NICTITATING MEMBRANE (THIRD EYELID)
| Site: | EHC | Egyptian Health Council |
| Course: | Veterinary Ophthalmology Guidelines |
| Book: | NICTITATING MEMBRANE (THIRD EYELID) |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:35 AM |
Description
"last update: 16 June 2026" Download Guideline
Table of contents
- - Acknowledgement
- - ANATOMY
- - CLINICAL EXAMINATION OF NICTITATING MEMBRANE
- - Inversion and eversion of the nictitating membrane “scrolled third eyelid”
- - Protrusion of the nictitating membrane
- - Hypertrophy of the nictitating membrane
- - Neoplasms of the nictitating membrane
- - Abscesses of the nictitating membrane
- - Prolapse of the nictitans gland (or “cherry eye”)
- - Dermoids
- - References
- Acknowledgement
We would like to acknowledge the committee of National Egyptian Guidelines for Veterinary Medical Interventions, Egyptian Health Council for adapting this guideline.
Executive Chief of the Egyptian Health Council: Prof. Dr Mohamed Mustafa Lotief.
Head of the Committee: Prof. Dr Ahmed M Byomi
The rapporteur of the Committee: Prof. Dr Mohamed Mohamedy Ghanem.
Scientific Group Members: Prof. Dr Nabil Yassien, Prof. Dr Ashraf Aly Eldesoky Shamaa, Prof. Dr Amany Abbas, Prof. Dr Dalia Mansour, Dr Essam Sobhy Dr Mohamed Elsharkawy, Prof. Dr Gamal A. Sosa., Dr Naglaa Radwan, Dr Hend El Sheikh
Scientific Editor/Authors: Prof. Dr Ashraf Aly Eldesoky Shamaa. Dr Mohamed Elsharkawy. Prof. Dr. Mohamed Mostafa Saied Amer, Prof. Dr. Shaaban Mohamed and Dr. Mohamed Moustafa Bahr Moustafa.
- ANATOMY
It’s a mobile, protective, and glandular structure lying between the cornea and the lower eyelid in the medial portion of the inferior conjunctival sac. Which is consists of the following:
1- T-shaped cartilaginous “skeleton” essential rigidity to the third eyelid, the “horizontal” arm lies parallel to and about 1.5mm from the leading edge of the third eyelid, The “vertical” arm runs perpendicular to the free edge and at its base is encircled by the gland of the third eyelid.
2- Conjunctiva covering the surfaces of the cartilage and gland on both bulbar and palpebral surfaces, Its tightly adherent at the free margin of the third eyelid but looser over the base and gland.
3- Numerous superficial lymphoid follicles under the bulbar surface (which are pinkish red, are normally present beneath the conjunctiva on the bulbar surface of the third eyelid).
4- The gland of the third eyelid. (Seromucoid and produces up to 50% of the normal tear film in dogs).
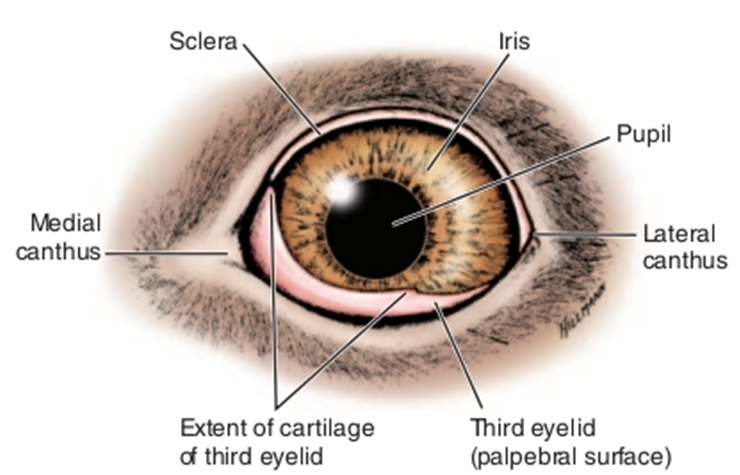
Fig.1: Diagram of the eye showing normal position of the third eyelid. (Evans, 1993).
