (Conditional recommendation).
· We advise performing plain abdominal x-ray to rule out toxic megacolon and a chest x-ray to rule out colon perforation in patients with severe UC, (Conditional recommendation).
· We advise using the Truelove and Witts index and the Mayo score for evaluating the grade of UC activity, (Conditional recommendation).
· We advise performing colonoscopy with ileocecal valve intubation as the diagnostic method of choice for evaluating the extension and grade of disease activity, (Conditional recommendation).
· We advise performing at least two biopsies to be taken per segment at the level of the terminal ileum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum, including normal zones of the mucosa, to microscopically make the diagnosis and determine disease extension, (Conditional recommendation).
· We advise diagnosing dysplasia through the Vienna classification by at least two pathologists, (Conditional recommendation).
· We advise performing surgery for patients with confirmed diagnosis (through clinical, radiologic, and laboratory parameters) who do not improve with intravenous steroids within the first 72 hours, (Conditional recommendation).
· Surgery is recommended to corticosteroid-dependent patients, as well as immunomodulator refractory patients (Strong recommendation).
· We recommend a multidisciplinary approach to guide optimal care in hospitalized patients with moderate-to-severe UC before surgical intervention, (Strong recommendation).
· We advise a shared decision-making approach to tailor procedure selection to the patient’s preference, (Conditional recommendation).
· We advise weaning steroids before restorative proctocolectomy, (Conditional recommendation).
· We advise against performing single-stage restorative proctocolectomy in patients receiving biologics, (Conditional recommendation).
· We advise prophylactic anticoagulation therapy in adult patients with active UC during hospitalization, considering the high risk of venous thromboembolism during UC flares, (Conditional recommendation).
· We advise correction of nutrition imbalances preoperatively, (Good practice statement).
· We advise performing appendectomy to decrease the need for proctocolectomy related to medically refractory disease, (Conditional recommendation).
· Patients with UC undergoing proctectomy should be counseled regarding possible effects on fertility, pregnancy, sexual function, and urinary function, (Strong recommendation).
· Total proctocolectomy (with IPAA, end ileostomy, or continent ileostomy) is recommended for patients with UC undergoing elective surgery, (Strong recommendation).
· For patients with UC undergoing restorative total proctocolectomy with IPAA, 2-stages, modified 2-stages, and 3-stages all are accepted approaches, (Strong recommendation).
· IPAA is not recommended in case of fecal incontinence, intermediate colitis or low rectal cancer on top of ulcerative colitis, (Good practice statement).
· We advise performing a staged approach for an IPAA in patients being treated with high-dose corticosteroids or monoclonal antibodies, (Conditional recommendation).
· Total abdominal colectomy with ileorectal anastomosis may be considered in selected patients who have UC with relative rectal sparing, (Conditional recommendation).
· We advise performing a “rescue” diverting loop ileostomy in the setting of worsening, acute, severe UC to potentially avoid an emergent total abdominal colectomy, (Conditional recommendation).
· We advise performing reconstructive surgery to refractory and corticosteroid-dependent patients as it improves the quality of life despite the risk of early and late complications, (Conditional recommendation).
· We advise performing laparoscopic surgery to patients with medically refractory UC, as it is associated with lower intra- and postoperative morbidity, faster recovery, fewer adhesions and incisional hernias, shorter hospital length of stay, improved female fertility, and better cosmoses, (Conditional recommendation).
· For patients with severe medically refractory UC, fulminant colitis, toxic megacolon, or colonic perforation, we advise performing total abdominal colectomy with end ileostomy, (Conditional recommendation).
· Endoscopic surveillance is recommended for patients with visible polypoid or non-polypoid dysplasia that is completely excised endoscopically, (Strong recommendation).
· Total proctocolectomy with or without IPAA is recommended for patients with visible dysplasia not amenable to endoscopic excision, invisible dysplasia in the flat mucosa surrounding a visible dysplastic lesion, or colorectal adenocarcinoma, (Strong recommendation).
