The Procedural Work For Cardiac Diseases
| Site: | EHC | Egyptian Health Council |
| Course: | Evidence of nursing procedures for internal sections |
| Book: | The Procedural Work For Cardiac Diseases |
| Printed by: | Guest user |
| Date: | Thursday, 6 August 2026, 7:56 AM |
Description
"last update: 25 March 2025" تحميل الدليل
Table of contents
- - Prepared by
- - Oath of the Profession
- - Nursing Care Vision and Mission
- Introduction to Cardiovascular Diseases
- - Angina Pectoris
- - Myocardial Infarction (MI)
- - Nursing Care for Patients with Myocardial Infarction (Heart Muscle Death)
- - Nursing Care for Coronary Artery Disease (CAD) Patients
- - Nursing Care for Heart Failure (Congestive Heart Failure)
- - Nursing Care for Pulmonary Edema Patients
- - References
- Prepared by
Inpatient guide
Under supervision
- Prof. Dr. Mohamed Latif, CEO of the Egyptian Health Council
Dr. Kawthar Mahmoud, Head of the Egyptian Nursing Syndicate - Member of the Senate
Prepared by
|
Title |
Name |
NO. |
|
Dean Of Faculty Nursing, Professor of Medical and Surgical Nursing, Tanta University |
Dr Afaf Abdel Aziz Abdel Aziz Basal |
1 |
|
Professor Of Critical Care Nursing |
Prof.Dr/Zeinab Hussain Ali |
2 |
|
Professor And Head of the Department of Medical Surgical Nursing. Faculty-. Benha University |
Amal Said Taha Refaie |
3 |
|
Supervisor Of the Education Sector at Port Said University |
Amal Ahmed Khalil Morsy |
4 |
|
Professor Of Medical Surgical Nursing- Faculty of Nursing- Cairo University |
Dr. Hanan Ahmed Al Sebaee |
5 |
|
Head of central administration on secondment at MOHP |
Dr Neveen ab drab al0nabi Mohamed |
6 |
|
Director Of Primary Health Care Nursing Department at MOHP. |
Maysa Hosny Ahmed Tammam |
7 |
|
Supervisor Of Technical Education- EHA |
Nancy Alaa Eldeen Abd-Elbaset Ali |
8 |
|
Supervisor Of Nursing Services Development- EHA |
Sherien Mohamed Saad |
9 |
|
Assistant Professor of Maternity and Neonatal Health Nursing - Faculty of Nursing- Ain Shams University |
Assist.Perof. Dr./Heba Mahmoud Mohammed |
10 |
|
General manager of general administration of health institutes affairs |
Dr Mai Galal Ibrahim Al-Assal |
11 |
|
Participants |
||
|
Head of nursing administration at EHA, Ismailia branch |
Ms. Nahla Kamel Mostafa |
12 |
|
member of the Nursing administration at EHA, Ismailia branch |
Ms. Maha Mohamed Saad |
13 |
|
member of the Nursing administration at EHA, Ismailia branch |
Mr. Tharwat Abdel-Al Mohamed |
14 |
|
nursing specialist at the General Administration of Nursing - MOHP |
Mr. Mona Ali Abdul Rahman Al-Katami |
15 |
|
nursing specialist at the General Administration of Nursing - MOHP |
Ms. Sherine Abdel Hakim Abdel Hakim Khattab |
16 |
|
nursing specialist at the General Administration of Nursing - MOHP |
Mr. bahaa fuoad barsom |
17 |
- Oath of the Profession
"I swear by Almighty God that I will be sincere and dedicated in my work, fear God in my profession, respect its laws and regulations, and perform my duties with efficiency and dedication.
I pledge to rely on the knowledge derived from the science of nursing in my practice, and to exert my utmost effort in caring for those entrusted to me, preserving their dignity, maintaining their confidentiality, defending their rights, and protecting them from harm.
I vow not to fear the blame of anyone in speaking the truth, to provide a safe environment for the patient, the family, and the community, and to continue developing myself, respecting and honoring those who have taught me.
I commit to working together with my colleagues in the profession for the sake of righteousness and piety.
And I testify before God that I am truthful in what I say."
- Nursing Care Vision and Mission
Nursing Care Vision in the Internal Medicine Ward
The nursing staff in the Internal Medicine Ward aspires to elevate the nursing profession and provide effective, safe, and high-quality nursing care to patients in the ward, in accordance with Egyptian, national, and international standards.
