Small Cell Lung Cancer
| الموقع: | EHC | Egyptian Health Council |
| المقرر الدراسي: | علاج الأورام |
| كتاب: | Small Cell Lung Cancer |
| طبع بواسطة: | Guest user |
| التاريخ: | الخميس، 6 أغسطس 2026، 7:02 AM |
الوصف
"last update: 4 June 2026" Download Guideline
- Executive Summary
This guidance provides a data-supported approach to diagnosis, staging, treatment and follow up of patients diagnosed with SCLC.
|
Recommendation |
Strength of recommendation |
|
Diagnosis and Risk Assessment |
|
|
Initial assessment should include smoking history, physical examination, complete blood count, liver enzymes, sodium, potassium, calcium, glucose, LDH and creatinine (pulmonary function tests if localized disease). |
Good practice statement |
|
Attention drawn towards potential autoimmune-mediated paraneoplastic symptoms is advised . |
Conditional |
|
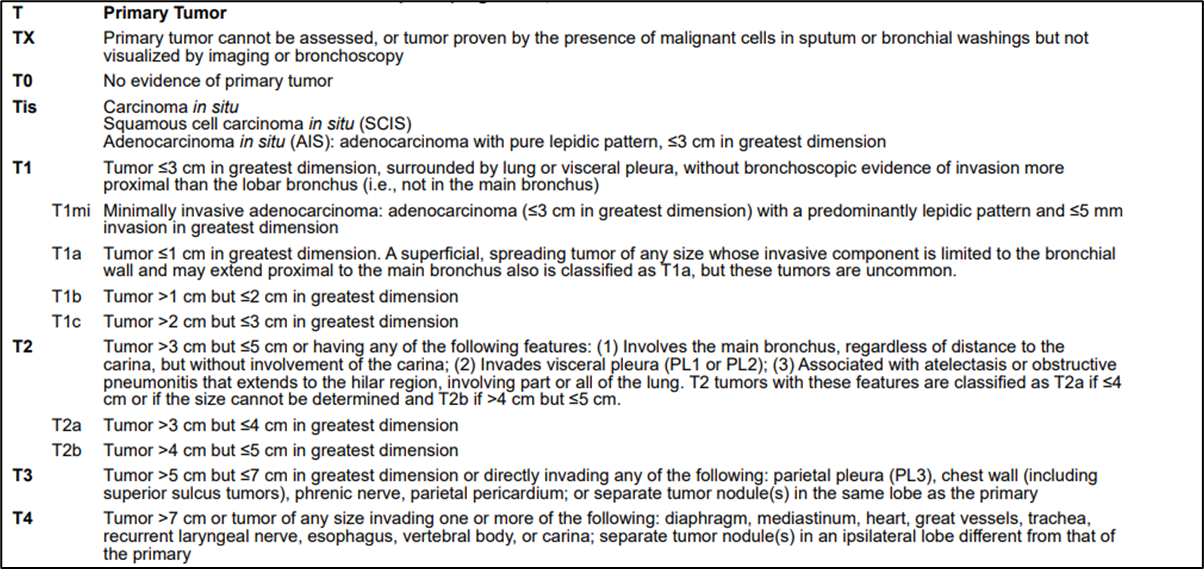
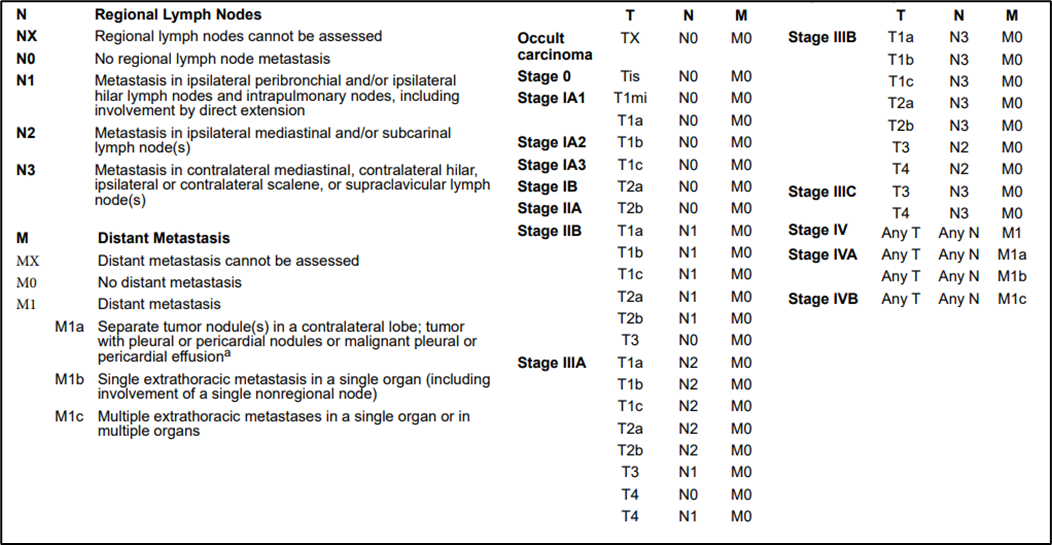
Combined approach of using the AJCC TNM staging system (9th edition) and the older Veterans Administration (VA) Lung Study Group’s 2-stage classification VA scheme for SCLC staging should be used (appendix 1). |
Good practice statement |
|
The effusion should be excluded as a staging element if: 1) multiple cytopathologic examinations of the pleural fluid are negative for cancer; 2) the fluid is not bloody and not an exudate; and 3) clinical judgment concludes that the effusion is not directly related to the cancer. |
Good practice statement |
|
Pericardial effusions are classified using the same criteria mentioned above. |
Good practice statement |
|
A contrast-enhanced CT of the chest and abdomen is recommended. |
Strong |
|
Brain MRI is recommended for all patients. However, contrast enhanced CT is an option when MRI is not available. |
Strong |
|
FDG–PET–CT is optional for staging in limited-stage disease, and FDG–PET findings that modify treatment decisions should be pathologically confirmed. |
Conditional |
|
FDG–PET–CT is advised to assist in RT volume delineation. |
Conditional |
|
In limited-stage disease, additional bone scintigraphy is recommended when no FDG–PET–CT has been carried out. |
Strong |
|
In limited-stage disease, a bone marrow aspiration and biopsy are advised in the case of abnormal blood counts suggesting bone marrow involvement only if it changes clinical management. |
Conditional |
|
The workup for SCLC should not delay the onset of treatment for >1 week because of the aggressive nature of SCLC. |
Good practice statement |
|
Tobacco smoking cessation counseling and intervention should be strongly promoted in patients with SCLC and patients who previously smoked tobacco should be strongly encouraged to remain abstinent. |
Good practice statement |
|
Treatment |
|
|
Management of limited-stage disease (i.e. stages I-III SCLC eligible for treatment of curative intent) |
|
|
Surgery should be considered in patients with clinical stages I and II (cT1-2N0) SCLC in the context of a multimodal treatment concept and following a multidisciplinary board decision. |
Strong |
|
The aim of surgical treatment should be achieving an R0 resection. |
Strong |
|
When considering surgical treatment for SCLC, pathological mediastinal staging should be done. |
Strong |
|
Sublobular resection is not recommended for SCLC. |
Conditional |
|
After surgical resection, in case of pT1-2N0-1, R0 resection, adjuvant chemotherapy should be given. |
Strong |
|
