Newborn Measurement guide
| Site: | EHC | Egyptian Health Council |
| Course: | دلائل الاجراءات التمريضية لقسم حديث الولاده |
| Book: | Newborn Measurement guide |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 8:34 AM |
Description
"last update: 22 January 2025" تحميل الدليل
- Prepared by
NICU guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Professor of Obstetrics and Gynecology Nursing |
Dr. Nagat Salah Shalabi Salama |
12 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Shaima Abdel Basset Ibrahim Salim |
13 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Hoda Al-Sayd Muhammad |
14 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Walaa Ahmed Ali |
15 |
|
member of the Nursing administration at EHA, port said branch |
Mrs. Omnia Abdel Qader Muhammad |
16 |
|
member of the Nursing administration at EHA- South Sinai branch |
Mrs. Yasser Abdel Karim Omar Abdel Jawad |
17 |
- Determination of Gestational Age
Definition of Gestational Age:
It is the period or number of weeks that the fetus spends inside the mother’s uterus from the beginning of pregnancy until birth.
Importance of Determining Gestational Age:
- Classification of newborns into full-term, premature, or post-term infants.
- Developing an appropriate treatment plan based on gestational age with early detection and management of possible complications.
- Comparing intrauterine growth of newborns with standard growth rates according to gestational age.
Methods Used to Determine Gestational Age:
Before Birth:
Calculated from the first day of the mother’s last menstrual period or by ultrasound examination.
After Birth:
Using the New Ballard Score, one of the most commonly used methods to determine gestational age during the first hours after birth by assessing neuromuscular and physical maturity.
