Metabolic disorders in Ruminant, Ketosis, Ketonemia ,Woody cow syndrome
| Site: | EHC | Egyptian Health Council |
| Course: | Large ruminant Medicine and surgery Guidelines |
| Book: | Metabolic disorders in Ruminant, Ketosis, Ketonemia ,Woody cow syndrome |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:55 AM |
Description
"last update: 19 May 2026" Download Guideline
- Acknowledgment
We would like to acknowledge the committee of the National Egyptian Guidelines for Veterinary Medical Interventions, Egyptian Health Council for adapting this guideline.
Executive Chief of the Egyptian Health Council: Prof. Mohamed Mustafa Lotief.
Head of the Committee: Prof. Ahmed M Byomi
The rapporteur of the Committee: Prof. Mohamed Mohamedy Ghanem.
Scientific Group Members: Prof. Nabil Yassien, Prof. Ashraf Aldesoky Shamaa, Prof. Amany Abbas, Prof. Dalia Mansour, Dr Essam Sobhy Dr Mohamed Elsharkawy, Prof. Dr Gamal A. Sosa., Dr Naglaa Radwan, Dr Hend El Sheikh
Editor/Author: Prof. Mohamed Ghanem
- Definition
Ketosis, also called acetonemia or ketonemia, is one of the most common metabolic disorders in high‑producing dairy cows and bufflaos. It typically occurs during early lactation, when energy demands for milk synthesis exceed dietary energy intake, causing cows to enter a state of negative energy balance (NEB). This results in excessive fat mobilization and increased production of ketone bodies (β‑hydroxybutyrate (BHBA), acetoacetate, and acetone). Ketosis has economic impact as it significantly reduces milk yield, fertility, and overall herd profitability.
- Classification of Ketosis
1-Primary (Nutritional) Ketosis: Occurs when feed intake fails to meet energy requirements during early lactation. This is the most common form.
2-Secondary Ketosis: Results from other conditions that reduce appetite:
- Displaced abomasum
- Mastitis
- Metritis
- Retained placenta
- Lameness
2.3. Clinical vs. Subclinical Ketosis
- Clinical Ketosis: Noticeable symptoms (anorexia, emaciation, and reduced milk yield).
- Subclinical Ketosis (SCK): Elevated BHBA without visible signs. Highly economically significant. Subclinical ketosis can affect 15–30% of dairy herds.
- Etiology
Ketosis develops when:
1. Energy intake < energy demand in early lactation.
2. The cow mobilizes stored fat → increased non‑esterified fatty acids (NEFAs).
3. The liver incompletely oxidizes NEFAs → ketone body accumulation.
Predisposing factors:
- High milk-producing cows
- Overconditioned cows at calving (Body Condition Score > 3.75)
- Poor-quality or low-energy rations
- Stress, overcrowding
- Sudden feed changes
- Pathogenesis
1-Negative Energy Balance (NEB)
After calving, milk production increases rapidly, but feed intake lags. Energy deficit triggers adipose tissue lipolysis.
2-Liver Overload
Mobilized NEFAs enter the liver, where they are:
- Completely oxidized → CO₂ + ATP
- Partially oxidized → ketone bodies
- Esterified → triglycerides, contributing to fatty liver
3- Ketone Accumulation
High levels of BHBA and acetoacetate lead to:
- Suppressed appetite
- Reduced rumen motility
- Further worsening of NEB
4- Neurological Form (Nervous Ketosis)
High ketone levels alter brain metabolism → licking, chewing, head pressing, hyperexcitability.
