LACRIMAL SYSTEM
| Site: | EHC | Egyptian Health Council |
| Course: | Veterinary Ophthalmology Guidelines |
| Book: | LACRIMAL SYSTEM |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 16 June 2026" Download Guideline
Table of contents
- - Acknowledgement
- - ANATOMY AND PHYSIOLOGY
- - The distributional system
- - The excretory system
- - EXAMINATION OF LACRIMAL SYSTEM
- - AFFECTION OF THE LACRIMAL SYSTEM
- - Epiphora
- - Congenital Atresia, Ectopia, and Imperforate Puncta
- - Dacryocystitis
- - Obstruction of the canaliculi
- - Obstruction of the nasolacrimal duct
- - Atresia of nasal punctum
- - Lacrimal sac histoplasmosis
- - Keratoconjunctivitis sicca (KCS - Dry eye - Xerophthalmia)
- - References
- Acknowledgement
We would like to acknowledge the committee of National Egyptian Guidelines for Veterinary Medical Interventions, Egyptian Health Council for adapting this guideline.
Executive Chief of the Egyptian Health Council: Prof. Dr Mohamed Mustafa Lotief.
Head of the Committee: Prof. Dr Ahmed M Byomi
The rapporteur of the Committee: Prof. Dr Mohamed Mohamedy Ghanem.
Scientific Group Members: Prof. Dr Nabil Yassien, Prof. Dr Ashraf Aly Eldesoky Shamaa, Prof. Dr Amany Abbas, Prof. Dr Dalia Mansour, Dr Essam Sobhy Dr Mohamed Elsharkawy, Prof. Dr Gamal A. Sosa., Dr Naglaa Radwan, Dr Hend El Sheikh
Scientific Editor/Authors: Prof. Dr Ashraf Aly Eldesoky Shamaa. Dr Mohamed Elsharkawy. Prof. Dr. Mohamed Mostafa Saied Amer, Prof. Dr. Shaaban Mohamed and Dr. Mohamed Moustafa Bahr Moustafa.
- ANATOMY AND PHYSIOLOGY
The lacrimal apparatus consists of a 3 systems:
I- Secretory system.
II- Distributional system.
III- Excretory system.
I. The secretory system ( lacrimal glands ) These glands are:
a- lacrimal glands
1- The gland of the third eyelid
Which lies within the stroma of the third eyelid, is partially visible on the inner surface of the third eyelid.
2- The tubuloalveolar lacrimal gland
is flattened and lies over the superior temporal part of the globe. The position is similar in species with a fully enclosed bony orbit. Lacrimal secretions enter the superior conjunctival fornix from the canine lacrimal gland via three to five microscopic ducts, and from the gland of the third eyelid via multiple ducts opening on the bulbar surface of the third eyelid between the normal lymphoid follicles. The precorneal tear film is distributed over the ocular surface by gravity, blinking, and movement of the third eyelid.
3-Accessory lacrimal glands Which are near the lid margins and contribute to the precorneal tear film, are composed of the following
The meibomian (tarsal) glands. They produce the superficial layer of the precorneal tear film.
The glands of Moll (modified sweat glands).
The glands of Zeis (modified sebaceous glands associated with the cilia)
The functional significance of the glands of Moll and Zeis in animals is unknown, although infections of the glands of Zeis occur clinically and are called external hordeolum (stye).
- The distributional system
Precorneal tear film is consists of 3 layers
a) Outer oily layer
b) Middle aqueous layer
c) Inner mucoid layer
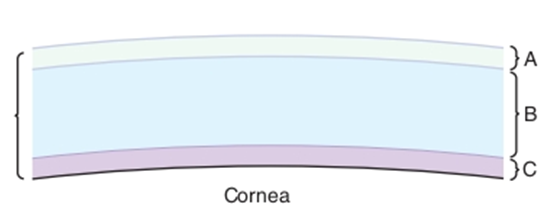
Fig.1: Precorneal tear film. A, Superficial lipid layer; B, aqueous layer; C, inner mucoid layer (David et al.,2008).