Conditions:
- The infant should be calm and clinically stable.
- The nurse should record infant data: name, age, examination time, and gestational age.
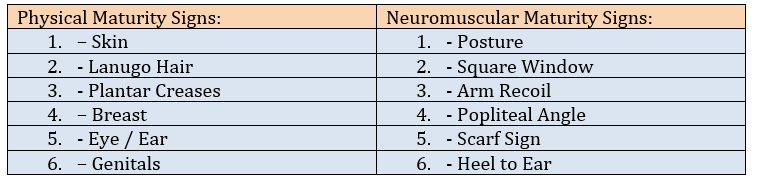
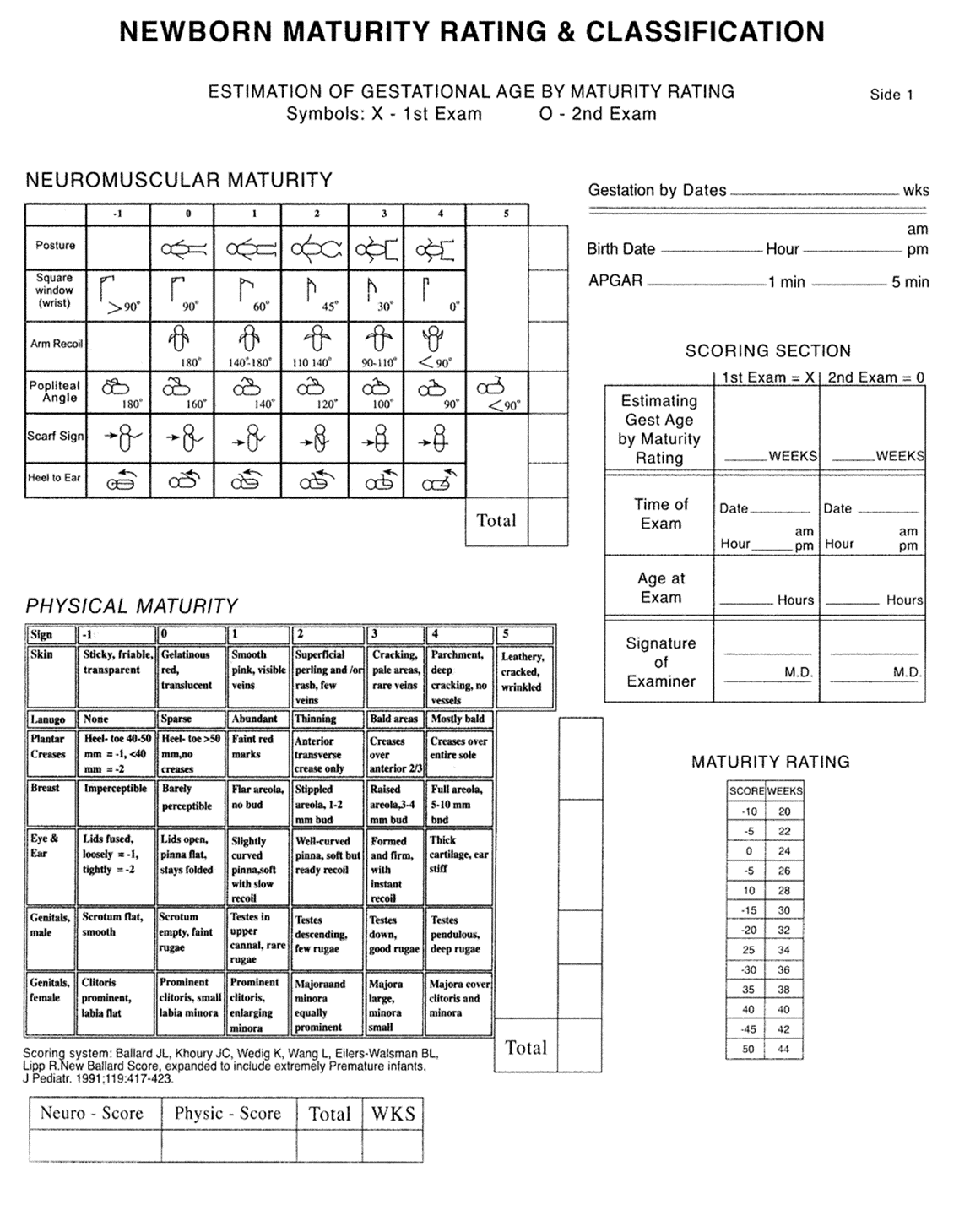
First: Assessment of Neuromuscular Maturity Signs of the Newborn
This assessment includes the following:
1. Posture
The infant’s posture is observed while lying supine, and the score is given according to the closest matching image.

2. Square Window
The hand is flexed toward the wrist, and the angle between the palm and the forearm is measured. The score is assigned according to the closest matching image.

3. Arm Recoil
The infant is placed in a supine position. The arm is flexed for five seconds, then fully extended and released. The spontaneous flexion of the arm at the elbow is observed. The angle at the elbow joint is assessed, and the score is assigned according to the closest matching image.

4. Popliteal Angle
The infant is placed supine with the diaper removed, ensuring that the pelvis is flat against the bed. One leg is flexed toward the abdomen until the infant relaxes, then the leg is gently extended. The angle behind the knee is measured, and the score is assigned according to the closest matching image.

5. Scarf Sign
The infant is placed supine. One arm is gently pulled across the chest toward the opposite shoulder until resistance is felt. The score is assigned according to the closest matching image.

6. Heel to Ear
The infant is placed supine with the pelvis flat against the bed. One foot is gently pulled toward the ear until resistance is felt. The score is assigned according to the closest matching image.