· Total proctocolectomy is recommended for patients confirmed to have invisible multifocal, low-grade dysplasia or any invisible high-grade dysplasia, (Strong recommendation).
· We advise performing restorative proctocolectomy in patients with carcinoma or multifocal high-grade or low-grade dysplasia, (Conditional recommendation).
· We advise extended postoperative venous thromboembolism prophylaxis in patients with UC exposed to tofacitinib, (Conditional recommendation).
· We advise against surveillance or follow-up of the ileo-anal pouch in the asymptomatic patient, unless there are risk factors, such as a history of neoplasia or primary sclerosing cholangitis, (Conditional recommendation).
· We advise prescribing 500 mg of ciprofloxacin twice a day or 15-20 mg/kg/day of metronidazole for 2 weeks as the first-line treatment in patients with acute pouchitis, (Conditional recommendation).
- Recommendations
Section 1. Diagnosis of UC:
· We advise diagnosing UC through the correlation of clinical, biochemical, endoscopic, and histopathologic aspects, (Conditional recommendation, low certainty evidence, (6)).
· We advise clinically diagnosing UC by the presence of chronic diarrhea with mucus and blood, straining and rectal tenesmus, nocturnal stools, weight loss, fever, and abdominal pain, (Conditional recommendation, low certainty evidence, (6)).
· We advise performing a complete blood count, acute-phase reactants (erythrocyte sedimentation rate, C-reactive protein), liver function tests, and stool tests as the initial laboratory approach in patients suspected of presenting with UC, (Conditional recommendation, low certainty evidence, (6)).
· We advise performing fecal calprotectin and fecal lactoferrin levels to assess mucosal cicatrization or endoscopy to assess remission. (Conditional recommendation, moderate certainty evidence, (6)).
· We advise performing plain abdominal x-ray to rule out toxic megacolon and a chest x-ray to rule out colon perforation in patients with severe UC, (Conditional recommendation, low certainty evidence, (6)).
· We advise using the Truelove and Witts index and the Mayo score for evaluating the grade of UC activity, (Conditional recommendation, low certainty evidence, (6)), (table 3 & 4).
· We advise performing colonoscopy with ileocecal valve intubation as the diagnostic method of choice for evaluating the extension and grade of disease activity, (Conditional recommendation, low certainty evidence, (6)).
· We advise performing at least two biopsies to be taken per segment at the level of the terminal ileum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum, including normal zones of the mucosa, to microscopically make the diagnosis and determine disease extension, (Conditional recommendation, low certainty evidence, (6)).
· We advise diagnosing dysplasia through the Vienna classification by at least two pathologists, (Conditional recommendation, low certainty evidence, (6)), (table 7).
Section 2. Indications of surgical treatment:
· We advise performing surgery for patients with confirmed diagnosis (through clinical, radiologic, and laboratory parameters) who do not improve with intravenous steroids within the first 72 hours, (Conditional recommendation, moderate certainty evidence, (5)).
· Surgery is recommended to corticosteroid-dependent patients, as well as immunomodulator refractory patients (Strong recommendation, moderate certainty evidence, (5)).
Section 3. Preoperative optimization of refractory moderate-to-severe UC:
· We recommend a multidisciplinary approach to guide optimal care in hospitalized patients with moderate-to-severe UC before surgical intervention, (Strong recommendation, moderate certainty evidence, (4)).
· We advise a shared decision-making approach to tailor procedure selection to the patient’s preference, (Conditional recommendation, low certainty evidence, (5)).
· We advise weaning steroids before restorative proctocolectomy, (Conditional recommendation, low certainty evidence, (5)).
· We advise against performing single-stage restorative proctocolectomy in patients receiving biologics, (Conditional recommendation, very low certainty evidence, (5)).