After surgical resection, in case of R1-R2 resection or positive mediastinal lymph nodes (N2), adjuvant chemotherapy should be combined with RT, preferably concurrently. |
Strong |
|
The preferred Chemotherapy for patients with limited-stage (stage I-III) SCLC is platinum plus etoposide. |
Strong |
|
G-CSF is a treatment option to prevent haematological toxicity. |
Good practice statement |
|
Patients with T1-4N0-3M0 tumours and a good PS (0-1) should be treated with concurrent platinum-salt based chemotherapy and thoracic RT. |
Strong |
|
The recommended dose fractionation schedule is 66 Gy. in 33 fractions or equivalent doses |
Strong |
|
Thoracic RT should be initiated as early as possible, starting on the first or second cycle of Chemotherapy. |
Strong |
|
When the patient PS (≥2) or dose to the organs at risk do not allow for the early administration of thoracic RT, it should be postponed until the start of the third cycle of Chemotherapy. |
Strong |
|
Sequential CRT is the preferred option for patients who are not candidates for concurrent CRT due to poor PS, comorbidities and/or disease volume. |
Strong |
|
In case of response to Chemotherapy, the post-Chemotherapy primary tumour should be included in the radiation field. |
Strong |
|
In case of response to Chemotherapy, the pre-Chemotherapy nodal stations should be included in the radiation field. |
Strong |
|
Selective node irradiation is recommended (i.e. involved nodes defined as FDG avid on PET–CT, enlarged on CT and/or biopsy-positive). |
Strong |
|
Patients with stage III SCLC with a response after treatment (CRT) and a PS of 0-1 should be offered PCI. |
Strong |
|
PCI can be considered in patients with a PS of 2. |
Conditional |
|
The role of PCI is not as well defined in patients with stage I-II SCLC or in those >70 years of age or who are frail. In such cases, shared decision making is advised. |
Conditional |
|
The recommended PCI regimen is 25 Gy/10 fractions. |
Strong |
|
Management of extensive-stage disease (i.e. stage IV or stage III SCLC not eligible for treatment of curative intent) |
|
|
The preferred first-line treatment of extensive-stage SCLC (PS 0-2) is four to six cycles of a platinum plus etoposide |
Strong |
|
Cisplatin with irinotecan or topotecan are alternative treatment options. |
Conditional |
|
In poor prognosis patients, gemcitabine plus carboplatin is an alternative treatment option. |
Conditional |
|
In patients achieving a response after Chemotherapy and a PS of 0-2, RT to the residual primary tumour and lymph nodes (30 Gy/10 fractions) is a treatment option. |
Conditional |
|
PCI (20 Gy/5 fractions and 25 Gy/10 fractions) is justified without prior MRI staging or follow-up in patients <75 years of age and a PS of 0-2 who achieved a response after Chemotherapy. |
Strong |
|
In patients with extensive-stage SCLC without brain metastases on brain MRI after Chemotherapy and who can be followed-up with regular brain MRI, PCI may be omitted. |
Strong |
|
Patients with platinum-refractory SCLC have a poor prognosis and BSC is recommended. |
Conditional |
|
Topotecan is recommended for patients with platinum-resistant or -sensitive relapse; CAV , texans, gemcitabine, and oral etoposide are alternative options. |
Strong |
|
In patients with platinum-sensitive SCLC, rechallenge with first-line platinum plus etoposide can be considered. |
Strong |
- Recommendations
Diagnosis and Risk Assessment