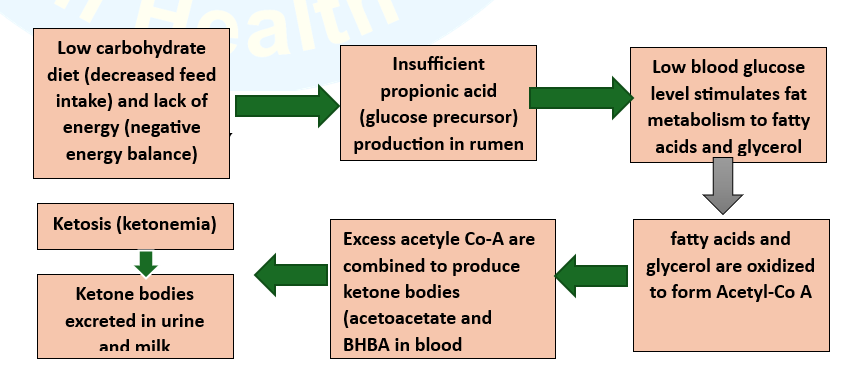
Diagram summarizing the pathogenesis of ketosis in cattle
How NEB is produced in cattle
· Around calving, lactating dairy cows naturally decrease dry matter intake (DMI) due to the advanced gestation stage, as well as metabolic changes which occur in this period. This DMI decrease leads to a NEB.
· During the last week of fetal development, the fetus uses approximately 46% of maternal glucose.
· The onset of milk production makes this energy shortage more remarkable. The mammary gland requires a large amount of glucose for milk lactose synthesis when lactation starts.
- Clinical Signs
1- Clinical Ketosis (digestive form)
- Reduced milk yield
- Selective anorexia (refuse eating of concentrate)
- Weight loss and decreased body condition score
- Firm, dry feces
- Acetone odor on breath or milk
- Decreased rumen motility

Figure (3): Emaciation in buffalo affected with ketosis
2- clinical ketosis (nervous form)
- Excessive licking, chewing
- Head pressing
- Ataxia or incoordination
- Muscle tremors
3-Subclinical Ketosis
No visible signs, but the cattle have:
- Reduced milk yield
- Reduced reproductive performance
- Higher risk of displaced abomasum and metritis
- Diagnosis
1-Laboratory Tests
- Blood BHBA > 1.2 mmol/L: Subclinical ketosis
- Blood BHBA > 3.0 mmol/L: Clinical ketosis
- Elevated NEFAs (prepartum > 0.3 mEq/L, postpartum > 0.6 mEq/L)
- Blood glucose estimation: glucose level less than 40 mg/dl, total blood ketones >30 mg/dl, and milk ketones >10 mg/dl is indicative of ketosis.
2- Urine Tests
Detect acetoacetate and acetone using nitroprusside sticks.
3- Milk Tests
Commercial milk ketone tests (Ketotest, KetoCheck).
4-Clinical and case history
- Early lactation in High-producing cow
- Recent decrease in appetite
· Comparative diagnosis and treatment of clinical ketosis and subclinical ketosis in dairy cows.
|
Aspect |
Clinical ketosis |
Subclinical ketosis |
|
Definition |
A significant metabolic disorder with visible clinical signs |
No obvious clinical signs, but elevated ketone bodies in the blood |
|
Incidence rate |
Lower (approximately 2%−10%) |
Higher (approximately 10%−40%) |
|
Clinical signs |
- Reduced or loss of appetite - Decreased milk production - Weight loss - Depression or neurological signs (e.g., circling, licking objects) - Acetone odor in breath or milk |
No obvious clinical signs, but may have slight declines in production performance |
|
Diagnostic methods |
- Observation of clinical signs - Blood BHBA test (>3.0 mmol/L) - Urine or milk ketone test (strong positive) |
- Blood BHBA test (1.2–3.0 mmol/L) - Milk or urine ketone test (weak positive) |
|
Treatment |
- Intravenous glucose infusion (500.0 ml of 50% glucose solution) - Oral propylene glycol (300.0–500.0 ml/day for 3–5 days) - Supplementation with vitamin B12 and corticosteroids (if necessary) - Adjust diet to increase digestible carbohydrates |
- Oral propylene glycol (200.0-300.0 ml/day for 3–5 days) - Adjust diet to optimize energy balance - Supplementation with vitamins and minerals |
|
Prevention |
- Formulate a balanced diet to avoid negative energy balance - Regularly monitor blood or milk ketone levels - Improve management during the transition period to reduce stress |
- Optimize nutrition management during the transition period - Regularly monitor ketone levels - Provide high-quality forage and appropriate concentrates |
|
Prognosis |
Good prognosis with timely treatment, but may affect production and reproductive performance |
Good prognosis with early intervention, effectively preventing progression to clinical ketosis |
- Treatment of ketosis
1- Glucose Therapy
- IV 500 mL of 50% dextrose → rapid improvement: Must be combined with longer-term therapy to prevent relapse.