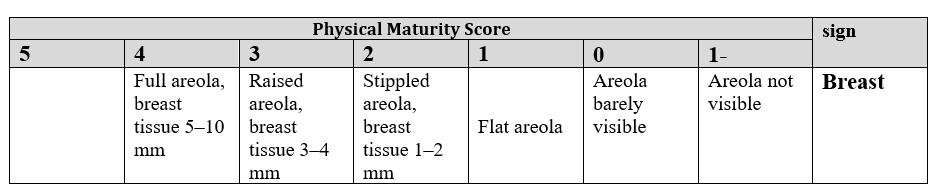
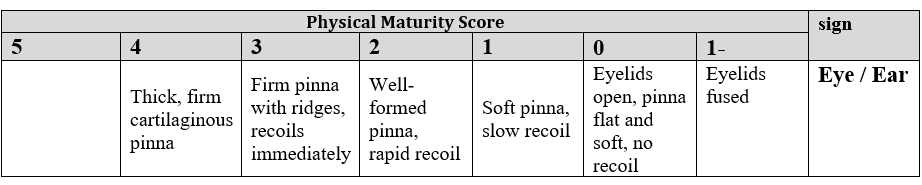
Second: Assessment of Physical Maturity Signs of the Newborn
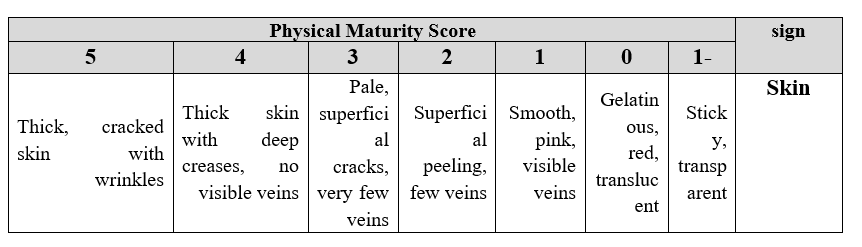
1. Skin
The skin is observed for color, thickness, and transparency of visible veins.
2. Lanugo Hair
Fine, downy hair present on the forehead, shoulders, arms, back, and legs. It is abundant in preterm infants and minimal or absent in full-term infants.

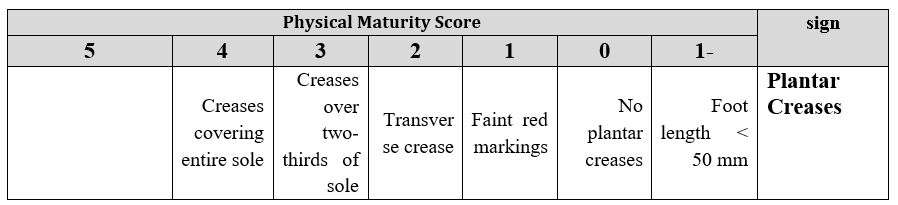
3. Plantar Creases
4. Breast
5. Eye / Ear
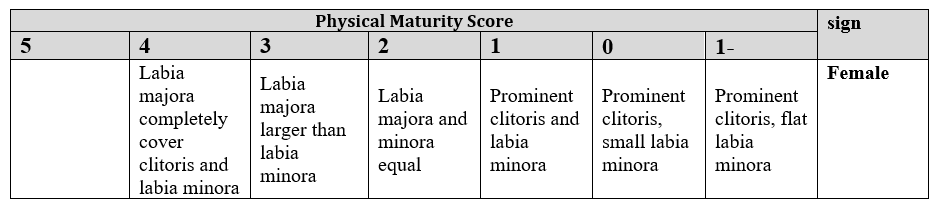
6. Genitals
Male Genitalia

Female Genitalia
Third: Calculation of Gestational Age
- The total score of neuromuscular and physical maturity is calculated.
- The total score is compared with the maturity rating chart to determine gestational age in weeks.