● Initial assessment should include smoking history, physical examination, complete blood count, liver enzymes, sodium, potassium, calcium, glucose, LDH and creatinine (pulmonary function tests if localized disease).
Good practice statement
● Attention drawn towards potential autoimmune-mediated paraneoplastic symptoms is advised.
Conditional recommendation, low grade evidence (9)
● Combined approach of using the AJCC TNM staging system (9th edition) and the older Veterans Administration (VA) Lung Study Group’s 2-stage classification VA scheme for SCLC staging should be used (appendix 1).
Good practice statement
● The effusion should be excluded as a staging element if: 1) multiple cytopathologic examinations of the pleural fluid are negative for cancer; 2) the fluid is not bloody and not an exudate; and 3) clinical judgment concludes that the effusion is not directly related to the cancer.
Good practice statement
● Pericardial effusions are classified using the same criteria mentioned in the above recommendation.
Good practice statement
● A contrast-enhanced CT of the chest and abdomen is recommended.
Strong recommendation, very low grade evidence (10)
● Brain MRI is recommended for all patients. However, contrast enhanced CT is an option when MRI is not available.
Strong recommendation, low grade evidence (10)
● FDG–PET–CT is optional for staging in limited-stage disease, and FDG–PET findings that modify treatment decisions should be pathologically confirmed.
Conditional recommendation, moderate grade evidence (11,12)
● FDG–PET–CT is advised to assist in RT volume delineation.
Conditional recommendation, low grade evidence (11,12)
● In limited-stage disease, additional bone scintigraphy is recommended when no FDG–PET–CT has been carried out.
Strong recommendation, very low grade evidence (11,12)
● In limited-stage disease, a bone marrow aspiration and biopsy are advised in the case of abnormal blood counts suggesting bone marrow involvement only if it changes clinical management..
Conditional recommendation, low grade evidence (11)
● The workup for SCLC should not delay the onset of treatment for >1 week because of the aggressive nature of SCLC.
Good practice statement
● Tobacco smoking cessation counseling and intervention should be strongly promoted in patients with SCLC.
Good practice statement
Treatment
● The WHO classification recognizes two types of SCLC: pure and combined SCLC, patients with combined SCLC should treated using regimens for SCLC, because it is the more aggressive cancer.
Strong recommendation, strong grade evidence (13)
· Surgery should be considered in patients with clinical stages I and II (cT1-2N0) SCLC in the context of a multimodal treatment concept and following a multidisciplinary board decision.
Strong recommendation, low grade evidence (14)
· The aim of surgical treatment should be achieving an R0 resection.
Strong recommendation, low grade evidence (15)
· When considering surgical treatment for SCLC, pathological mediastinal staging should be done.
Strong recommendation, very low grade evidence (16,17)
· Sublobular resection is not recommended for SCLC.
Conditional recommendation, low grade evidence (15)
· After surgical resection, in case of pT1-2N0-1, R0 resection, adjuvant chemotherapy should be given.
Strong recommendation, very low grade evidence (18)
· After surgical resection, in case of R1-R2 resection or positive mediastinal lymph nodes (N2), adjuvant chemotherapy should be combined with RT, preferably concurrently.