Nursing Care Mission in the Internal Medicine Ward
The nursing staff in the Internal Medicine Ward is committed to improving the health status of patients and providing the best possible nursing care that aligns with the hospital's objectives and procedures as well as the nursing management. Additionally, the nursing team works towards enhancing the scientific and practical level of all nursing staff in the ward and shifting their perspectives toward modern trends in nursing and medical sciences.
Introduction to Cardiovascular Diseases
Introduction to Cardiovascular Diseases (CVDs)
- Cardiovascular diseases are the leading cause of death worldwide.
- In 2019, approximately 17.9 million people died from cardiovascular diseases, representing 32% of total global deaths. Of these, 85% were due to heart attacks and strokes.
- More than three-quarters of deaths from cardiovascular diseases occur in low- and middle-income countries.
- Cardiovascular diseases accounted for 38% of premature deaths (under 70 years) out of 17 million deaths from non-communicable diseases in 2019.
- Most cardiovascular diseases are preventable by addressing behavioral and environmental risk factors, such as smoking, poor diet, obesity, physical inactivity, harmful alcohol use, and air pollution.
Most Common Cardiovascular Diseases
1. Coronary Heart Disease (CHD)
2. Cerebrovascular Diseases
3. Peripheral Artery Disease (PAD)
4. Rheumatic Heart Disease
5. Congenital Heart Disease
- Angina Pectoris
Definition: Angina pectoris refers to the heart muscle suffering from a sudden and acute shortage of oxygen necessary for its function, due to insufficient coronary artery blood supply. This results in a sensation of squeezing, pressure, heaviness, or tightness in the chest, and may lead to a feeling of weight on the chest.
Types of Angina Pectoris:
1. Stable Angina (Chronic Stable Angina): In this type, over time, the patient adapts to the condition, allowing for the development of collateral circulation. Painful episodes occur less frequently and are usually mild. Medical treatment typically provides complete relief to the patient.
2. Unstable Angina (Pre-infarction Syndrome): In this type, pain occurs suddenly during rest or with minimal exertion. The episodes are frequent, intense, and last longer than stable angina, sometimes extending beyond 20 minutes. The pain does not subside with rest or usual angina medications (e.g., nitroglycerin).
3. Recurrent Angina: In this type, the patient experiences multiple attacks per day and may take several nitroglycerin tablets one after another (sometimes up to 10-20 tablets per day). This condition may persist for several weeks. It may indicate either significant damage to all three main coronary arteries or could be due to the patient’s anxious or nervous psychological state.
4. Twisted or "Masked" Angina: These cases are particularly important as they occur in patients who have other medical conditions unrelated to coronary insufficiency. The pain in these cases often radiates and manifests at specific times, pointing to the site and cause of the underlying condition (e.g., cervical disc issues or gastrointestinal disorders like peptic ulcers). It is crucial to determine whether these conditions alone are causing the symptoms or if they coexist with true coronary insufficiency, which may worsen the condition.
Signs and Symptoms of Angina Pectoris:
· Pain Characteristics:
The pain typically appears in the front of the chest, behind the sternum, and
may radiate upward to the upper sternum, neck, or lower jaw. The left arm often
experiences pain, typically on the inner side near the trunk, or in the form of
a band around the other fingers of the left hand.
· Nature of Pain:
The pain is often described as crushing, squeezing, or as a vice tightening
around the chest. It may also present as pressure, heaviness, or an internal
burning sensation.
· Other Symptoms:
The individual may appear pale, sweat profusely, and experience a rapid
heartbeat with arrhythmias.
Diagnostic Methods for Angina Pectoris:
1. Medical History:
The patient is asked to provide a detailed history of the episodes, including
whether the pain is associated with physical exertion, stress, or heavy meals.
The pain's characteristics (location, duration, radiation) and any relief
factors are documented.
2. Chest X-ray:
This helps detect any heart enlargement or pulmonary congestion.
3. Coronary Angiography:
This procedure is used for diagnosis and to identify patients who may require
coronary artery bypass surgery (CABG).
4. Electrocardiogram (ECG):
In a standard ECG, ST segment depression and T-wave inversion are typical signs
of angina.
5. Stress ECG:
The patient undergoes physical exertion (e.g., on a treadmill or stationary
bike), which induces increased heart rate, blood pressure, and heart work. If
angina or ECG changes occur, it may confirm coronary artery disease.
Medical Treatment for Angina Pectoris:
1. Aspirin:
Aspirin prevents platelet aggregation, reducing the risk of clot formation and
the incidence of heart attacks and death in patients with angina.