Functions of The precorneal tear film
1- Provide antibacterial activity (lysozyme and leucocytes).
2- Maintain the optical activity of the cornea. The film has a refractive index comparable to the cornea.
3- Provide metabolic needs; oxygen and other metabolites are absorbed by the epithelium from the tear film.
4- Remove waste products and debris.
5- Provide lubrication for the eyelids.
6- Mucous thread (Fine mucous threads lie in the superior and inferior conjunctival fornices in the normal animal).
Effects of Precorneal Tear Film Dysfunction
1- Hypertonicity of the remaining tear film.
2- Dehydration of the conjunctival and corneal epithelium.
3- Hypoxia of the corneal epithelium and subepithelial stroma.
4- lack of lubrication with frictional irritation of the ocular surface by the eyelids and third eyelid.
5- Increase in numbers of microorganisms and mucus on the ocular surface and on the eyelids.
6- Secondary inflammation of the conjunctiva and cornea with stromal vascularization and later pigmentation.
7- Corneal erosions or ulcers.
- The excretory system
Excretory system consists of
a) Lacrimal puncta
In most domestic mammals the inferior and superior puncta lie on the inner conjunctival surface of the eyelids, near the nasal limit of the tarsal glands.
b) Lacrimal Canaliculi.
The lacrimal canaliculi (superior and inferior) lead to a variable dilation in the common nasolacrimal duct.
c) Lacrimal sac
The lacrimal sac varies in size, in some animals consisting only of a slight dilation in the duct. The sac lies within a depression in the lacrimal bone called the lacrimal fossa.
d) Nasolacrimal duct
the nasolacrimal duct passes via a canal on the medial surface of the maxilla to open in the nasal
cavity.
e) Nasal puncta.
In dogs the opening is ventrolateral near the attached margin of the alar fold; in horses it is ventral on the mucocutaneous junction; and in cattle it is more lateral. In cattle and horses the nasal opening is readily visible and can be cannulated, but in dogs it can be seen only after exposure with a speculum or other suitable instrument with the animals under general anesthesia.
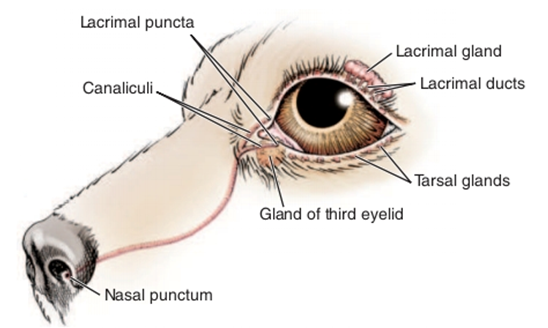
Fig.2: Components of the nasolacrimal system (David et al.,2008).
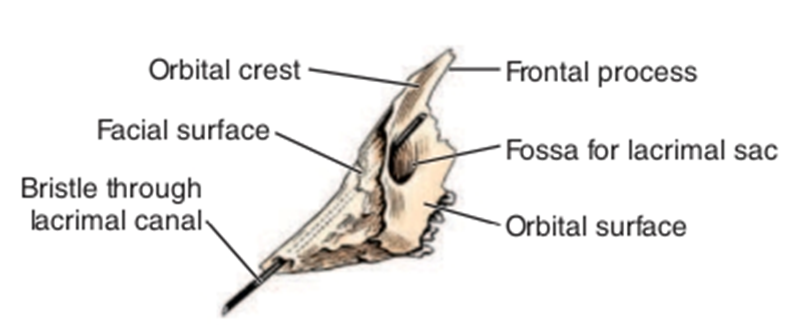
Fig.3: Left canine lacrimal bone, lateral aspect, showing the lacrimal fossa. (Evans, 1993).
- EXAMINATION OF LACRIMAL SYSTEM
I- Schirmer’s tear test (STT)
1- Quantitative abnormalities.
2- If epiphora is due to overproduction of tears, the eye is usually red and the STT values are higher than normal.