Strong recommendation, very low grade evidence (16)
· The preferred Chemotherapy for patients with limited-stage (stage I-III) SCLC is cisplatin plus etoposide.
Strong recommendation, high grade evidence (19)
· When cisplatin is contraindicated because of comorbidities, carboplatin plus etoposide is recommended.
Strong recommendation, high grade evidence (20)
· G-CSF is a treatment option to prevent haematological toxicity.
Good practice statement
· Patients with T1-4N0-3M0 tumours and a good PS (0-1) should be treated with concurrent platinum-salt based chemotherapy and thoracic RT.
Strong recommendation, high grade evidence (21,22)
· The recommended fractionation schedule is 66 Gy in 33 fractions or equivalent doses.
Strong recommendation, high grade evidence (21)
· Thoracic RT should be initiated as early as possible, starting on the first or second cycle of Chemotherapy.
Strong recommendation, high grade evidence (23)
· When the patient PS (≥2) or dose to the organs at risk do not allow for the early administration of thoracic RT, it should be postponed until the start of the third cycle of Chemotherapy.
Strong recommendation, high grade evidence (24,25)
· Sequential CRT is a preferred option for patients who are not candidates for concurrent CRT due to poor PS, comorbidities and/or disease volume.
Strong recommendation, low grade evidence (26)
· In case of response to Chemotherapy, the post-Chemotherapy primary tumour should be included in the radiation field.
Strong recommendation, low grade evidence (26)
· In case of response to Chemotherapy, the pre-Chemotherapy nodal stations should be included in the radiation field.
Strong recommendation, low grade evidence (26)
· In case of stable disease, surveillance is recommended until progression.
Good practice statement
· In case of disease progression treatment of extensive disease is recommended
Good practice statement
· Selective node irradiation is recommended (i.e. involved nodes defined as FDG avid on PET–CT, enlarged on CT and/or biopsy-positive).
Strong recommendation, high grade evidence (24)
· Patients with stage III SCLC with a response after treatment (CRT) and a PS of 0-1 should be offered PCI.
Strong recommendation, low grade evidence (27)
· PCI can be considered in patients with a PS of 2.
Conditional recommendation, low grade evidence (27)
· The role of PCI is not as well defined in patients with stage I-II SCLC or in those >70 years of age or who are frail. In such cases, shared decision making is advised.
Conditional recommendation, very low grade evidence (28)
· The recommended PCI regimen is 25 Gy/10 fractions.
Strong recommendation, high grade evidence (29)
Management of extensive-stage disease (i.e. stage IV or stage III SCLC not eligible for treatment of curative intent)
· The preferred first-line treatment of extensive-stage SCLC (PS 0-2) is four to six cycles of a platinum plus etoposide.
Strong recommendation, high grade evidence (19)
· Cisplatin with irinotecan or topotecan are alternative treatment options.
Conditional recommendation, moderate grade evidence (30,31)
· In poor prognosis patients, gemcitabine plus carboplatin is an alternative treatment option.
Conditional recommendation, moderate grade evidence (32)
· In patients achieving a response after Chemotherapy and a PS of 0-2, RT to the residual primary tumour and lymph nodes (30 Gy/10 fractions) is a treatment option.
Conditional recommendation, moderate grade evidence (33)
· PCI (20 Gy/5 fractions and 25 Gy/10 fractions) is justified without prior MRI staging or follow-up in patients <75 years of age and a PS of 0-2 who achieved a response after Chemotherapy.
Strong recommendation, high grade evidence (34)
· In patients with extensive-stage SCLC without brain metastases on brain MRI after Chemotherapy and who can be followed-up with regular brain MRI, PCI may be omitted.
Conditional recommendation, high grade evidence (35)
· Patients with platinum-refractory SCLC have a poor prognosis and BSC is recommended.
Strong recommendation, moderate grade evidence (36)
· Topotecan is recommended for patients with platinum-resistant or -sensitive relapse; CAV , Texans, Gemcitabine, oral etoposide are alternative options.
Strong recommendation, moderate grade evidence (37)
· In patients with platinum-sensitive SCLC, rechallenge with first-line platinum plus etoposide can be considered.
Strong recommendation, high grade evidence (38)
- Acknowledgments
· We would like to acknowledge the Oncology Committee of the Egyptian Health Council (EHC) Guidelines, for adapting these Guidelines.
· Chair of the Oncology Committee of Egyptian Health Council Guidelines: Prof Hussein Khaled.
· The Oncology Committee Members: Emad Hamada, Samir Shehata, Hesham Elghazaly, Hesham Tawfik, Fouad Abuotaleb, Ebtesam Saad Eldin, Ehab Khalil, Khaled Abdelkarim, Lobna EZZ Elarab, Mary Gamal, Mohamed Abdel Mooti, Mohamed Gamil, Nervana Hussein, Ola Khorshid, Omar Sherif Omar, Rasha Fahmi, Rasha Shaltout, Yousri Wasef & Yousri Rostom.