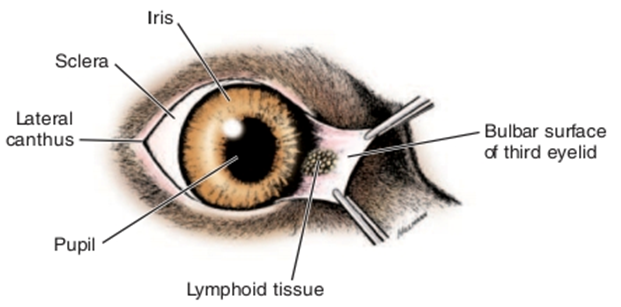
Fig.2: manually everted to show normal lymphoid follicles on the bulbar surface. ( Evans , 1993).
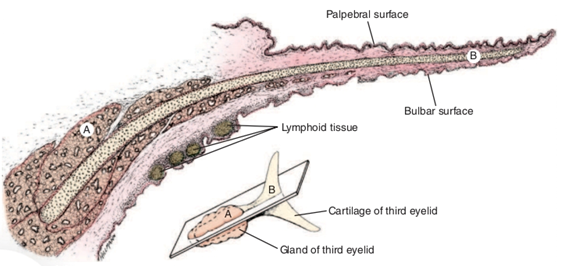
Fig.3: Transverse section of the third eyelid. A, Gland of the third eyelid; B, cartilage of the third eyelid. (Evans, 1993).
Functions of the third eyelid
1- Distribution of the precorneal tear film.
2- Protection of the cornea.
3- Production of aqueous and immunoglobulin for the tear film.
Removal of the third eyelid or its gland predisposes to the following problems:
1- Increased corneal exposure, drying of the cornea, corneal trauma, and chronic keratitis.
2- Chronic conjunctivitis (purulent and frequently resistant to treatment).
3- Decreased tear production.
- CLINICAL EXAMINATION OF NICTITATING MEMBRANE
The palpebral surface of the third eyelid is easily examined by applying digital pressure on the closed eyeball through the upper eyelid. The bulbar surface is examined by using a fixation forceps for the eversion of the membrane under effect of topical analgesia. The margin of the membrane is usually pigmented in most of domestic animals.
- Inversion and eversion of the nictitating membrane “scrolled third eyelid”
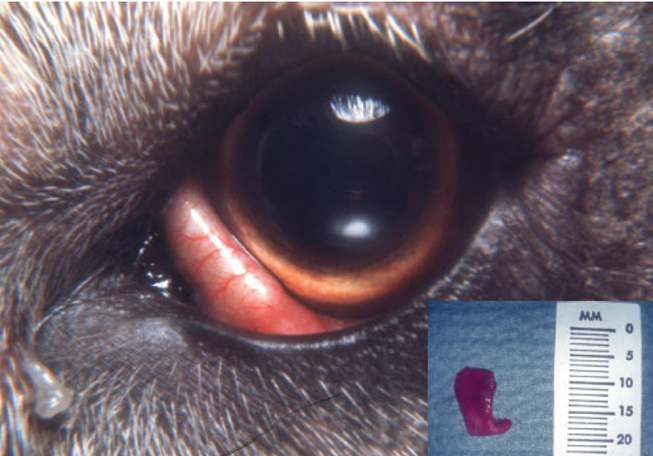
Fig.4: Everted
cartilage of the nictitans in a German Shepherd puppy. Note the leading pigmented
margin is absent and folded over (everted) exposing the defective cartilage
(see insert: bent cartilage upon removal).
Inversion and eversion of the third eyelid refer to rolling in or rolling out of the free margin of the membrane respectively. Congenital eversion seems to be more common than inversion. The condition may be unilateral or bilateral and seen mostly in young animals but may develop in middle aged animals. Traumatic injuries and improper suturing of the conjunctival membrane of the third eyelid during operations may also result in eversion or inversion.
Symptoms:
1- Increase visibility of the third eyelid.
2- Inversion or eversion of the free margin of the membrane.
3- Slight degree of conjunctivitis and mucoid discharge may be evident.
Treatment:
The aim of the treatment is the removal of the abnormally curved part of the cartilage. Sometimes the whole deformed cartilage is removed.