· We advise prophylactic anticoagulation therapy in adult patients with active UC during hospitalization, considering the high risk of venous thromboembolism during UC flares, (Conditional recommendation, very low certainty evidence, (5)).
· We advise correction of nutrition imbalances preoperatively, (Good practice statement).
· We advise performing appendectomy to decrease the need for proctocolectomy related to medically refractory disease, (Conditional recommendation, moderate certainty evidence, (4)).
· Patients with UC undergoing proctectomy should be counseled regarding possible effects on fertility, pregnancy, sexual function, and urinary function, (Strong recommendation, moderate certainty evidence, (4)).
Section 4. Surgical treatment of UC:
· Total proctocolectomy (with IPAA, end ileostomy, or continent ileostomy) is recommended for patients with UC undergoing elective surgery, (Strong recommendation, moderate certainty evidence, (4)).
· For patients with UC undergoing restorative total proctocolectomy with IPAA, 2-stages, modified 2-stages, and 3-stages all are accepted approaches, (Strong recommendation, moderate certainty evidence, (4)).
· IPAA is not recommended in case of fecal incontinence, intermediate colitis or low rectal cancer on top of ulcerative colitis, (Good practice statement).
· We advise performing a staged approach for an IPAA in patients being treated with high-dose corticosteroids or monoclonal antibodies, (Conditional recommendation, low certainty evidence, (4)).
· Total abdominal colectomy with ileorectal anastomosis may be considered in selected patients who have UC with relative rectal sparing, (Conditional recommendation, moderate certainty evidence, (5 & 6)).
· We advise performing a “rescue” diverting loop ileostomy in the setting of worsening, acute, severe UC to potentially avoid an emergent total abdominal colectomy, (Conditional recommendation, low certainty evidence, (5)).
· We advise performing reconstructive surgery to refractory and corticosteroid-dependent patients as it improves the quality of life despite the risk of early and late complications, (Conditional recommendation, low certainty evidence, (5)).
· We advise performing laparoscopic surgery to patients with medically refractory UC, as it is associated with lower intra- and postoperative morbidity, faster recovery, fewer adhesions and incisional hernias, shorter hospital length of stay, improved female fertility, and better cosmoses, (Conditional recommendation, moderate certainty evidence, (5)).
· For patients with severe medically refractory UC, fulminant colitis, toxic megacolon, or colonic perforation, we advise performing total abdominal colectomy with end ileostomy, (Conditional recommendation, moderate certainty evidence, (4 & 6)).
· Endoscopic surveillance is recommended for patients with visible polypoid or non-polypoid dysplasia that is completely excised endoscopically, (Strong recommendation, moderate certainty evidence, (4)).
· Total proctocolectomy with or without IPAA is recommended for patients with visible dysplasia not amenable to endoscopic excision, invisible dysplasia in the flat mucosa surrounding a visible dysplastic lesion, or colorectal adenocarcinoma, (Strong recommendation, moderate certainty evidence, (4)).
· Total proctocolectomy is recommended for patients confirmed to have invisible multifocal, low-grade dysplasia or any invisible high-grade dysplasia, (Strong recommendation, moderate certainty evidence, (4)).
· We advise performing restorative proctocolectomy in patients with carcinoma or multifocal high-grade or low-grade dysplasia, (Conditional recommendation, moderate certainty evidence, (6)).
Section 6. Post-operative:
· We advise extended postoperative venous thromboembolism prophylaxis in patients with UC exposed to tofacitinib, (Conditional recommendation, low certainty evidence, (4)).
· We advise against surveillance or follow-up of the ileo-anal pouch in the asymptomatic patient, unless there are risk factors, such as a history of neoplasia or primary sclerosing cholangitis, (Conditional recommendation, low certainty evidence, (6)).
· We advise prescribing 500 mg of ciprofloxacin twice a day or 15-20 mg/kg/day of metronidazole for 2 weeks as the first-line treatment in patients with acute pouchitis, (Conditional recommendation, moderate certainty evidence, (6)).