II- Nasolacrimal duct cannulation (Fluorescein passage test - Rose Bengal stain).
1- Rose bengal stain to detect epithelial abnormalities caused by quantitative and qualitative disorders.
2- Fluorescein passage or Jones test for drainage disorders and corneal ulceration is reliable only when its result is positive. Because of communications between the nasolacrimal duct and the nasal cavity, false-negative results occur even though the duct is patent.

Fig.4: Nasolacrimal duct cannulation in donkey.
- AFFECTION OF THE LACRIMAL SYSTEM
DISTURBANCES OF LACRIMAL FUNCTION
The two categories of lacrimal dysfunction are:
1- Inability of the drainage system to remove the tears produced.
This is caused either by:
a- Obstruction of the drainage system or overproduction of tears.
b- The clinical signs depend on the relative amounts of tears produced and drained away.
2- Failure to produce a normal precorneal tear film (or one of its components), usually resulting in secondary conjunctivitis and keratitis. Abnormalities are quantitative (insufficient aqueous component) or qualitative (abnormalities in components or function of the superficial lipid layer, or the inner mucoid layer).
- Epiphora
It means abnormal flow of tears outside the eye. By means of the “zip-closure action” of the blinking of the eyelids, tear fluid is moved towards the medial canthus. If any functional obstruction to its
drainage or simply excessive production, tears flows over the edge of the eyelid and a brown tear stripe will form under the medial canthus.
Causes:
1- Medial lower entropion.
2- Prominence of the globe (exophthalmia) with shallow lacrimal lake.
3- Obstruction of the lower punctum.
4- Congenital absence of the lower punctum or canaliculus.
5- Nasolacrimal duct obstruction.
6- Localized inflammation along the course of the duct.
7- Excessive tear production secondary to irritation caused by entropion, ectropion, distichiasis, trichiasis and ectopic cilia.
Symptoms:
Flow of tears outside the eye with tear stains the medial canthal skin and hair. Flow of tears for a long time usually leads to formation of tear scald in donkeys.
Treatment:
Try to correct the primary cause after thorough examination of the eyeball and its adnexal structures.
- Congenital Atresia, Ectopia, and Imperforate Puncta
- The condition is congenital and is often characterized by epiphora, although some animals are relatively asymptomatic and epiphora may not become apparent until several weeks of age, when tear production increases.
- In dogs, imperforate puncta (usually of the inferior puncta) and punctal aplasia are common.
Diagnosis
By examination of the normal location of the puncta with magnification and from the inability to cannulate or probe the puncta with a small polytetrafluoroethylene (Teflon) IV catheter (minus needle),a lacrimal cannula, or fine nylon thread.
Treatment:
1. Surgical opening of the affected punctum is performed. A lacrimal cannula is inserted into the patent punctum or at the nasal punctum and flushing is performed under pressure.
Antibiotic-corticosteroid preparations are applied for 7 to 10 days to prevent scarring and obstruction. Daily dilation and flushing may be needed for a few days to prevent closure. If the membrane is thick or bleeds when incised the nasolacrimal system may need to be cannulated for 1 to 3 weeks to prevent fibrosis of the newly created stoma.
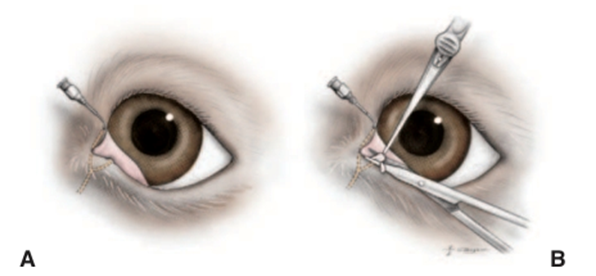
Fig.5: Repair of imperforate punctum by pressurized fluid. A, The opposing punctum is cannulated, and pressure is applied via a saline-filled syringe to elevate the obstructing conjunctiva over the other punctum . B, The tissue is grasped with fine forceps and incised with strabismus scissors or other fine scissors (David et al.,2008).