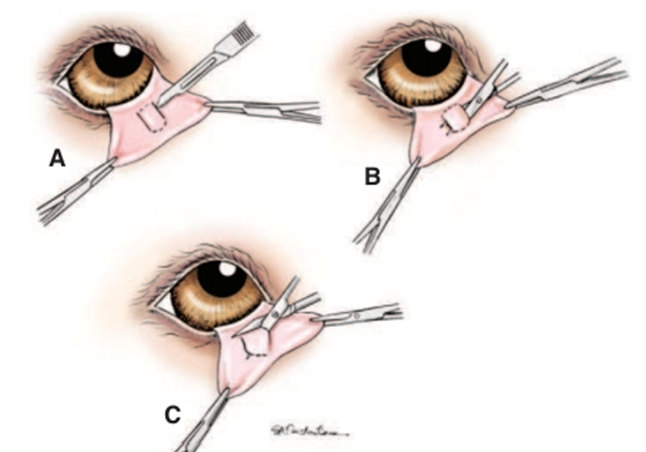
Fig.5: Surgical correction of third eyelid cartilage eversion. A, on the bulbar side of the third eyelid, the conjunctiva is incised overlying each side of the scrolled vertical part of the third eyelid cartilage. B, The scrolled cartilage and overlying conjunctiva are undermined with tenotomy scissors. C, The undermined section of scrolled cartilage and overlying conjunctiva is resected. No sutures are required. (Martin, 1970).
- Protrusion of the nictitating membrane
Protrusion, elevation or prominence of the nictitating membrane occurs in many conditions such as:
1- Congenital microphthalmia and enophthalmia.
2- Diseases accompanied by loss of weight and dehydration (decreased amount of periorbital fat).
3- Encephalitis due to rabies, tetanus or canine distemper and meningitis.
4- Postorbital space occupying lesion such as; abscesses, cysts, tumors and hematomas.
5- Swelling or symblepharon of the nictitating membrane.
6- Horner’s syndrome in dogs. It is a partial or complete loss of sympathetic innervation of the eye. The condition manifests itself clinically by miosis of pupil, protrusion of the third eyelid, ptosis, enophthalmia, small palpebral fissure and changes in intraocular pressure mainly occur in dog.

Fig.6: Protrusion of the third eyelid in a cat.
Treatment:
The specific cause is treated
- Hypertrophy of the nictitating membrane
It is a specific inflammatory and degenerative disease of the third eyelid. The first sign is bilateral inflammation and depigmentation of the nictitating membrane and mucoid discharge is evident. As the process of inflammation progressed, there is thickening and enlargement of the membrane and development of nodular irregular surface. The cause is not established. Biopsy and scraping from the conjunctiva reveal plasma cell and other inflammatory cells.
Treatment:
1. Long term steroid-antibiotic therapy (the treatment not exceed than 15-21 days).
2. Total excision of the third eyelid.
- Neoplasms of the nictitating membrane
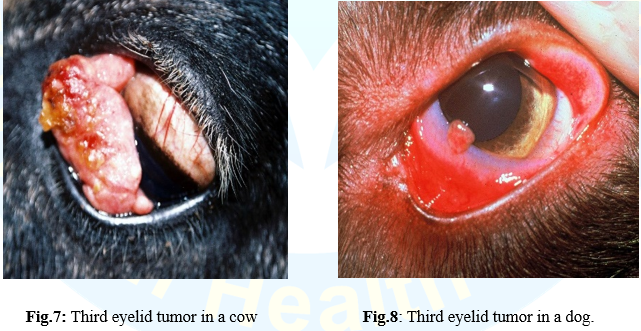
Squamous cell carcinoma is the most common tumor of the third eyelid in all species of animals. Adenoma and adenocarcinoma have been described in dogs. hemangioma or hemangiosarcoma
and adenocarcinoma of the third eyelid also are common. Unpigmented membranes are more susceptible.
Treatment:
Surgical removal of the affected area is the treatment of choice, but if the lesion is extensive, radical excision of the entire third eyelid is indicated. If the cartilage is exposed during surgical excision of the tumor, the conjunctival wound is sutured to prevent prolapse of the cartilage or gland.