- Acknowledgement
We would like to acknowledge the Guideline Development Group, (GDG) committee for developing these guidelines.
Chair of GDG: Mostafa Abdel-Hamed Soliman, Professor of Surgery, Cairo University.
Moderator of GDG: Mohamed Ali Mohamed Nada, Professor of Surgery, Ain Shams University.
Members of GDG (Alphabetically):
Abdel-Wahab Mohamed Ezzat, Professor of Surgery, Ain Shams University.
Ahmed Abdel-Raouf Elgeidie, Professor of Digestive Surgery, Mansoura University.
Alaa Abdallah, Professor of Surgery, Ain Shams University.
Atef Abdel-Ghani Salem, Professor of Surgery, Benha University.
Hesham Abdel-Raouf El-Akkad, Professor of Surgery, Ain Shams University.
Ibrahim El-Zayat, Head of Surgery Department, Aswan University.
Khaled Abdallah El-Fiky, Professor of Surgery, Ain Shams University.
Khaled Amer, Professor of Surgery, Military Medical Academy.
Khaled Safwat, Professor of Surgical Oncology and Endoscopy, Zagazig University.
Mohamed Ibrahim Abdel-Hamed Al-Said, Professor of Surgery, Zagazig University.
Tarek Ibrahim, Professor of Surgery, National Liver Institute, Menofia University.
- Abbreviations
5ASAs 5-AminoSalicylates
|
AGREE II |
Appraisal of Guidelines for Research and Evaluation II |
|
ASCRS |
American Society of Colon and Rectal Surgeons |
|
CRP |
C Reactive Protein |
|
ECCO |
European Crohn’s and Colitis Organization |
|
ESR |
Erythrocyte Sedimentation Rate |
|
GDG |
Guideline Development Group |
|
GRADE |
Grade of Recommendations, Assessment, Development and Evaluation |
|
IBD |
Inflammatory Bowel Disease |
|
IBDU |
Inflammatory Bowel Disease Unclassified |
|
IPAA |
Ileal Pouch-Anal Anastomosis |
|
UC |
Ulcerative Colitis |
|
WHO |
World Health Organization |
- Glossary
There is a common agreement has been reached by the Consensus about frequently used terms. Such terms reflect clinical decision-making and are considered helpful as a consequence. Ulcerative colitis (UC) is a chronic inflammatory condition causing continuous mucosal inflammation of the colon without granulomas on biopsy, affecting the rectum and a variable extent of the colon in continuity, which is characterized by a relapsing and remitting course,(1).
IBD unclassified (IBDU) is the term best suited for the minority of cases where a definitive distinction between UC, Crohn's disease, or other cause of colitis cannot be made after the history, endoscopic appearances histopathology of multiple mucosal biopsies and appropriate radiology have been taken into account, (1).
Indeterminate colitis is a term reserved for pathologists to describe a colectomy specimen which has overlapping features of ulcerative colitis and Crohn's disease. It has distinct prognostic factors related to further surgery, (1).
Distribution of disease: The Consensus favors use of the Montréal classification, (Table1) for defining the distribution of disease, (Table 2). This is used to describe the maximal, macroscopic extent of disease at colonoscopy. The implications of more extensive microscopic disease are still not understood, (2).
Disease onset: There is some evidence to suggest that patients with UC stratified by age (A1: <16; A2:16–40 and A3: >40 years) have different outcomes. Patients diagnosed before the age of 16 had a more aggressive initial course, while older age at diagnosis was found to be associated with a lower risk of colectomy. There is also some evidence that UC diagnosed in the very young has a different etiology and prognosis, (2).
Active disease: Clinical disease activity is grouped into remission, mild, moderate and severe. This refers to biological activity and not to treatment-responsiveness. Our Consensus participants considered Truelove and Witts' criteria useful in clinical practice (Table 3), in conjunction with sigmoidoscopy to confirm active colitis. However, there is other classifications frequently used specially by gastroenterologists, (1).