- Bolus IV administration of 500 mL of 50% dextrose solution is a common therapy
2- Glucocorticoids
- Dexamethasone or isoflupredone acetate as it promotes gluconeogenesis and appetite.
- 5–20 mg/dose, IM, may result in a more sustained response, relative to glucose alone.
- Glucose and glucocorticoid therapy may be repeated daily as necessary
3- Propylene Glycol
- Oral drench: 300 mL/day for 3–5 days acts as a glucose precursor.
4- Niacin
Reduces fat mobilization; sometimes used as supportive therapy as it helps conversion of food to energy.
4- insulin therapy
A long-acting insulin preparation given IM at 150–200 IU/day may be beneficial in type 2 ketosis.
5-Treatment of Underlying Disease: Essential in secondary ketosis.
- Prevention Strategies
1-Dietary Management
- Avoid overconditioning during dry period
- Provide high-energy, high-quality ration during early lactation
- Ensure adequate fiber and rumen-effective carbohydrates
- Transition diets 2–3 weeks prepartum
2- Monitoring High-Risk Groups
- Test fresh cows (first 2–21 days in milk)
- Identify cows with high BHBA or NEFA levels
3- Management Practices
- Reduce stress and overcrowding
- Maintain comfortable housing
- Ensure consistent feed availability
4- Feeding Additives
- Monensin (increases propionate production)
- Yeast and rumen modifiers (improve rumen fermentation)
- Economic Impact
Ketosis leads to:
- Reduced milk production (2–7 kg/day loss in SCK)
- Infertility and delayed conception
- Increased risk of displaced abomasum, mastitis, metritis
- Higher culling rates
- References
Ghanem MM and El-Deep WM (2010) lecithin cholesterol acyltransferase (LCAT) activity as a predictor for ketosis and parturient haemoglobinuria in Egyptian water buffaloes. Research in Veterinary Science, 88(1):20-25
Ghanem, M., Fares A.; Abdel-Raof Y. M.; El-Attar H. E. (2017). Clinico-biochemical, oxidative markers and trace elements changes in cows with ketosis. Benha Veterinary Medical Journal, 33(2), 224-236.
Ghanem, M.M., Mahmoud, M.E., Abd El-Raof, Y.M., El-Attar, H.M. (2016). Efficacy of different cow side tests for diagnosis of ketosis in lactating cows. Benha Vet Medical Journal, 31(2): 225-230.
McArt, J. A. A. , Nydam, D. V. , & Oetzel, G. R. (2012). Epidemiology of subclinical ketosis in early lactation dairy cattle. Journal of Dairy Science, 95(9), 5056–5066. 10.3168/jds.2012-5443
McArt, J. A. A. , Nydam, D. V. , & Overton, M. W. (2015). Hyperketonemia in early lactation dairy cattle: A deterministic estimate of component and total cost per case. Journal of Dairy Science, 98, 2043–2054. 10.3168/jds.2014-8740
McArt, J. A. A. , Nydam, D. V. , & Oetzel, G. R. (2013). Dry period and parturient predictors of early lactation hyperketonemia in dairy cattle. Journal of Dairy Science, 96, 198–209.