2. Heparin:
Heparin is given to prevent clot formation. The typical dose is 5000 units
intravenously every 4 to 6 hours. ECG monitoring continues to assess the drug’s
effectiveness, and PTT (Partial Thromboplastin Time) or PT (Prothrombin Time)
tests are performed after two hours of administration and then daily.
3. Nitroglycerin (Angina Pain Relief):
Nitroglycerin dilates coronary arteries, improving blood flow to the heart.
These and other similar medications also help develop collateral circulation
(secondary blood flow pathways) in areas with poor perfusion, reducing heart
strain and oxygen demand.
4. Beta-Adrenergic Blockers:
These medications reduce heart rate, blood pressure, and myocardial
contractions, lowering the heart's oxygen demands. They also help prevent
arrhythmias and decrease the risk of heart attacks and sudden death. An example
is Tenormin.
5. Calcium Channel Blockers:
These drugs reduce myocardial contractions and relax smooth muscle in the
coronary and peripheral vasculature, helping control chest pain in unstable
angina. An example is Diltiazem.
6. Surgical Treatment (Coronary Artery Bypass Grafting -
CABG):
In this procedure, a vein (usually from the patient's leg) is removed and
grafted as a bypass between the aorta and a narrowed coronary artery. This
provides a new path for blood to reach the heart muscle, bypassing the blockage
and improving oxygen delivery to the heart.
- Myocardial Infarction (MI)
What is Myocardial Infarction?
Myocardial infarction (MI) is a term synonymous with coronary artery occlusion and heart attack, but the term "myocardial infarction" is preferred because myocardial ischemia leads to Acute Coronary Syndrome (ACS), which can result in the death of heart muscle cells.
In myocardial infarction, a portion of the heart muscle is permanently damaged due to the rupture of atherosclerotic plaques and the formation of blood clots, resulting in a complete blockage of the artery. The ranges of Acute Coronary Syndrome (ACS) include unstable angina, non-ST elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI).
Pathophysiology:
In all cases of myocardial infarction, there is a significant imbalance between the supply of oxygen to the heart muscle and its demand.
- Unstable Angina: There is reduced blood flow in the coronary artery, often due to the rupture of atherosclerotic plaques, but the artery is not completely blocked.
- Progression to Infarction: When cells are deprived of oxygen, ischemia occurs, leading to cell injury. Oxygen deprivation causes infarction or damage to the cells.
Causes:
The causes of myocardial infarction primarily involve the blood vessels.
- Vascular Spasm: This refers to a sudden constriction or narrowing of the coronary artery.
- Decreased Oxygen Supply: This occurs due to acute blood loss, anemia, or low blood pressure.
- Increased Oxygen Demand: This can be caused by a rapid heart rate, thyroid toxicity, or cocaine use.
Clinical Symptoms:
Some patients may have prior symptoms or a history of coronary artery disease, but about half of them report no prior symptoms.
- Chest Pain Location: Chest pain is the main symptom of myocardial infarction. It is characterized by persistent, crushing pain beneath the sternum, which may radiate to the left arm, jaw, neck, or shoulder blades. The pain is often described as heavy, pressing, or crushing and may last for more than 12 hours.
- Shortness of Breath: Occurs due to increased oxygen demand and reduced oxygen supply.
- Indigestion: Results from the stimulation of the nervous system.
- Tachycardia and Tachypnea: To compensate for the lack of oxygen supply, the heart rate and breathing rate increase.
- Catecholamine Response: The patient may experience cold extremities, sweating, anxiety, and tension.
- Fever: It rarely occurs in the early stages of myocardial infarction, but a slight increase in temperature may appear in the following days.
Evaluation and Diagnostic Methods:
- The diagnosis of myocardial infarction (MI) is generally based on the clinical symptoms.
- Patient History: Includes the current symptoms, a history of previous heart disease, and any other relevant illnesses, as well as a family history of heart disease.
- Electrocardiogram (ECG):
- ST-segment elevation indicates ischemia.
- T-wave elevation or inversion indicates injury.
- Q-wave development suggests prolonged ischemia or cell death.
- Cardiac Enzymes and Isoenzymes:
- CPK-MB (Cardiac Isoenzyme): Rises within 4-8 hours, peaks at 12-20 hours, and returns to normal within 48-72 hours.