The term severe colitis (or ‘acute severe colitis’) is preferred to ‘fulminant’ colitis, because the term ‘fulminant’ is ill-defined. Severe colitis as defined according to Truelove and Witts' criteria is easy to apply in outpatients, mandates hospital admission for intensive treatment and defines an outcome (only 70% respond to intensive therapy) , (1).
Moderate colitis has become necessary to distinguish from mildly active disease, because the efficacy of some treatments may differ. The simplest clinical measure to distinguish moderate from mildly active colitis is the presence of mucosal friability (bleeding on light contact with the rectal mucosa at sigmoidoscopy). The technique of assessing mucosal friability at flexible sigmoidoscopy has yet to be standardized, (1).
Remission is defined as complete resolution of symptoms and endoscopic mucosal healing. In clinical practice, there is an agreement that ‘remission’ meant a stool frequency ≤3/day with no bleeding and no urgency. Remission defined by individual patients has an 86% sensitivity and 76% specificity for a regulatory-defined remission (absence of visible blood and absent mucosal friability), indicating that sigmoidoscopy to confirm mucosal healing is generally unnecessary in practice, (3).
Response is defined as clinical and endoscopic improvement, depending on the activity index used (table 4). In general, this means a decrease in the activity index plus a decrease in the rectal bleeding and endoscopy sub-scores, (3).
Relapse: The term relapse is used to define a flare of symptoms in a patient with established UC who is in clinical remission, either spontaneously or after medical treatment. Rectal bleeding an essential component of relapse, and we believe that a combination of rectal bleeding with an increase in stool frequency and abnormal mucosa at sigmoidoscopy was necessary to define relapse. In clinical trials, the criteria for relapse should be predefined with the score that is being used for an individual study.
Early relapse an arbitrary, but clinically relevant period of 3 months after achieving remission on previous therapy defines early relapse. The therapeutic significance needs to be defined. Pattern of relapse may be infrequent (≤1/year), frequent (≥2relapses/ year), or continuous (persistent symptoms of active UC without a period of remission). Although the terms are arbitrary, they are considered clinically relevant and care should be taken to distinguish between terms that describe disease activity at a point in time and those that describe the longitudinal pattern (or ‘behavior’) of the disease), (3).
The term ‘chronic active disease’ has been used in the past to define a patient who is dependent on, refractory to, or intolerant of steroids, or who has disease activity despite immunomodulators. Since this term is ambiguous it is best avoided. Instead, arbitrary, but more precise definitions are preferred, including steroid refractory or steroid-dependence.
Steroid-refractory colitis: Patients who have active disease despite prednisolone up to 0.75 mg/kg/day over a period of 4 weeks. The definition is consistent with the definition for steroid-refractory Crohn's disease; however, it is likely to evolve, with a reduction in the duration of steroid therapy as the threshold for biologic therapy changes.
Steroid-dependent colitis: Patients who are either unable to reduce steroids below the equivalent of prednisolone 10 mg/day within 3 months of starting steroids, without recurrent active disease, or who have a relapse within 3 months of stopping steroids. As with steroid-refractoriness, the definition is likely to evolve as the threshold for biologic therapy changes. There is an agreement that steroid-dependence requires that the total duration of steroids does not exceed 3 months before a threshold equivalent to prednisolone 10 mg/day is reached. Patients are still considered steroid-dependent if they relapse within 3 months of stopping steroids. Although these limits are arbitrary, they serve as guidance for clinical practice and may be used for uniformity in clinical trials. The aim should be to withdraw steroids completely, (3).
Immunomodulator-refractory colitis: Patients who have active disease or relapse in spite of thiopurines at an appropriate dose for at least 3 months (i.e. azathioprine 2–2.5 mg/kg/day or mercaptopurine 1 1.5 mg/kg/day in the absence of leucopenia). The definition is arbitrary, but has increasing clinical relevance when deciding on the place of biological therapy or surgery.