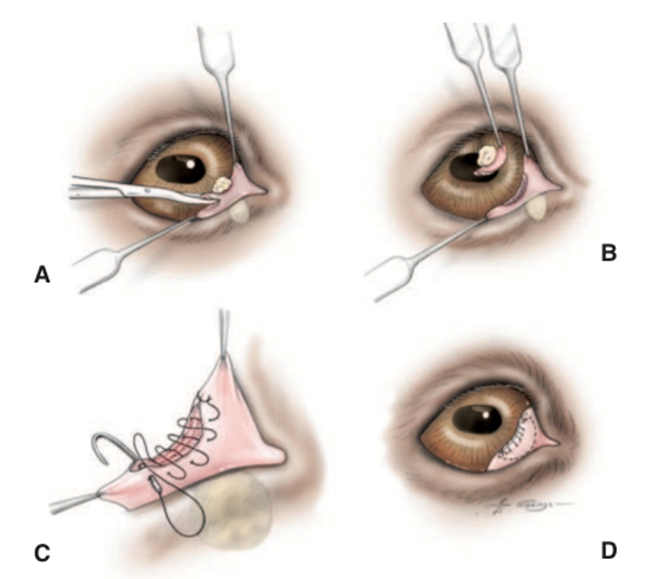
Fig.9: Surgical removal of a small neoplasm on the free margin of the third eyelid. A and B, The third eyelid is grasped with forceps or mosquito hemostats, and the mass plus adequate margin are removed with tenotomy scissors. C and D, The bulbar and anterior conjunctival surfaces are sutured over the edge of any exposed cartilage using 6/0 absorbable suture in a simple continuous pattern. Adjunctive radiation or cryotherapy may be necessary in the region outlined by a dotted line (Wilcock and Peiffer, 1988).
- Abscesses of the nictitating membrane
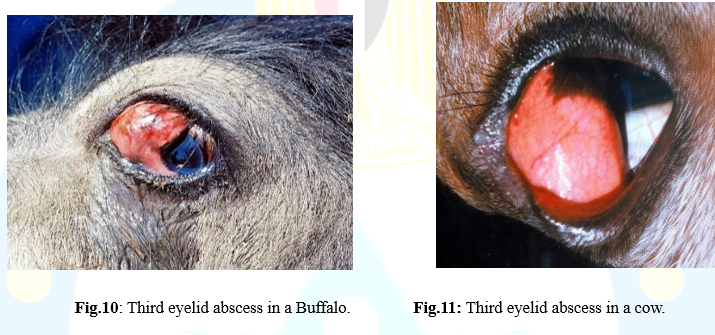
Subconjunctival abscesses of the nictitating membrane are most common in cattle and buffaloes. Foreign body penetration or trauma appears to be the main cause of the condition. The third eyelid is protruded and extends over the cornea obscuring the animal vision.
Treatment:
The abscess is incised vertically at the palpebral surface of the conjunctiva and the contents are evacuated. Lavage of the abscess cavity and the eyeball is performed with mild antiseptic solution. Antibiotic ointment is applied twice daily for 5 successive days.
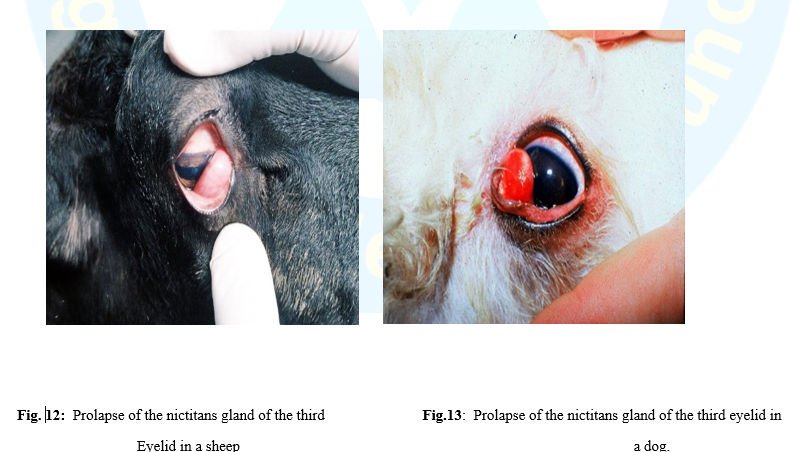
- Prolapse of the nictitans gland (or “cherry eye”)
Prolapse of the nictitans gland over the free border of the third eyelid also known as hypertrophy, hyperplasia, adenoma of the nictitans gland and cherry eye. The nictitans gland protrudes from behind the nictitating membrane as a reddish mass over its free border. The normal gland has a connective tissue bands anchoring it to the periorbital tissues at the base of the membrane. When these bands are not developed properly, the gland moves towards the free edge of the membrane. The movement of the membrane causes the gland to prolapse outwards. Inflammation and hypertrophy of the gland develop as soon as the gland is prolapsed.