- LDH: Rises within 8-24 hours, peaks within 72-144 hours, and may take up to 14 days to return to normal. A ratio of LDH1 higher than LDH2 (inverted ratio) is a helpful marker for confirming myocardial infarction if not detected in the acute phase.
- Troponin: Troponin I (cTnI) and Troponin T (cTnT): Levels rise within 4-6 hours, peak at 14-18 hours, and return to normal within 6-7 days. These enzymes are more specific for cell damage and are useful in diagnosing myocardial infarction after surgeries where CPK-MB may rise due to skeletal muscle injury.
- Myoglobin: A small molecular weight heme protein that is rapidly released from damaged muscle tissues. It rises within 2 hours after acute myocardial infarction and peaks between 3-15 hours.
- Electrolytes and Minerals: Imbalance of sodium and potassium may alter electrical conduction and impair the heart's contractility.
- White Blood Cells (WBC): Leukocytosis (10,000-20,000 WBC) usually appears on day 2 after myocardial infarction due to inflammation.
- Erythrocyte Sedimentation Rate (ESR): Elevated on day 2 or 3 after myocardial infarction, indicating an inflammatory response.
- Arterial Blood Gases (ABGs) / Pulse Oximetry: May indicate hypoxia or acute/chronic pulmonary pathologies.
- Lipids (Total Cholesterol, HDL, LDL, VLDL, Total Triglycerides, Phospholipids): Elevated levels may reflect atherosclerosis as a cause of coronary artery narrowing or spasm.
- Chest X-ray: May be normal or show cardiac enlargement, indicating heart failure or ventricular dilation.
- 2D Echocardiogram: Can be performed to assess the dimensions of the cardiac chambers, wall motion, ejection fraction (EF), and valve function.
- Nuclear Imaging Studies: Persantine or Thallium imaging assesses blood flow to the myocardium and myocardial cell status, such as the location/extent of acute or prior myocardial infarction.
- Cardiac MRI / MUGA (Multi-Gated Acquisition Scan): Assesses global and regional ventricular function, wall motion, and ejection fraction.
- Coronary Angiography: Shows coronary artery narrowing or occlusion and is often performed alongside left ventricular pressure measurement and assessment of left ventricular function (EF). This procedure is usually not done in the acute phase of myocardial infarction unless emergency coronary artery repair or cardiac surgery is imminent.
- Digital Subtraction Angiography (DSA): A technique used to visualize coronary bypass grafts and detect peripheral artery diseases.
- Magnetic Resonance Imaging (MRI): Provides images of blood flow, heart chambers, ventricular septum, valves, vessels, plaque formation, and infarcted tissue, as well as thrombus locations.
- Stress Test: Determines the cardiovascular response to physical activity (often performed with thallium imaging during recovery).