Refractory distal colitis defined as persistent symptoms due to colonic inflammation confined to the rectum (proctitis), or left-side of the colon, despite treatment with oral plus topical steroids and 5ASAs for 4–8 weeks. This represents a common clinical dilemma, although whether it is a separate entity is unclear, (3).
New patient: A patient with active UC presenting at, or shortly after diagnosis, with no previous therapy for UC
Complementary therapies: Treatments used alongside conventional medicine.- Introduction
Ulcerative colitis is a lifelong disease arising from an interaction between genetic and environmental factors, observed predominantly in the developed countries of the world. The precise etiology is unknown and therefore medical therapy to cure the disease is not yet available. Patients may live with a considerable symptom burden despite medical treatment (66% describe interference with work and 73% with leisure activities) in the hope that the etiology of ulcerative colitis will shortly be revealed and a cure emerge. Despite randomized trials there will always be many questions that can only be answered by the exercise of judgement and opinion, (1).
Currently several national guidelines are available, most of which are not updated. The guidelines committee of GDG decided in 2025 to develop a national guideline for the surgical management of ulcerative colitis and its complications, acknowledging that it will be a compromise of American Society of Colon and Rectal Surgeons (ASCRS) guidelines, (4), European Crohn’s and Colitis Organization (ECCO) guidelines, (5) and the Mexican consensus on the diagnosis and treatment of ulcerative colitis 2018, (6).
- Scope and purpose
The scope of these guidelines is to establish a national guidelines for UC patients as regard surgical treatment of the disease and its complications as regard the need for surgery, timing, and type of surgery to achieve a best outcome as much as we can.
The main purposes of these guidelines are to minimize malpractice and poor surgical decision, to improve the quality of medical care and surgical service, to provide the best clinical practice to our patients, and finally to reduce the cost of medical service.
- Target audience
The principle targeted audiences are the practicing surgeons, however, gastroenterologists, ICU specialists and nursing staff may be included as well.
- Methods
A comprehensive search for guidelines was undertaken to identify the relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
• Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence)
• Selecting only national and/or international guidelines
• Specific range of dates for publication (using Guidelines published or updated in 2018 and later)
• Selecting peer reviewed publications only
• Selecting guidelines written in English language
• Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
• Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations
The following characteristics of the retrieved guidelines were summarized in:
• Developing organization/authors
• Date of publication, posting, and release
• Country/language of publication
• Date of posting and/or release
• Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point (any guideline scoring above 50% on the rigor dimension was retained). The GDG decided to adapt the American Society of Colon and Rectal Surgeons clinical practice guidelines 2020,(4), the European Crohn's and Colitis Organization (ECCO) guidelines 2022,(5) and the Mexican consensus on the diagnosis and treatment of ulcerative colitis 2018,(6).
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Specifically, the quality of evidence was graded as ‘High’, ‘Moderate’, ‘Low’ or ‘Very low’, (table 5& 6).
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
these are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Research needs
1. The prevalence of UC in Egyptian population.
2. Timing and type of surgery offered for a patient with UC.
3. The use of robotic surgery in era of surgical management of UC.
4. Endoscopic management of UC associated dysplasia are needed.
5. Role of Appendectomy in prevention of proctocolectomy in UC.
- Clinical indicators of monitoring
1. CBC, CRP, ESR, Liver function tests, stool tests.
2. Plain X-Ray abdomen and chest.
3. Colonoscopy.
4. Biopsy.
5. Documentation of the indication of surgery in UC.
6. Documentation of the type of operation.
- Updating of the guideline
The GDG committee for guidelines development is responsible for the continuous evaluation of evidence available about ulcerative colitis. The present guidelines will be updated in case of significant changes based on new evidence.
- Annexes
Table 1: Montreal classification of disease activity in UC, (1).