- Abbreviations
|
AJCC |
American joint commission on cancer |
|
BSC |
Best supportive care |
|
CBC |
Complete blood count |
|
CCRT |
Concomitant radio-chemo-therapy |
|
CT |
Computed Tomography |
|
EHC |
Egyptian Health Council |
|
G-CSF |
Granulocyte colony stimulating factor |
|
IHC |
Immunohistochemistry |
|
KFTs |
Kidney function tests |
|
LFTs |
Liver function tests |
|
MRI |
Magnetic resonance imaging |
|
OS |
Overall Survival |
|
PCI |
Prophylactic cranial irradiation |
|
PET/CT |
Positron emission tomography/Computed Tomography |
|
PS |
Performance Status |
|
SCLC |
Small-cell lung cancer |
|
ULN |
Upper limit of normal |
- Introduction
Small-cell lung cancer (SCLC) is the most aggressive form of lung cancer. Although SCLC is characterized by rapid responses to chemotherapy and sensitivity to radiotherapy, due to early treatment resistance, the 5-year overall survival (OS) is <10%. The incidence of SCLC has
decreased in recent decades, and with a prevalence of 1-5 per 10 000 people in the European community (1-4). In Egypt, there was an estimated 375 new cases of SCLC and 335 deaths
occurred because of this disease based on GLOBOCAN 2022. (5)
- Purpose and scope
These guidelines are developed to improve the quality of care for SCLC cancer via providing a uniform standard of care across the country to help in early diagnosis, treatment and follow up for SCL cancer so more optimal treatment options and improved clinical outcomes.
- Target audience
Clinicians who are involved in the care and treatment of patients with SCLC, include medical oncologists, radiation oncologists, clinical oncologist, surgeons, clinical dietitian , intervention radiologists, radiologists, pathologists, and palliative care specialists.
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/exclusion criteria followed in the search and retrieval of guidelines to be adapted:
- Selecting only evidence-based guidelines (guidelines must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence). - Selecting only national and/or international guidelines.
- Specific range of dates for publication (using Guidelines published or updated 2020 and later).
- Selecting peer reviewed publications only.
- Selecting guidelines written in English language.
- Excluding guidelines written by a single author not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input.
- Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations.
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least two members. the panel decided a cutoff point or rank the guidelines (any guideline scoring above 50% on the rigor dimension was retained)
The NCCN, ESMO, NICE guidelines are the main sources used while formulating the national guidelines for SCLC (6-8).
- Evidence assessment
According to WHO handbook for Guidelines we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed information on GRADE is available through the on the following sites:
• GRADE working group: https://www.gradeworkinggroup.org/
• GRADE online training modules: http://cebgrade.mcmaster.ca/
Table 1: Quality of evidence in GRADE
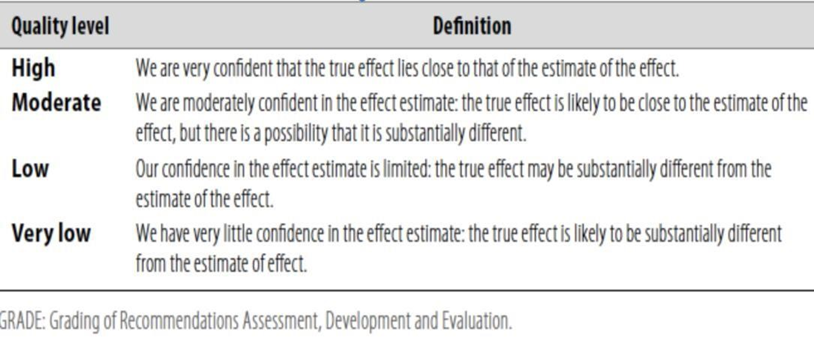
Table 2: Significance of the four levels of evidence
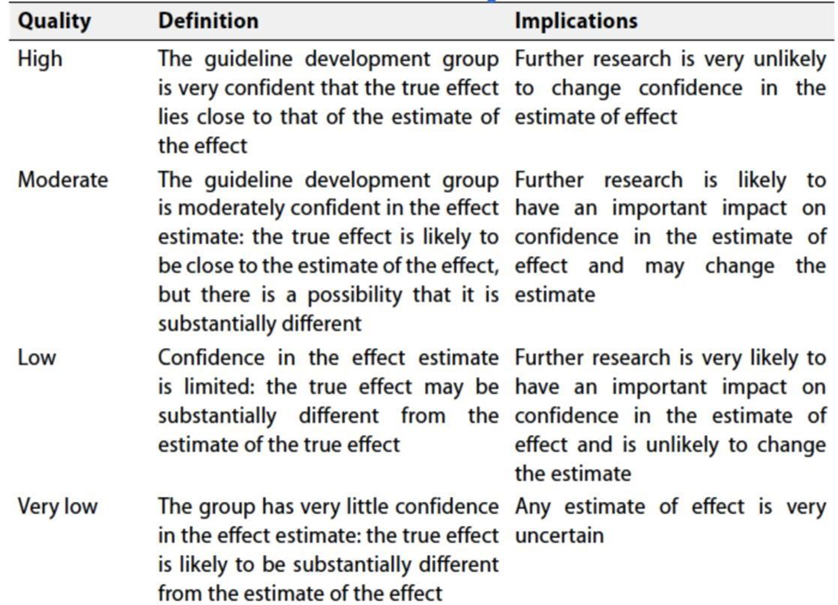
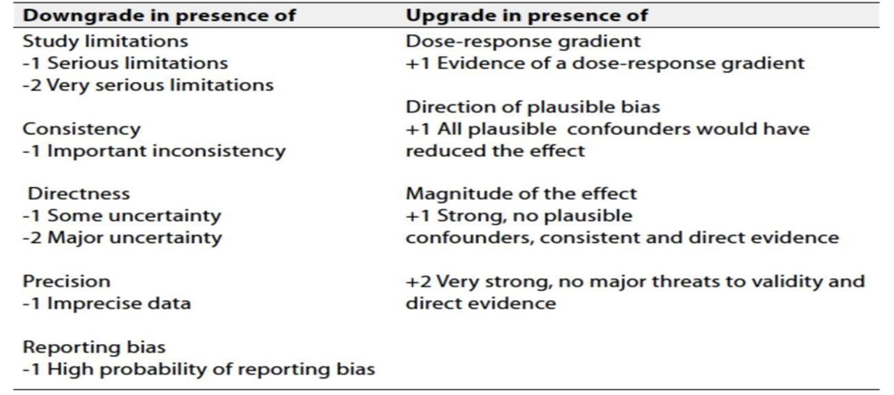
Table 3: Factors that determine How to upgrade or downgrade the quality of evidence
➢ The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation:
Strong recommendations: With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations: These are made when there is greater uncertainty about the four factors above (Table 2) or if local adaptation must account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations; when there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
- Clinical indicators for monitoring
For patients newly diagnosed with SCL cancer:
▪ laboratory evaluation (CBC, LFT, and KFT)
▪ imaging
▪ tissue biopsy for pathological confirmation and IHC
- Research gaps
▪ Address the leading cause of lung cancer, such as smoking.
▪ Systematically incorporate cost-benefit analyses into clinical trials, including health economic measures such as the incremental cost-effectiveness ratio, to support clinical decision-making (e.g., ultra-low-dose immunotherapy).
▪ Identify predictive biomarkers for response to specific targeted therapies and immunotherapy.
▪ Improve preclinical models for testing novel drugs.
▪ Identify tools for assessing quality of life in clinical trials.
- Update of this guideline
▪ This guideline will be updated whenever there is new evidence.
- References
1.American Cancer Society. Cancer Facts & Figures 2019. Atlanta: American Cancer Society. 2019. Available at: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2019/cancer-facts-and-figures-2019.pdf.
2. Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database.J Clin Oncol. 2006;24(28):4539-4544.
3. Breitling LP, Rinke A, Gress TM. Recent survival trends in high-grade neuroendocrine neoplasms and lung cancer. Neuroendocrinology. 2020;110(3-4):225-233.
4. Abdel-Rahman O. Changing epidemiology of elderly small cell lung cancer patients over the last 40 years; a SEER database analysis. Clin Respir J. 2018;12(3):1093-1099.
5.Globocan: https://gco.iarc.who.int/media/globocan/factsheets/populations/818-egypt-fact-
sheet.pdf
6.ESMO:https://www.esmo.org/guidelines/esmo-clinical-practice-guidelines-lung-and-chest-
tumours
7.NCCN: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1462
8.NICE : https://www.nice.org.uk/what-nice-does/our-guidance/about-nice-guidelines
9.Gozzard P, Woodhall M, Chapman C, et al. Paraneoplastic neurologic disorders in small
cell lung carcinoma: a prospective study. Neurology 2015;85(3):235-239.
10.Seute T, Leffers P, ten Velde GP, et al. Detection of brain metastases from small cell lung
cancer: consequences of changing imaging techniques (CT versus MRI). Cancer. 2008;112(8):1827-1834.