2- The overlying conjunctiva may be removed through retrograde probing with fine nylon thread (2/0) from the nasal opening. . This procedure ismost useful for the superior punctum, because it is more difficult to pass a probe into the inferior punctum from the nasal end.
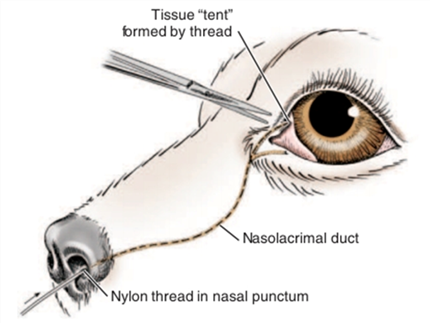
Fig.6: Retrograde probing of imperforate punctum. The nasal meatus of the nasolacrimal duct is probed using a nylon (2/0) thread. The probe is passed up to elevate the obstructing conjunctiva, which is excised (David et al.,2008).
- Dacryocystitis
It means inflammation of the lacrimal sac, canaliculi and nasolacrimal duct. Dacryocystitis usually is a concurrent with or sequelae to conjunctivitis.

Fig.7 : Dacryocystitis and secondary conjunctivitis in a horse. The conjunctivitis results from the failure of tear drainage as well as the reflux of tears from the obstructed and inflamed nasolacrimal sac.
Causes:
Viral, bacterial and mycotic infections are the most common causes. Cystic dilations of the nasolacrimal duct causing chronic dacryocystitis in dogs have been described
Symptoms:
1- Thick mucoid or mucopurulent discharge is present at the medial canthus.
2- Mucopurulent conjunctivitis is usually present.
3- Small swelling at the medial canthus is evident and painful to palpation. Digital pressure over this swelling may extrude a mucopurulent exudate.
4- In acute dacryocystitis, abscess may form and opens subcutaneously at the medial canthus. Fistula may develop connecting the sac with external skin.
5- Painful, erythematous dermatitis at the medial canthus in some cases.
6- History of recurrent unilateral conjunctivitis with temporary responses to topical antibiotics and attempted flushing.
DIAGNOSIS.
based on clinical signs, especially expression of purulent material from the puncta. The exact
site of the obstruction may be determined by cannulation, dacryocystorhinography, or magnetic resonance imaging.
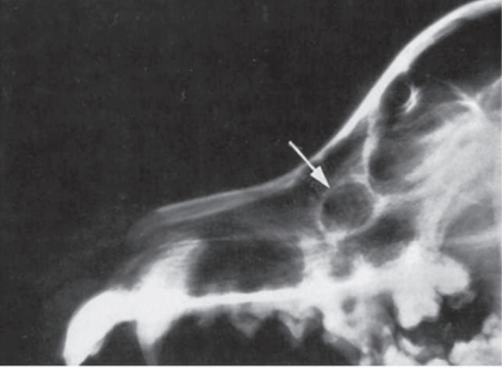
Fig.8: Lateral radiographic view of the skull of a 4-year-old golden retriever with recurrent intermittent episodes of purulent discharge from the right eye. A radiolucent area with sclerotic margins (arrow) is evident dorsal and rostral to the maxillary process of the maxillary bone (dorsal to the upper right fourth premolar). (Woerdt et al., 1997)
Treatment:
A- Medical treatment
By flushing and topical medication are effective in some cases, they are less reliable than catheterization and there is a greater chance of recurrence.
B- Surgical treatment
1- Catheterization and placement of retention tube which is left in place for 2 to 3 weeks. The inserted tubes rarely cause discomfort unless they become loose. For the first few days the uncannulated punctum may be flushed daily with a topical ophthalmic antibiotic solution, and topical antibiotic/corticosteroid solution is also applied to the ocular surface. If abscessation of the sac or severe dermatitis is present, systemic antibiotics are added.