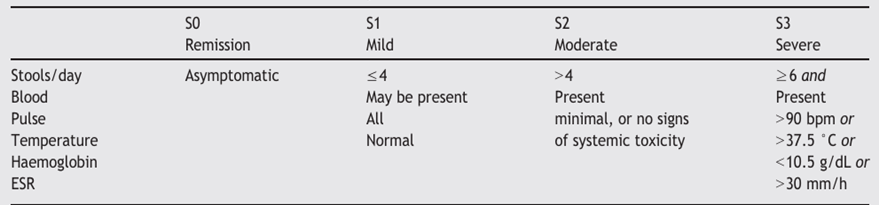
Table 2: Distribution of UC, (2).
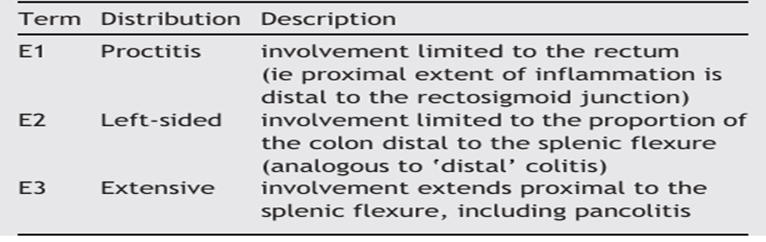
Table 3: Disease activity in UC Truelove and Witts, (1).
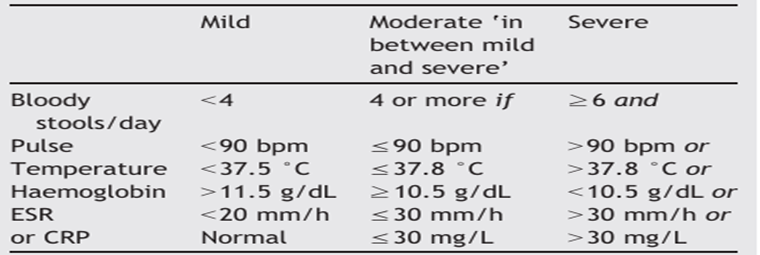
Table 4: Mayo score, (3).

Table 5: Quality and Significance of the four levels of evidence in GRADE:
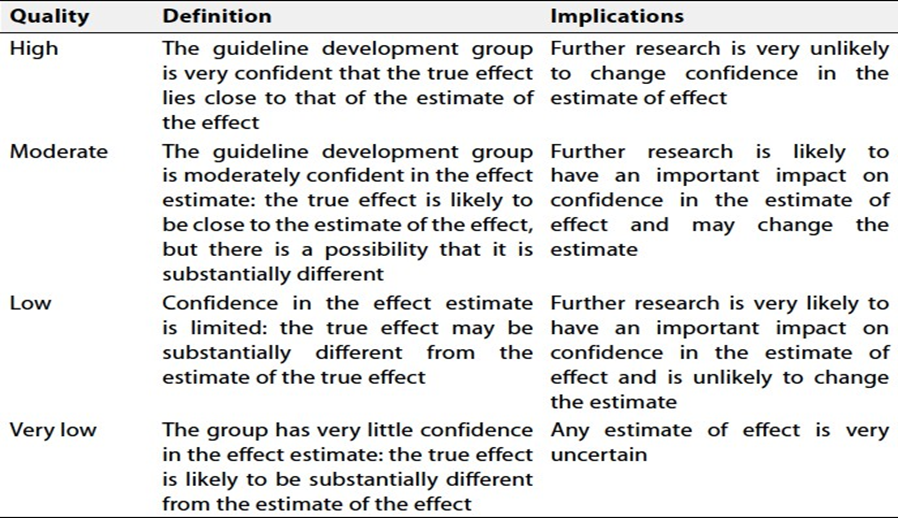
Table 6: Factors that determine How to upgrade or downgrade the quality of evidence
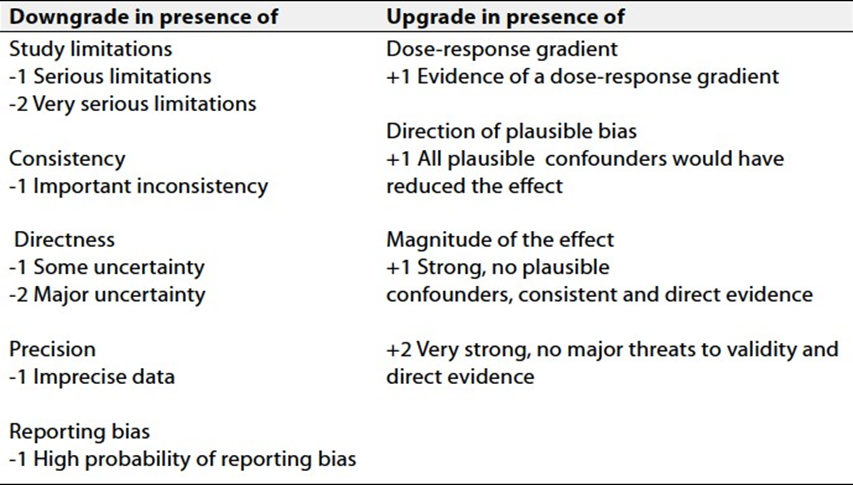
Table 7: Vienna classification for histological classification of colorectal polyps, (7).
|
Category |
Diagnosis |
|
Group 1 |
Negative for dysplasia |
|
Group 2 |
Indefinite for dysplasia |
|
Group 3 |
Mucosal low grade neoplasia - Low grade adenoma - Low grade dysplasia |
|
Group 4 - Subgroup 4.1 - Subgroup 4.2 - Subgroup 4.3 - Subgroup 4.4 |
Mucosal high grade neoplasia - High grade adenoma/dysplasia - Carcinoma in situ - Suspicious for invasive carcinoma - Intramucosal carcinoma |
|
Group 5 |
Submucosal invasion by carcinoma |
- References
1. Dignass A, Eliakim R, Magro F, Maaser C, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis Part 1: Definitions and diagnosis. Journal of Crohn’s and Colitis 2012; 6: 965-990.
2. Silverberg MS, Satsangi J, Ahmad T, Arnott ID, Bernstein CN, Brant SR, et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a working party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol 2005;19(Suppl A):5–36.