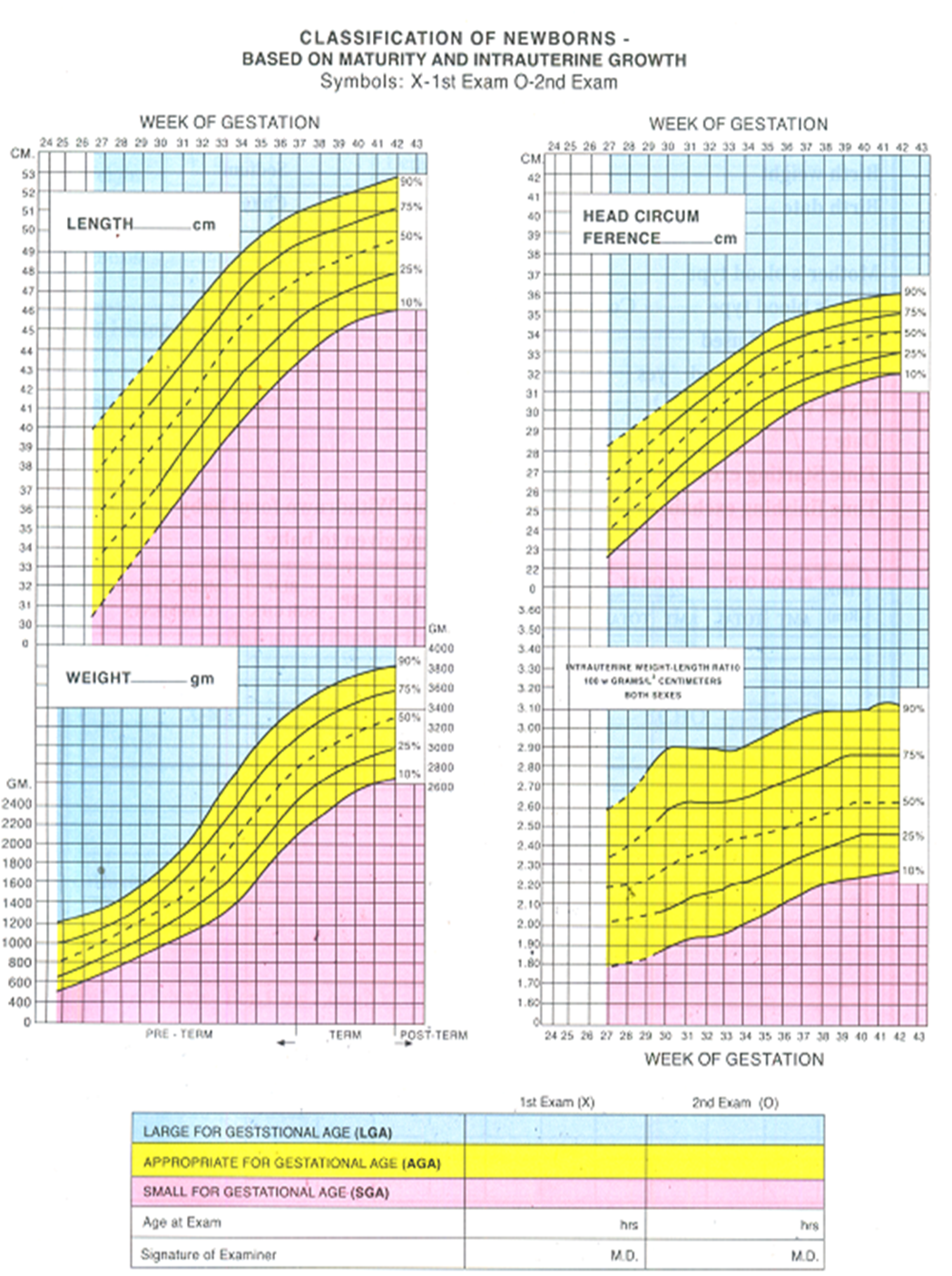
Fourth: Classification of the Newborn
- Weight (grams), length, and head circumference (centimeters) are measured and recorded.
- Weight, length, and head circumference are compared with gestational age using intrauterine growth charts.
- Newborns are classified according to gestational age and weight for gestational age.