2- Dacryocystotomy when the obstruction prevents the passage of a catheter.
|
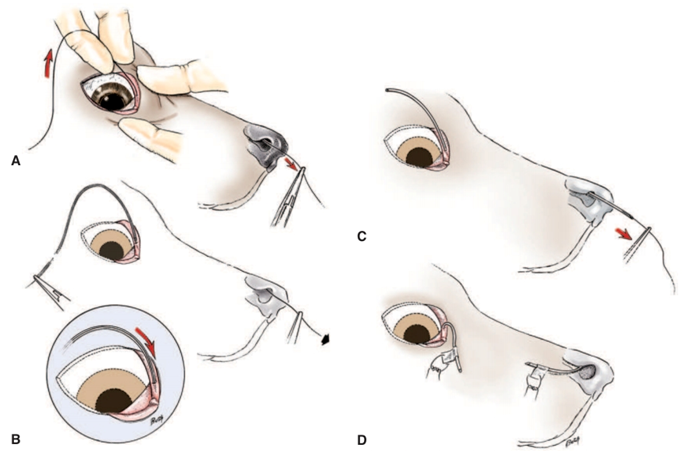
Fig.9: Indwelling nasolacrimal duct catheterization for correction of recurring obstruction: A, A monofilament nylon thread (2/0 with a smooth melted end) is passed via the superior punctum to emerge from the nose . B, Fine polyethylene (PE90), polyvinyl, or silicone tubing with a beveled end is passed over the thread. Halsted forceps are clamped behind the tubing, which is pulled from the nasal end by forceps on the thread. In horses, larger tubing is used. C, Care is taken as the tubing enters the punctum. Note: The inferior punctum may also be used if threading via this punctum was used. The tubing is pulled down the nasolacrimal duct, past any obstructions. D, The tube is sutured in place for 2 to 3 weeks. An Elizabethan collar should be considered to prevent the tubing from being dislodged. (Bistner et al.,1977) . |
- Obstruction of the canaliculi
Treatment:
Conjunctivoralostomy or conjunctivorhinostomy is the operation of choice in cases of absence of the lower canaliculus.
- Obstruction of the nasolacrimal duct
In cats blockage of the puncta or nasolacrimal ducts are common sequela of presumed herpetic
keratoconjunctivitis and upper respiratory tract infections. Similar may be seen in any species and frequently accompanies symblepharon.

Fig.10: Duct obstruction in a horse. Note the mucoid discharge at the medial canthus.
Symptoms:
1- Epiphora.
2- moisture and tear staining of the medial canthal skin and sometimes serous or seromucoid conjunctivitis.
Treatment:
In congenital atresia of a segment of the duct, Conjunctivorhinostomy or Conjunctivobuccostomy is the treatment of choice. In cases of acquired obstruction flushing of the duct is performed 2-3 times daily for several days with ophthalmic solutions containing antibiotics and corticosteroids.
|
Fig.11:Conjunctivorhinostomy. A, The conjunctiva is removed from the inferior nasal area overlying the lacrimal bone. B, A communication is made from the conjunctival sac to the nasal cavity with a Steinmann orthopaedic pin. The pin is directed toward the contralateral external nares but is advanced only until it enters the nasal cavity. A stent of plastic tubing is sutured in place (David et al.,2008).
|
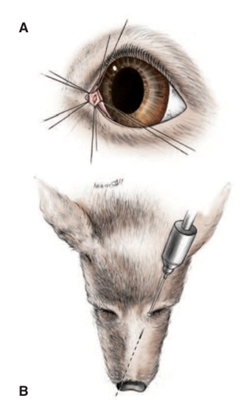
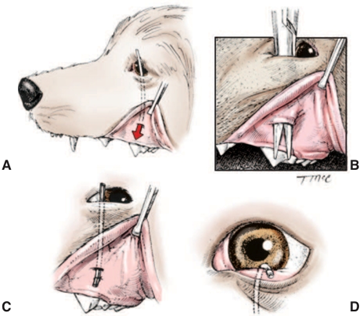
Fig.12:Conjunctivobuccostomy. A, Direction of the final drainage canal. B, A canal is made from the inferior conjunctival fornix to the oral cavity with straight hemostats. C, A tube is passed and sutured to the oral mucosa. D, The upper end of the tube is sutured to the skin in the region of the nasal canthus so as not to rub on the cornea. The tube is left in place for a minimum of 2 months. (Lavach ,1985)
- Atresia of nasal punctum
It means absence of the nasal punctum at the nostrils. The lumen of the duct is distended with saline via the lacrimal puncta and the mucosa at the nostrils is dissected until the lumen is entered.