Causes:
1- Congenital, perhaps hereditary weakness of the connective tissue bands between the gland and periorbital tissues.
2- Trauma to the third eyelid or orbit. The condition is seen frequently in dogs and reported in cat, sheep and buffalo.
3- It likely results from lymphoid hyperplasia (in young animals exposed to environmental antigens for the first time) and laxity of the retinaculum that should attach the third eyelid to the periorbita. This combination of events allows the gland to evert while remaining attached to the cartilage of the third eyelid.
Symptoms:
1- A rounded, cherry or pea-like mass appears at the medial canthus of the eyeball. The condition is usually bilateral.
2- Secondary epiphora and conjunctivitis may occur.
Treatment:
- Prolapsed glands of the third eyelid are treated by replacement, not by excision. Since the gland accounts for a significant part of the tear production, neither the gland nor the entire nictitating membrane should be removed. The purpose of treatment is to relocate the gland in its normal position.
- In cases of recurrence, the gland may be excised but the owner should be warned in advance about the high risk of KCS. Grasp the gland by fixation forceps and apply a mosquito artery forceps at its base for a minute and then cut it by a scissors. An alternative procedure is that the bulbar conjunctiva is incised first over the gland and bluntly dissected from it then the mosquito artery forceps is applied to the base of the gland. Hemorrhage is controlled, if present, by light pressure on the surgical wound for few minutes. Antibiotic-corticosteroid ophthalmic ointment is applied twice a day for 5 days postoperatively.
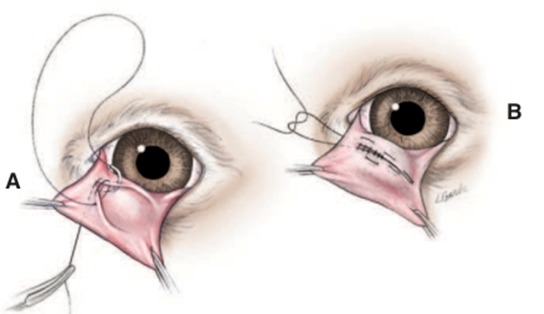
Fig.14: Surgical replacement of a prolapsed gland of the third eyelid (“cherry eye”) via a modification of the conjunctival pocket technique of Morgan. A, Two semielliptical incisions are made through the bulbar conjunctiva around the periphery of the prolapsed gland. The outer (free) edges of conjunctiva created by these incision are then apposed over the prolapsed gland using 4/0 to 6/0 absorbable suture, such as polyglactin 910 (Vicryl) in a simple continuous pattern. The initial and final anchorin knots are placed on the anterior face of the third eyelid to avoid frictional irritation of the cornea. B, The second (Cushing) layer of a continuous Connell-Cushing pattern is then placed with bites parallel to the conjunctival incisions, and, again, knots are placed on the anterior face of the third eyelid. (Stanley and Kaswan ,1994).
- Dermoids
Ectopic islands of skin located solely on the conjunctiva of third eyelid are rare. It usually extends to include the cornea.

Fig.15: Third eyelid dermoid at the free end in a cow.
Treatment
Surgical excision is the treatment of choice.
- References
1. Constantinescu GM, McClure RC (1990): Anatomy of the orbital fasciae and the third eyelid in dogs. Am J Vet Res 51:260.
2. Dugan S, et al. (1992): Clinical and histologic evaluation of the prolapsed
3. Evans HE [1993]: Miller’s Anatomy of the Dog, 3rd- ed. Saunders, Philadelphia.).
4. Komaromy AM, et al. (1997): Primary adenocarcinoma of the gland of the
5. Martin CL (1970): Everted membrane nictitans in German shorthaired
6. Med Assoc 157:1229.
7. Morgan RV, et al. (1993): Prolapse of the gland of the third eyelid in dogs: a
8. nictitating membrane in a cat. J Am Vet Med Assoc 33:333. pointers. J Am
9. Rebhun WC, Del Piero F (1998): Ocular lesions in horses with lymphosarcoma: 21 cases (1977-1997). J Am Vet Med Assoc 212:852.
10. Stanley RG, Kaswan RL (1994): Modification of the orbital rim anchorage
11. third eyelid gland in dogs. J Am Vet Med Assoc 201:1861.
12. Wilcock BL, Peiffer RL (1988): Adenocarcinoma of the third eyelid in seven dogs. J Am Vet Med Assoc 15:193.