Firstly: According to Gestational Age
|
Born before 37 weeks of gestation. |
|
|
Full-Term Infant |
Born between 37 and 42 weeks of gestation. |
|
Post-Term Infant |
Born after 42 weeks of gestation. |
Secondly: According to Weight for Gestational Age
|
SGA |
Weight below the 10th percentile |
|
AGA |
Weight between the 10th and 90th percentiles |
|
LGA |
Weight above the 90th percentile |
Exception in Gestational Age Assessment
If the newborn is clinically
unstable during the first hours after birth or affected by maternal sedative
medications that interfere with neuromuscular assessment, only the physical
maturity score may be calculated and multiplied by two to obtain the total
score.
Once the infant becomes more alert and stable within 72 hours, neuromuscular
maturity should be reassessed to determine the accurate gestational age.
- Pain Measurement
Pain Assessment for Infants Under 3 Months
- The nurse uses the CRIES pain assessment scale, which includes:
C – Crying:
- No crying = 0
- Crying with a high-pitched tone = 1
- Crying with inability to console or stop crying = 2
R – Requires Oxygen (if oxygen saturation < 95%):
- Does not require oxygen = 0
- Requires less than 30% oxygen = 1
- Requires more than 30% oxygen = 2
I – Increased Vital Signs:
- Heart rate and blood pressure within normal limits = 0
- Heart rate and blood pressure elevated but less than 20% above normal = 1
- Heart rate and blood pressure more than 20% above normal = 2
E – Expression:
- Normal facial expression = 0
- Grimacing facial expression = 1
- Grimacing with labored/noisy breathing = 2
S – Sleeplessness:
- Regular sleep pattern = 0
- Awakens frequently = 1
- Continuously awake = 2
- The nurse informs the physician of the pain score if it is greater than 3.
- The physician prescribes pharmacological pain management if the pain score is greater than 5.
Children from 3 Months to 6 Years of Age:
- The nurse uses the FLACC Scale, which includes:
- Facial expression
- Leg movement
- Activity
- Crying
- Consolability
- The nurse informs the physician of the pain score if it is greater than 3.
Children from Birth to 3 Months (CRIES Scale):
- Crying: (No crying – High-pitched crying – Inconsolable crying)
- Requires Oxygen if SpO₂ < 95%: (No – Requires < 30% oxygen – Requires > 30% oxygen)
- Increased Vital Signs:
- No change or below normal heart rate and blood pressure
- Increase in heart rate and blood pressure ≤ 20% above normal
- Increase in heart rate and blood pressure > 20% above normal
- Expression: (None – Grimacing – Grimacing with moaning)
- Sleeplessness: (No – Awakens frequently – Continuously awake)
- The nurse documents the pain assessment in the Pain Assessment Form.
C. Frequency of Pain Reassessment:
- Pain is reassessed to determine the patient’s response to the established treatment plan.
- The nurse reassesses and documents pain in the same form as follows:
- Every shift
- When the patient reports pain
- Before surgery
- After surgery
- One hour after administration of pain medication
- As per physician’s orders
D. Pain Management Protocols:
3. Pain Management:
- The attending physician establishes a pain management plan according to the pain management protocol, documents it in the clinical physician notes, and writes the orders in the physician order sheet.
- The nurse records the treatment plan in the Pain Assessment Form in the designated area.
- The assigned nurse implements and follows up the treatment plan according to the pain management form and physician instructions.
4. Education of Parents/Guardians of Newborns:
- Information is provided regarding:
- Methods of pain assessment and available treatment options
- Comprehensive medication list (dose – frequency – route of administration)
- Therapeutic effects and potential side effects
5. Discharge Plan:
- All discharged patients are provided with a pain management treatment plan.
- Growth Measurements
Growth Measurements (Weight – Length – Head Circumference)
Purpose:
To assess the appropriateness of weight, length, and head circumference in
relation to the neonate’s gestational age, as well as to monitor normal growth
and detect any changes.
Work Procedures
First: Neonatal Weight Measurement
- Weight is measured upon admission to the Neonatal Intensive Care Unit (NICU), then measured daily at a fixed time, preferably before feeding.