11.Martucci F, Pascale M, Valli MC, et al. Impact of (18)F-FDG PET/CT in staging patients
with small cell lung cancer: a systematic review and meta-analysis. Front Med (Lausanne). 2019;6:336.
12.Manoharan P, Salem A, Mistry H, et al. (18)F-Fludeoxyglucose PET/CT in SCLC:
analysis of the CONVERT randomized controlled trial. J Thorac Oncol. 2019;14(7):1296-1305.
13.Qin J, Lu H. Combined small-cell lung carcinoma. Onco Targets Ther
2018;11:3505–3511.
14.Zhao X, Kallakury B, Chahine JJ, et al. Surgical resection of SCLC: prognostic factors
and the tumor microenvironment. J Thorac Oncol. 2019;14(5):914-923.
15.Rami-Porta R, Wittekind C, Goldstraw P. Complete resection in lung cancer surgery:
proposed definition. Lung Cancer. 2005;49(1):25-33.
16.Ernani V, Ganti AK. Surgery for limited-stage small cell lung cancer: ready for prime-
time? J Thorac Dis. 2017;9(10):3576-3578.
17.Stinchcombe TE. Current treatments for surgically resectable, limitedstage,
and extensive-stage small cell lung cancer. Oncologist. 2017;22(12):1510-1517.
18.Yang CF, Chan DY, Speicher PJ, et al. Role of adjuvant therapy in a population-
based cohort of patients with early-stage small-cell lung cancer. J Clin Oncol. 2016;34(10):1057-1064.
19.Mascaux C, Paesmans M, Berghmans T, et al. A systematic review of the role of
etoposide and cisplatin in the chemotherapy of small cell lung cancer with methodology assessment and meta-analysis. Lung Cancer. 2000;30(1):23-36.
20.Karam I, Jiang SY, Khaira M, et al. Outcomes of small cell lung cancer patients treatedwith cisplatin-etoposide versus carboplatin-etoposide. Am J Clin Oncol. 2015;38(1):51-54.
21. Faivre-Finn C, Snee M, Ashcroft L, et al. Concurrent once-daily versus twice-daily chemo radiotherapy in patients with limited-stage small cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial. Lancet Oncol. 2017;18(8):1116-1125.
22. Gomes F, Faivre-Finn C, Mistry H, et al. Safety of G-CSF with concurrent
chemo-radiotherapy in limited-stage small cell lung cancerdsecondary
analysis of the randomised phase 3 CONVERT trial. Lung
Cancer. 2021;153:165-170.
23. Turrisi AT 3rd, Kim K, Blum R, et al. Twice-daily compared with once daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med. 1999;340(4): 265-271.
24.De Ruysscher D, Lueza B, Le Péchoux C, et al. Impact of thoracic radiotherapy timing in
limited-stage small-cell lung cancer: usefulness of the individual patient data meta-analysis. Ann Oncol. 2016;27(10): 1818-1828.
25.Lu H, Fang L, Wang X, et al. A meta-analysis of randomized controlled trials
comparing early and late concurrent thoracic radiotherapy with etoposide and cisplatin/carboplatin chemotherapy for limited-disease small-cell lung cancer. Mol Clin Oncol. 2014;2(5):805-810.
26. Kies MS, Mira JG, Crowley JJ, et al. Multimodal therapy for limited small-cell lung cancer: a randomized study of induction combination chemotherapy with or without thoracic radiation in complete responders; and with wide-field versus reduced-field radiation in partial responders: a Southwest Oncology Group Study. J Clin Oncol. 1987;5(4):592-600.
27.Le Péchoux C, Dunant A, Senan S, et al. Standard-dose versus higherdose
prophylactic cranial irradiation (PCI) in patients with limitedstage small-cell lung cancer in complete remission after chemotherapy and thoracic radiotherapy (PCI 99-01, EORTC 22003-08004, RTOG 0212, and IFCT 99-01): a randomised clinical trial. Lancet Oncol.2009;10(5):467-474.
28.Aupérin A, Arriagada R, Pignon JP, et al. Prophylactic cranial irradiation
for patients with small-cell lung cancer in complete remission.
Prophylactic Cranial Irradiation Overview Collaborative Group. N Engl
J Med. 1999;341(7):476-484.
29.Takahashi T, Yamanaka T, Seto T, et al. Prophylactic cranial irradiation versus observation in patients with extensive-disease small-cell lung cancer: a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18(5):663-671.
30.Liu ZL, Wang B, Liu JZ, et al. Irinotecan plus cisplatin compared with etoposide plus cisplatin in patients with previously untreated extensive-stage small cell lung cancer: a meta-analysis. J Cancer Res Ther. 2018;14(Supplement):S1076-S1083.