This comprehensive diagnostic approach helps in early identification and management of myocardial infarction, reducing complications and improving patient outcomes
Medical Treatment:
The medical treatment of angina aims to reduce heart muscle damage, maintain heart function, and prevent complications .
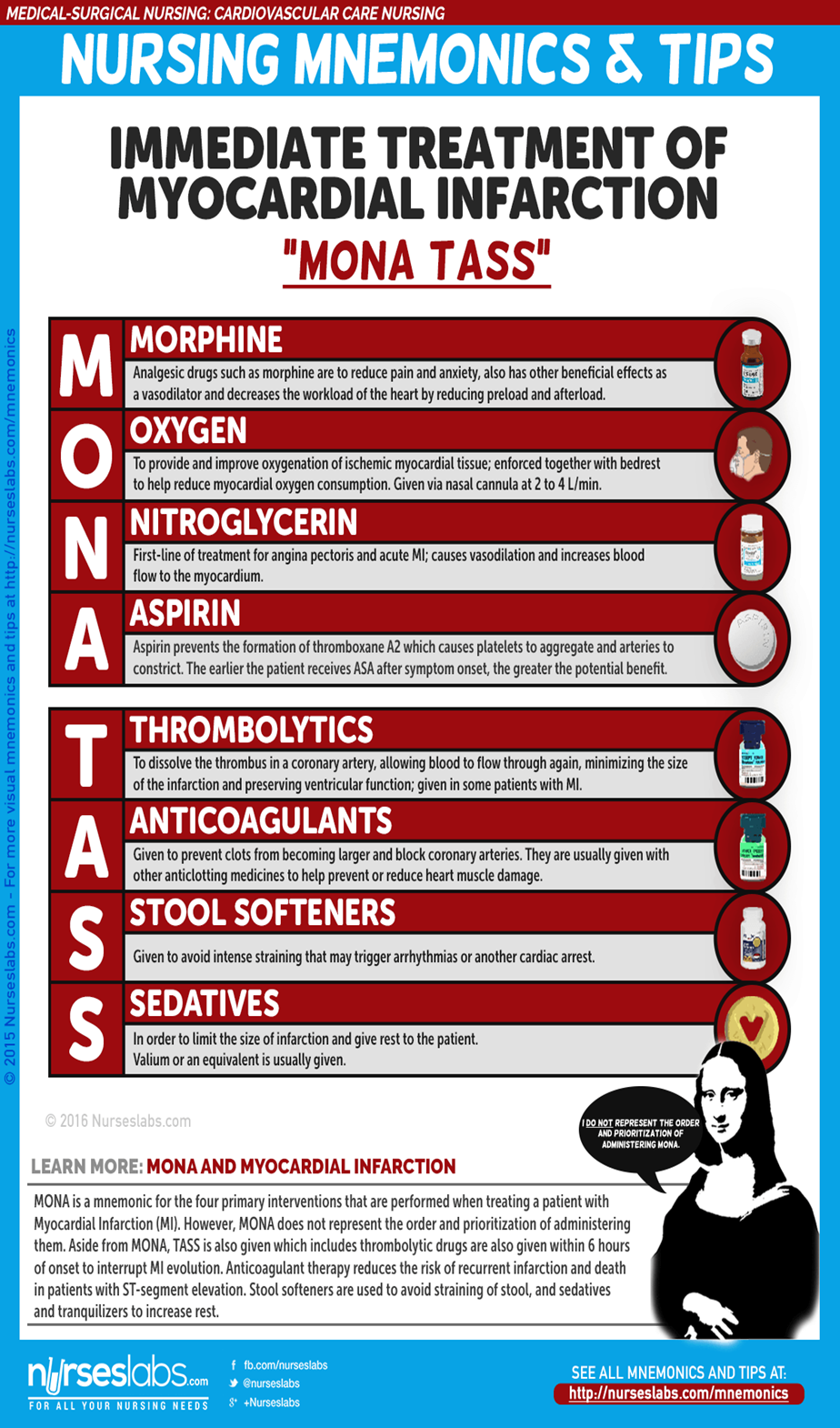
Pharmacological Treatment
- Morphine: Morphine is administered intravenously to treat Myocardial Infarction (MI) with the goal of reducing pain and anxiety.
- Angiotensin-Converting Enzyme (ACE) Inhibitors: These inhibitors block the conversion of angiotensin I to angiotensin II, reducing blood pressure and encouraging the kidneys to excrete sodium and fluids, thus decreasing the oxygen demand in the heart.
- Thrombolytic Drugs: These medications dissolve the clot in the coronary artery, allowing blood to flow again through the artery, reducing the size of the infarction and preserving ventricular function.
Emergent Percutaneous Coronary Intervention (PCI)
- This procedure is used to open a blocked coronary artery and enhance reperfusion to the area deprived of oxygen.
- PCI may also be recommended for patients with unstable angina and non-ST elevation myocardial infarction (NSTEMI), especially for those at high risk due to continuous ischemia.
Nursing Care for Myocardial Infarction (MI)
Nursing care for individuals with myocardial infarction is crucial and systematic, requiring efficient delivery of care to the patient.
Nursing Assessment
Assessment is one of the most important aspects of patient care for those with myocardial infarction.
- Assessment of chest pain that does not resolve with rest or medication.
- Monitoring vital signs, especially blood pressure and heart rate.
- Assessment for signs of dyspnea, rapid breathing, and the presence of crackles in the lungs.
- Evaluation of nausea and vomiting.
- Monitoring of urine output for any decrease.
- Reviewing the patient’s medical history.
- Performing a thorough physical assessment to identify complications and changes in the patient's condition.
- Ongoing assessment of venous access sites.
Nursing Diagnosis
Based on clinical symptoms, medical history, and diagnostic assessment data, the main nursing diagnoses may include:
- Impaired tissue perfusion in the heart due to decreased coronary blood flow.
- Risk of impaired peripheral tissue perfusion due to decreased cardiac output from left ventricular dysfunction.
- Deficient knowledge related to self-care following myocardial infarction.
Planning and Goals
The goal of nursing care planning is to establish objectives that aim for the best possible health outcomes for the patient, such as reducing pain, improving heart function, and increasing the patient’s knowledge about self-care after the infarction.