Treatment
Lacrimal cannula is inserted for several days until the opening has been established.
- Lacrimal sac histoplasmosis
Dacryocystitis occurs in donkeys due to infection by Histoplasma species. The disease is very common in some localities in Egypt and is usually observed unilaterally but the other eye may get the infection after sometime from the first one.
Symptoms:
The medial part of the lower eyelid at the medial canthus of the eyeball becomes swollen and the conjunctiva gets inflamed. The lower punctum is dilated and transformed into rounded aperture. The lower eyelid is turned out at the medial canthus. A granulomatous tissue starts to protrude through the puncta lacrimalis of the lower eyelid and extends toward the cornea. These tissues are fleshy, rosy red in color, friable and easily detachable with moderate bleeding. Severe epiphora and blepharospasm are detected. Mucopurulent discharge may be observed in some cases. Long standing dacryocystitis may be complicated by maxillary sinusitis and purulent discharge is extruded from the nostril of the affected side.

Fig.13:Lacrimal sac histoplasmosis in a donkey.
Treatment:
The treatment is mainly surgical. The lacrimal sac is squeezed by digital pressure in early cases and retrograde flushing is performed. In advanced cases the granulomatous tissue are excised with a blunt scissors. The lacrimal sac is opened through the medial canthus, the content is squeezed and the lumen is curetted. Flushing is performed several times daily for 10 successive days with antibiotics and fungicidal solutions. Recovery is usually obtained but recurrences have been recorded in many cases.
- Keratoconjunctivitis sicca (KCS - Dry eye - Xerophthalmia)
- KCS is a disease involving the cornea and conjunctiva results from deficiency of the aqueous portion of the tear film. It is a common condition in dogs (The incidence of KCS in canine patients has been estimated at 1% Moore, 1999) and uncommon in cat and rare in other domestic animals.
- KCS is a common and important ocular disease in dogs. It should be suspected whenever chronic conjunctivitis, keratitis, or ocular discharge is present.

Fig. 14 : Early keratoconjunctivitis sicca (KCS) in a cat. Brown ocular discharge is present, the result of ocular surface inflammation KCS is commonly associated with feline herpesvirus (FHV1) infection in cats.
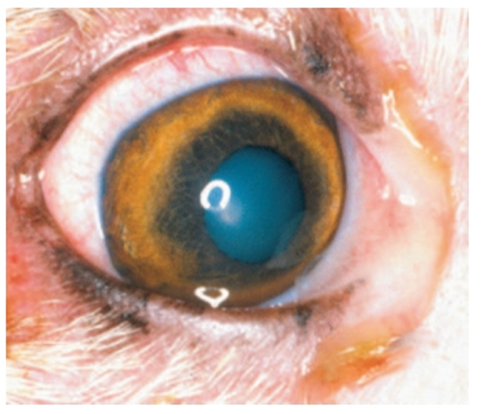
Fig.15: Mild keratoconjunctivitis sicca in a dog with a history of intermittent conjunctival hyperemia and discharge. At this stage tear production may wax and wane, and it is easy to misdiagnose the condition as intermittent conjunctivitis presumably of bacterial or allergic origin(David et al.,2008).

Fig.16: Severe keratoconjunctivitis sicca in an American cocker spaniel. Note the thick mucopurulent discharge that clings to the cornea, the hyperemia conjunctiva, and corneal roughening and pigmentation (David et al.,2008).
Causes:
1- Congenital absence of the lacrimal glands.
2- Spontaneous senile atrophy of the glands.