Equipment:
- Neonatal scale
- Clean towel
- Clean sheet
- Large cotton piece
- 70% ethyl alcohol
- Waste bin with red bag
Steps:
- Perform routine hand hygiene.
- Clean the scale using cotton soaked with alcohol.
- Place a cotton towel on the scale to prevent the neonate from feeling cold.
- Zero the scale to eliminate the weight of the sheet.
- Remove the diaper and any clothing, wrap the neonate in a clean sheet, and carry the neonate toward the scale (if the scale is fixed), or move the scale next to the incubator or crib (if movable).
- Gently place the neonate on the scale.
- Keep the hand close to the neonate without touching.
- Record the accurate weight reading.
- Return the neonate to the crib and reapply the diaper or clothing worn prior to weighing.
- Clean the scale after use and return it to its place.
- Perform routine hand hygiene.
- Document the weight in the neonate’s chart and inform the physician of any significant weight changes.
Note:
The normal birth weight for full-term neonates ranges from 2700 to 3850
grams.
Important Points When Measuring Neonatal Weight:
- Ensure the scale is zeroed.
- Place the scale on a stable, horizontal surface.
- Ensure the neonate is calm, with feet not touching any surface.
- Weigh the neonate once daily at a fixed morning time before feeding.
- If the admission weight is less than 1000 g, weight is measured twice daily (morning and evening).
- Record the weight accurately in the neonate’s chart and growth chart.
- Never leave the neonate unattended on the scale; return immediately to the crib.
- Reweigh if there is a significant discrepancy from the previous measurement and notify the physician of any major changes.
Second: Head Circumference Measurement
- Measured upon admission to the NICU, then weekly on a fixed day (e.g., every Saturday).
- In cases of intracranial hemorrhage, hydrocephalus, or birth asphyxia, head circumference is measured daily.
Equipment:
- Measuring tape
- Cotton pieces moistened with 70% ethyl alcohol
- Waste bin with red bag
Steps:
- Perform routine hand hygiene.
- Disinfect the measuring tape using an alcohol swab.
- Measure the head circumference starting from the most prominent occipital point, passing above the auricles, to the midpoint of the forehead (1 cm above the eyebrows).
- Disinfect the measuring tape after use and return it to its place.
- Perform routine hand hygiene.
- Document the head circumference in the neonate’s chart and inform the physician of any significant changes.
Note:
Normal head circumference for a full-term neonate ranges from 33 to 37 cm.
Third: Length Measurement
- Measured upon admission to the NICU, then weekly on a fixed day (e.g., every Saturday).
Equipment:
- Measuring tape or graduated measuring board
- Cotton pieces moistened with 70% ethyl alcohol
- Clean towel
- Waste bin with red bag
Steps:
- Perform routine hand hygiene.
- Place a cotton towel on the measuring board to prevent cold exposure.
- Place the neonate supine with the body fully extended.
- Position the head straight and perpendicular to the fixed headboard, centered properly.
- Ensure the head, back, thighs, and heels are in contact with the measuring surface without bending.
- Ensure the feet are perpendicular and resting firmly against the movable footboard.
- If a measuring board is unavailable, measure length using a measuring tape following the same steps, after disinfecting the tape with alcohol.
- Disinfect the measuring tape after use and return it to its place.
- Perform routine hand hygiene.
- Document the length in the neonate’s chart.
Note:
Normal neonatal length generally ranges between 47.5 and 53.5 cm.
Responsible:
- Nursing staff.
- Vital Signs Measurement
Purpose:
To ensure neonatal stability and monitor for any changes.
Work Procedures
First: Respiration
- Respiratory rate is assessed first, before other vital signs, to avoid stimulation that may lead to inaccurate readings.
Equipment:
- Stopwatch
Steps:
- Perform routine hand hygiene.
- Prepare the equipment.