To create a care plan, the focus should be on the following:
- Alleviating pain or signs and symptoms of ischemia.
- Preventing heart muscle damage.
- Ensuring adequate respiratory function.
- Maintaining or achieving sufficient tissue perfusion.
- Reducing anxiety.
- Preventing or early detection of complications.
- Relieving/controlling chest pain.
- Ensuring adequate heart rate/rhythm to maintain sufficient cardiac output and tissue perfusion.
- Achieving a level of activity sufficient for basic self-care.
- Reducing/Managing anxiety.
- Understanding the disease process, treatment plan, and prognosis.
- Developing a plan to address post-discharge needs.
Nursing Priorities
- Pain and anxiety relief.
- Reducing the workload on the heart.
- Prevention/early detection and management of arrhythmias or life-threatening complications.
- Promoting heart health and self-care.
Nursing Interventions:
Nursing interventions must be based on the goals outlined in the nursing care plan.
- Oxygen Administration with Medication: To help alleviate symptoms and ensure adequate tissue oxygenation.
- Encourage Bed Rest with Elevated Backrest: To reduce chest discomfort and ease breathing difficulties.
- Encourage Frequent Position Changes: To prevent fluid accumulation at the lung bases.
- Frequent Monitoring of Skin Temperature and Peripheral Pulses: To assess tissue perfusion and detect early signs of poor circulation.
- Provide Information in a Clear, Supportive, and Honest Manner: To help the patient understand their condition and the necessary interventions.
- Close Monitoring for Changes in Heart Rate, Rhythm, Heart Sounds, Blood Pressure, Chest Pain, Respiratory Status, Urine Output, Skin Color, and Lab Values: To detect early changes in the patient's condition that may require intervention.
Evaluation:
After implementing the interventions as per the schedule, the nurse should verify:
- Absence of Pain or Signs and Symptoms of Ischemia (tissue oxygen deprivation).
- Prevention of Further Myocardial Damage (Heart Muscle Injury).
- Absence of Respiratory Dysfunction.
- Adequate Tissue Perfusion Maintained.
- Reduced Anxiety Level.
Discharge Guidelines and Home Care:
The most effective way to ensure that a patient follows their self-care plan after discharge is to identify their priorities.
1. Education:
- Cardiac Health Education: Educating the patient about maintaining a heart-healthy lifestyle is crucial. This includes managing risk factors like diet, exercise, and smoking cessation.
2. Home Care:
- Assist with Scheduling Follow-up Appointments: Help the patient schedule and adhere to follow-up appointments for ongoing evaluation of their heart condition.
- Cardiac Rehabilitation: Ensure that the patient follows the prescribed cardiac rehabilitation program.
3. Monitoring and Follow-up:
- Regular Monitoring: The nurse should remind the patient about regular monitoring including lab tests, ECGs, and general health check-ups to ensure early detection of complications.
4. Adherence to Medications and Diet:
- Monitor Adherence to Prescribed Diet and Medications: Ensure that the patient adheres to dietary restrictions and medication schedules as prescribed by the healthcare provider.
Documentation Guidelines:
To ensure all actions are documented correctly, the following should be documented:
- Individual Outcomes
- Vital Signs, Heart Rhythms, and Arrhythmias
- Care Plan Details
- Education Plan
- Nursing Care for Patients with Myocardial Infarction (Heart Muscle Death)
This disease affects people globally, with increasing mortality rates due to its prevalence. Deaths are more common among men aged 40-70 years. Deaths are rare among women before menopause, but when we talk about the causes of heart muscle death, they are typically linked to the same causes as arteriosclerosis (hardening of the arteries).
The term "heart muscle death" refers to the loss of function in the heart muscle, which becomes ineffective due to a simple event like a blood clot that blocks a coronary artery supplying blood to the heart muscle. This blockage prevents blood flow, causing the muscle in that part of the heart to die and undergo fibrosis, leading to tissue changes and loss of function in the affected area. This typically occurs in the left ventricle and the septum between the ventricles due to the thickness of the wall and the high blood pressure in this area. The exact location and extent of the damage depend on which artery is blocked and how efficient the collateral circulation (secondary arteries) in the heart is. Usually, the left coronary artery (left main coronary artery) is the most commonly affected.
Symptoms of Myocardial Infarction:
· Sudden Severe Chest Pain: It begins unexpectedly, without any previous exertion or stress (often resembling or preceding angina pectoris). The pain reaches its peak behind the sternum and radiates to the middle of the chest, neck, jaw, the area known as the epigastrium, both shoulders, especially the left shoulder, and the left arm.