3. D'Haens G, Sandborn WJ, Feagan BG, Geboes K, Hanauer SB, Irvine EJ, et al. A review of activity indices and efficacy end points for clinical trials of medical therapy in adults with ulcerative colitis. Journal of Gastroenterol 2007; 132: 763–86.
4. Stefan D. Holubar, Amy L. Lightner, Vitaliy Poylin, Jon D. Vogel et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Surgical Management of Ulcerative Colitis. Dis Colon Rectum 2021; 64: 783–804.
5. Spinelli A, Bonovas S, Burisch J, Kucharzik T, et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Surgical Treatment. Journal of Crohn's and Colitis 2022; 16: 179–189.
6. Yamamoto-Furushoa JK, Gutiérrez-Grobea Y, López-Gómezb JG, Bosques-Padillac F, Rocha-Ramírezd JL. Mexican Consensus on Ulcerative Colitis Working Group. The Mexican consensus on the diagnosis and treatment of ulcerative colitis. Revisita de Gastroenterologia de Mexico 2018; 83 (2): 144-167. www.elsevier.es/rgmx
7. Ooda S A, Asser M L, Alhassafi M Y, Alsedefy A S and Lashen S A. Distribution of colorectal polyps according to Paris and Vienna classification systems: a prospective cohort single center study. Senses Sci (Educ Sci Tech) 2023: 10 (2) :87-98 doi: 10.14616/sands-2023-1-8798.