31. Eckardt JR, von Pawel J, Papai Z, et al. Open-label, multicenter, randomized,
phase III study comparing oral topotecan/cisplatin versus etoposide/cisplatin as treatment for chemotherapy-naive patients with extensive-disease small-cell lung cancer. J Clin Oncol. 2006;24(13):2044-2051.
32.Lee SM, James LE, Qian W, et al. Comparison of gemcitabine and carboplatin versus cisplatin and etoposide for patients with poorprognosis small cell lung cancer. Thorax. 2009;64(1):75-80.
33.Slotman BJ, van Tinteren H, Praag JO, et al. Radiotherapy for extensive
stage small-cell lung cancerdauthors’ reply. Lancet. 2015;385(9975):1292-1293.
34.Slotman B, Faivre-Finn C, Kramer G, et al. Prophylactic cranial irradiation
in extensive small-cell lung cancer. N Engl J Med. 2007;357(7): 664-672.
35.Jeremic B, Shibamoto Y, Nikolic N, et al. Role of radiation therapy in the combined-modality treatment of patients with extensive disease small-cell lung cancer: a randomized study. J Clin Oncol. 1999;17(7):2092-2099.
36.Owonikoko TK, Behera M, Chen Z, et al. A systematic analysis of efficacy
of second-line chemotherapy in sensitive and refractory smallcell lung cancer. J Thorac Oncol. 2012;7(5):866-872.
37.von Pawel J, Schiller JH, Shepherd FA, et al. Topotecan versus cyclophosphamide,
doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol. 1999;17(2):658-667.
38.Postmus PE, Berendsen HH, van Zandwijk N, et al. Retreatment with the induction regimen in small cell lung cancer relapsing after an initial response to short term chemotherapy. Eur J Cancer Clin Oncol. 1987;23(9):1409-1411.
- Annexes
1-TNM Classification
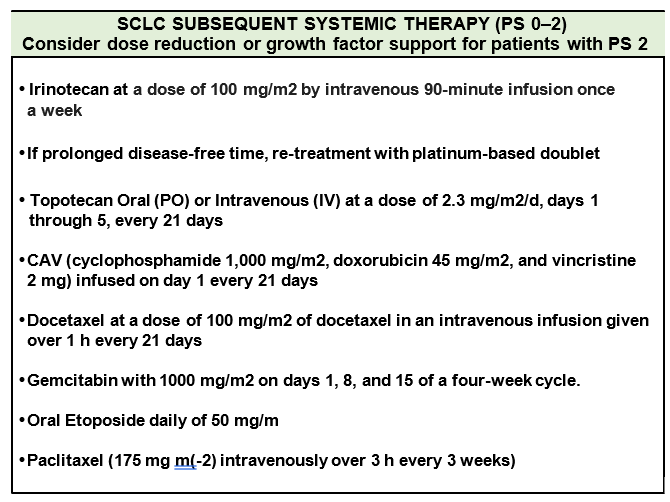
2-Systemic Therapy Doses
|
PRIMARY OR ADJUVANT THERAPY FOR LIMITED STAGE SCLC |
|
Four cycles of cytotoxic chemotherapy are recommended.
Planned cycle length should be every 21–28 days during concurrent RT.
During cytotoxic chemotherapy + RT, Cisplatin/Etoposide is recommended.
The use of myeloid growth factors is not recommended during concurrent cytotoxic chemotherapy plus RT |
|
● Cisplatin 75 mg/m, Day 1 and Etoposide 100 mg/m Days 1, 2, 3
• Cisplatin 60 mg/m2 Day 1 and Etoposide 120 mg/m Days 1, 2, 3
• Carboplatin area under the curve (AUC) 5–6 Day 1 and Etoposide 100 mg/m Days 1, 2, 3
• Cisplatin 25 mg/m2 Days 1, 2, 3 and Etoposide 100 mg/m Days 1, 2, 3
|
|
PRIMARY THERAPY FOR EXTENSIVE STAGE SCLC |
|
Four cycles of cytotoxic chemotherapy are recommended,
but some patients may receive up to 6 cycles based on response and tolerability after 4 cycles. |
|
Carboplatin AUC 5–6 Day 1 and Etoposide 80–100 mg/m2 Days 1, 2, 3
Cisplatin 75–80 mg/m Day 1 and Etoposide 80–100 mg/m2 Days 1, 2, 3
Carboplatin AUC 5 Day 1 and Irinotecan 50 mg/m2 Days 1, 8, 15
Cisplatin 60 mg/m2 Day 1 and Irinotecan 60 mg/m2 Days 1, 8, 15
Cisplatin 30 mg/m2 Days 1, 8 and Irinotecan 65 mg/m2 Days 1, 8 |