· Nature of Pain: The pain resembles angina in terms of its nature, location, and radiation but is more intense and lasts longer.
· Duration of Pain: The pain lasts for hours, and sometimes extends for a day or two. It does not improve or disappear with rest and is unrelieved by sublingual nitroglycerin.
· Preceding Angina: Sometimes, this pain may be preceded by episodes of angina (chest pain) or it may appear suddenly and severely from the very start.
· Accompanying Symptoms: The pain is often accompanied by profuse sweating and sometimes nausea or vomiting.
· Diagnostic Confirmation: The definitive indicator of heart muscle death (myocardial infarction) is the characteristic ECG changes seen during the event.
Nursing Considerations:
For patients suffering from a myocardial infarction (heart muscle death), the nursing care focuses on immediate management of symptoms, preventing further damage, and monitoring for complications. Below are some nursing interventions to consider:
1. Pain Management:
- Administer medications such as morphine (under medical supervision) to control pain and reduce myocardial oxygen demand.
2. Oxygen Therapy:
- Administer oxygen to increase oxygen supply to the heart and prevent further ischemic damage.
3. Monitor ECG:
- Continuous monitoring of the patient's ECG to detect arrhythmias and other abnormalities that could indicate worsening ischemia or heart failure.
4. Monitor Vital Signs:
- Regularly check vital signs, including blood pressure, heart rate, and respiratory rate. Look for any significant changes that could indicate worsening conditions.
5. Assess for Complications:
- Assess the patient for signs of heart failure, arrhythmias, and potential complications such as cardiogenic shock or thromboembolic events.
6. Positioning:
- Keep the patient in a semi-recumbent position to reduce cardiac workload and improve breathing.
7. Emotional Support:
- Offer emotional support to the patient, as they may experience anxiety, fear, or confusion due to the severity of the condition.
8. Provide Education:
- Educate the patient about the importance of lifestyle changes, such as smoking cessation, dietary modifications, and exercise after recovery.
Key Considerations in Nursing Care:
1. Frequent Monitoring:
- Regular assessments of the pain level, vital signs, and ECG findings are essential.
2. Fluid Management:
- Monitor fluid intake and output to ensure proper kidney function and avoid fluid retention.
3. Collaborate with the Healthcare Team:
- Work closely with the medical team to ensure appropriate medication administration (such as anticoagulants, beta-blockers, or ACE inhibitors) and other interventions to reduce myocardial damage.
4. Preventing Complications:
- Monitor for complications such as arrhythmias, cardiogenic shock, pulmonary edema, and deep vein thrombosis (DVT).
5. Psychosocial Support:
- Provide reassurance to the patient and family, as the psychological impact of a myocardial infarction can be significant, especially due to the sudden and life-threatening nature of the event.
Conclusion:
The death of part of the heart muscle is a serious condition that requires timely intervention and careful nursing management. Immediate care, monitoring, pain relief, and providing the patient with the necessary support during recovery can significantly impact the outcome and improve the patient's quality of life after a myocardial infarction.
Complications of Myocardial Infarction:
1. Cardiac Dysfunction and Arrhythmias:
- The patient may experience heart dysfunction, including arrhythmias (irregular heart rhythms), with an increased heart rate beyond the normal range (70-80 beats per minute).
2. Heart Failure and Valve Dysfunction:
- Heart failure may occur, often leading to complications such as valvular dysfunction, especially in the mitral valve. Small blood clots may form, which are noticeable in patients who have prolonged periods of rest during their illness, resulting in clot formation in the legs and thighs.
3. Cardiac Enlargement and Congestive Heart Failure:
- Sometimes, parts of the heart may become swollen, leading to heart failure. This can also result in small clots and rhythm disturbances.
4. Pericardial Bleeding:
- Bleeding beneath the heart lining (pericardium) can occur, which may lead to sudden death.
5. Sudden Death or Delayed Death:
- Patients with fibrosis or death of heart muscle have varying outcomes. Around five cases out of every ten may experience sudden death before reaching a doctor or during the medical consultation.
- Another group may succumb to complications within one month after the infarction.
- Approximately 60% of patients do not show symptoms, though some may experience episodes of angina (chest pain).
Treatment and Nursing Management:
1. Rest and Psychological Support:
- It is critical to provide complete rest (both physical and mental) to the patient as this leads to spontaneous improvement. The goal of medication is to relieve symptoms and manage complications.