- Approach the neonate quietly and observe respiration from outside the incubator without touching or moving the neonate.
- Count respirations for a full minute by observing abdominal movement.
- Document the respiratory rate, rhythm, depth, and type.
- Notify the physician of any abnormal findings.
- Normal neonatal respiratory rate ranges from 40–60 breaths/minute.
Second: Heart Rate
- Heart rate is assessed before temperature measurement, as temperature assessment may disturb the neonate and elevate the heart rate.
Equipment:
- Stethoscope
- Stopwatch
- Cotton pieces moistened with 70% ethyl alcohol
- Waste bin with red bag
Steps:
- Perform routine hand hygiene.
- Prepare the equipment.
- Disinfect the stethoscope diaphragm with an alcohol swab.
- Warm the stethoscope in the palm before contact with the neonate’s skin.
- Place the stethoscope over the apical area, just below the left nipple between the fourth and fifth intercostal spaces.
- Count heartbeats for a full minute, noting strength and regularity.
- Normal heart rate ranges from 120–160 beats/minute.
- Clean the stethoscope with alcohol.
- Return equipment to its place.
- Perform routine hand hygiene.
- Document the reading and notify the physician of any abnormal findings.
Third: Temperature
Equipment:
- Rectal thermometer (if measuring rectally)
- Petroleum jelly or paraffin oil (for rectal measurement)
- Cotton pieces moistened with 70% ethyl alcohol
- Waste bin with red bag
Rectal Temperature Measurement Steps
- Perform routine hand hygiene.
- Prepare the equipment.
- Wash the thermometer with cold water and soap, rinse and dry thoroughly.
- Disinfect the thermometer with an alcohol swab from the mercury reservoir to the tip.
- Shake the thermometer until the mercury level falls below 35°C.
- Apply a thin layer of petroleum jelly or paraffin oil to the tip.
- Place the neonate in a supine position and loosen the diaper.
- Hold the neonate’s ankles, flexing the knees upward.
- Gently insert the thermometer into the rectum at a 30-degree angle downward and backward, applying gentle pressure to the buttocks to prevent expulsion.
- Keep the thermometer in place for one minute, then remove and clean.
- Read the temperature.
- Normal rectal temperature ranges from 36.5–37.5°C.
- Refasten the diaper and allow the neonate to rest.
- Clean, disinfect, and store the thermometer properly.
- Clean and return equipment to its place.
- Perform routine hand hygiene.
- Document the temperature in the neonate’s chart.
Note:
Rectal temperature measurement should be avoided unless other methods are not
feasible. Proper technique must be followed to prevent complications.
Axillary Temperature Measurement Steps
- Perform routine hand hygiene.
- Disinfect the thermometer with an alcohol swab.
- Place the neonate in a supine position.
- Position the thermometer vertically in the center of the axilla.
- Secure the neonate’s arm against the body to hold the thermometer in place.
- Maintain the position for at least 5 minutes, ensuring continuous observation.
- Remove the thermometer and read the temperature.
- Return the neonate to the pre-measurement position.
- Perform routine hand hygiene.
- Document the temperature in the neonate’s chart.
- Return equipment to its place.
Fourth: Blood Pressure
Equipment:
- Cardiorespiratory monitor with blood pressure cuff
- Cotton pieces moistened with 70% ethyl alcohol
- Waste bin with red bag
Steps:
- Perform routine hand hygiene.
- Select the appropriate cuff size (should not cover more than two-thirds of the upper arm length).
- Disinfect the cuff using 70% alcohol.
- Wrap the cuff around the upper arm just above the elbow.
- Activate automatic cuff inflation.
- Observe the monitor until the reading appears.
- Document systolic, diastolic, and mean arterial pressure, and notify the physician of any abnormal readings.
- Disinfect the cuff with 70% ethyl alcohol.
- Perform routine hand hygiene.
Responsible:
- Nursing staff.