3- Lack of normal innervation of the glands. It may be due to traumatic causes, infection or spontaneously from unknown cause. This results in lack of lacrimal gland activity.
4- Trauma to the orbital and supra-orbital area damaging the lacrimal gland.
5- Surgical removal of the nictitans gland of the third eyelid.
6- Systemic disease, as canine distemper. The cause is a virus affecting the lacrimal and nictitans glands and may result in gland dysfunction.
7- Drug induced been associated with the nonsteroidal antiinflammatory drug (NSAID) , many sulfa derivatives, including trimethoprim sulfamethoxazole, sulfadiazine, and sulfasalazine. Sulfaderivative , with general anesthesia and topical or systemic atropine.Nutritional deficiencies as hypovitaminosis A.
8- Immune-Mediated. KCS in dogs is most often immunemediated.
9- Idiopathic causes; the majority of cases are of unknown cause.
Symptoms:
1- The clinical signs of KCS vary according to the degree of hyposecretion and the duration of the disease, also depending on whether the condition is bilateral or unilateral, acute or chronic and temporary or permanent.
2- Blepharospasm as a result of intense ocular pain and discomfort.
3- Mucoid and mucopurulent discharge. The eye and eyelids are covered with mucoid discharge. Change in the mucoid thread. As the tear production decreases, mucous production is increased as a protective mechanism for the eye resulting in increase in the size of mucous thread, change in its color into yellow green and becomes adherent to the conjunctiva.
4- Corneal changes include loss of luster, opacity, vascularization, pigmentation and keratinization.
5- Conjunctival changes. Conjunctiva becomes thick, dry and inflamed.
6- Nostrils may be normal or dry.
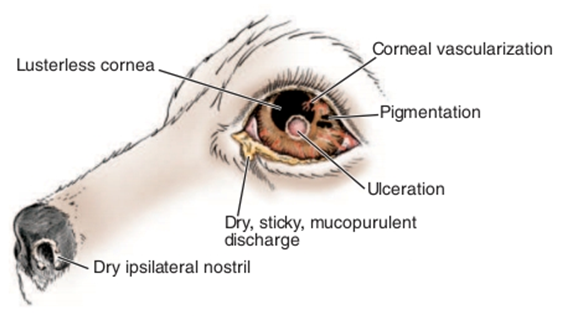
Fig.17: Clinical signs of keratoconjunctivitis sicca(David et al.,2008).
Diagnosis:
1- History of the case.
2- Clinical signs.
3- Schirmer’s tear test: The average normal tear wetting per minute is 20mm; suspicious levels are 5–10mm wetting per minute and most KCS patients exhibit wetting values less than 5mm per minute.
4- Rose-Bengal staining; 0.5% solution is instilled in the eye and the excess is flushed away with normal saline. Rose-Bengal stains the degenerated and devitalized corneo-conjunctival epithelium.
Treatment:
A) Medical Treatment:
1- Replacement of precorneal tear film by artificial tears as Methylcellulose 1%. Frequent instillation is essential.
2- Stimulation of lacrimal secretion by pilocarpine 1% solution, 1-4 drops added to the food.
3- Remove the excess of mucous by gentle and frequent washing and cleaning of the eyeball and eyelids with 5% acetylcysteine (mucomyst).
4- Control of infection by using broad spectrum antibiotics as chloramphenicol or gentamycin 4-6 times daily.
5- Anti-inflammatory agent as corticosteroids. It reduces conjunctival inflammation, conjunctival exudates, corneal vascularization and pigmentation.
B) Surgical treatment:
1- Surgical or cautery ablation of the lower punctum. This method is used to conserve the small amount of tears, if present. This technique has not been successful as KCS is usually absolute condition without any tear production.
2- Surgical reduction of the size of palpebral fissure through lateral tarsorrhaphy. Success of the procedure is dependent on some lacrimal activity.
3- Hydrophilic soft lenses applied to the cornea after application of medication to retains enough moisture and protect the cornea for several hours.
Parotid duct transportation: This operation is indicated when the medical treatment has been failed. A minimum of 3 months of medical treatment is desirable before starting surgical therapy as some dogs regain tear production during this time.
- References
1. Berdoulay A, et al. (2005): Effect of topical 0.02% tacrolimus aqueous suspension on tear production in dogs with keratoconjunctivitis sicca. Vet Ophthalmol 8:225.
2. Bistner SI, et al. 1977: Atlas of Veterinary Ophthalmic Surgery. Saunders, Philadelphia.
3. Burling K, et al. (1991): Anatomy of the rabbit nasolacrimal duct and its clinical implications. Prog Vet Comp Ophthalmol 1:33.
4. Carter R, Colitz CMH (2002): The causes, diagnosis, and treatment of canine keratoconjunctivitis sicca. Vet Med 97:683.
5. Collins BK, et al. (1986): Sulfonamide-associated keratoconjunctivitis sicca and corneal ulceration in a dysuric dog. J Am Vet Med Assoc 189:924.
6. Collins BK, et al. (1994): Immune-mediated keratoconjunctivitis sicca in a horse. Vet Comp Ophthalmol 4:61.
7. Covitz D, et al. (1977): Conjunctivorhinostomy: a surgical method for the control of epiphora in the dog and cat. J Am Vet Med Assoc 171:251.
8. David J.Maggs,Paul E.Miller (2008): SLATTER’S FUNDAMENTALS OF VETERINARY OPHTHALMOLOGYISBN: 978-0-7216-0561-6
9. Headrick JF, et al. (2004): Canine lobular orbital adenoma: a report of cases with distinctive features. Vet Ophthalmol 7:47.
10. Hicks SJ, et al. (1998): Biochemical analysis of ocular surface mucin abnormalities in dry eye: the canine model. Exp Eye Res 67:709.
11. Laing EJ, et al. (1988): Dacryocystotomy: a treatment for chronic dacryocystitis in the dog. J Am Anim Hosp Assoc 24:223.
12. Latimer CA, Wyman M (1984): Atresia of the nasolacrimal duct in three horses. J Am Vet Med Assoc 184:989.
13. Lavach JD, et al. (1984): Dacryocystitis in dogs: a review of 22 cases. J Am Anim Hosp Assoc 20:463.
14. Lim CC, Cullen CL (2005): Schirmer tear test values and tear film break-up times in cats with conjunctivitis. Vet Ophthalmol 8:305.
15. Lavach JD (1985): Lacrimal system, in Slatter DH [editor]: Textbook of Small Animal Surgery, Saunders, Philadelphia.
16. Naranjo C, et al. (2005). Characterization of lacrimal gland lesions and possible pathogenic mechanisms of keratoconjunctivitis sicca in dogs with leishmaniosis. Vet Parasitol 133:37.
17. Nykamp SG, et al. (2004): Computed tomography dacryocystography evaluation of the nasolacrimal apparatus. Vet Radiol Ultrasound 45:23.
18. Playter RF, et al. (1997): Lacrimal cyst (dacryops) in 2 dogs. J Am Vet Med Assoc 171:736.
19. Slatter D, Davis WJ (1974): Toxicity of phenazopyridine: electron microscopical studies on canine lacrimal and nictitans glands. Arch Ophthalmol 91:484.
20. Stiles J, et al. (1995): Keratectomy for corneal pigmentation in dogs with cyclosporine responsive chronic keratoconjunctivitis sicca. Vet Comp Ophthalmol 5:25.
21. van der Woerdt A, et al. (1997): Surgical treatment of dacryocystitis caused by cystic dilatation of the nasolacrimal system in three dogs. J Am Vet Med Assoc 211:445.
22. Wilkie DA, Rings MD (1990): Repair of anomalous nasolacrimal duct in a
23. bull by use of conjunctivorhinostomy. J Am Vet Med Assoc 196:1647.
24. van der Woerdt A, et al. 1997: Surgical treatment of dacryocystitis caused by cystic dilatation of the nasolacrimal system in three dogs. J Am Vet Med Assoc211:445.