2. Pain Management:
- Immediate pain management is essential. The patient should receive morphine (or its alternatives as prescribed by the physician) to relieve the pain (typically 10 mg, administered intramuscularly or intravenously). This dose can be repeated if necessary. It is important to note that the total morphine dosage in the first 12 hours should not exceed 60 mg to avoid respiratory depression or the occurrence of nausea/vomiting.
3. Bed Rest and Monitoring for Complications:
- Rest is crucial for recovery, and it may be required for an extended period. However, bed rest can lead to side effects such as:
- Pressure ulcers (bedsores)
- Deep vein thrombosis (DVT) in the legs
- Pneumonia
- Urinary retention
- Constipation, etc.
4. Duration of Rest:
- For patients without complications, 3 weeks of rest from work may be sufficient. However, if complications arise, rest may be extended to 6 weeks. A light sedative may be prescribed to relieve anxiety, or a sleeping pill if necessary.
5. Dietary Management:
- The patient’s diet in the early weeks should be:
- Low-calorie, low-salt, easily digestible, and small, frequent meals.
- Avoid caffeinated beverages (such as tea and coffee) and smoking completely, especially during the early recovery phase.
6. ICU Care and Close Monitoring:
- It is advised to place the patient in the Intensive Care Unit (ICU) for close monitoring, immediate management of complications, and continuous medical care. This setting allows the healthcare team to manage potential complications effectively and adjust treatments as needed.
Summary:
- Complications such as arrhythmias, heart failure, valve issues, and blood clots are common after a myocardial infarction.
- Immediate pain relief, bed rest, and monitoring for complications are critical to the patient’s recovery.
- A proper dietary plan, along with avoidance of harmful substances like caffeine and smoking, is essential during the recovery period.
- Close ICU monitoring ensures that complications are detected early, and the patient's progress is optimized.
- Nursing Care for Coronary Artery Disease (CAD) Patients
Continuous nursing care in the Intensive Care Unit (ICU) plays a vital role until the patient's condition stabilizes. The nurse should monitor the following:
1. Vital Signs Monitoring:
- Pulse, respiratory rate, temperature, and blood pressure should be frequently assessed to monitor the patient's cardiovascular status.
2. Complete Bed Rest:
- The patient should be on complete bed rest to minimize physical exertion and promote recovery.
3. Leg Movement to Prevent Deep Vein Thrombosis (DVT):
- Leg movements should be encouraged regularly to prevent leg clots (DVT). Passive or active range-of-motion exercises may be recommended.
4. Strict Adherence to Medication Regimen:
- Medications should be administered as prescribed by the physician, and the nurse must monitor for any side effects or adverse reactions to drugs.
5. Monitoring Fluid Intake and Output:
- The nurse should evaluate and document the amount of fluid the patient consumes and excretes, as this can indicate kidney function, hydration status, or possible complications (e.g., heart failure or fluid retention).
6. Observation of Symptoms:
- The nurse must be alert for signs of breathing difficulties, discomfort, chest pain, and monitor food intake and medication administration to ensure the patient’s condition is progressing appropriately.
Observation and Assessment of the Patient:
The nurse should perform both direct and indirect assessments of the patient to ensure a comprehensive evaluation:
Direct Observation:
- Visual inspection: Look for signs of distress, changes in the patient’s condition, skin color, or edema.
- Listening: Assess for any abnormal sounds like wheezing, abnormal heart sounds, or irregular respiratory patterns.
- Touch: Palpate the patient to check for tenderness, temperature changes, or abnormal pulses.
Indirect Observation:
- Blood pressure measurement: Regular monitoring of blood pressure is crucial to detect signs of hypertension, hypotension, or other complications.
- Monitor equipment (e.g., ECG, pulse oximeter): Use monitoring devices like ECG (electrocardiogram) or pulse oximeter to assess heart rhythm, oxygen saturation, and overall cardiovascular stability.
|
|
||||
Eye |
|
||||
Mouth |
|
||||
Neck |
|
||||
Chest |
|
||||
Arm |
|
||||
Abdomen |
|
||||
Legs |
|
||||
Skin |
|
||||
Behavioral changes |
|
||||
|
- Increased
temperature: Indicates the presence of infection or
inflammation.
|
Duties of Nursing Staff:
1. Early Detection and Prevention of Complications:
- The nurse should direct their efforts towards the early discovery of complications and the prevention of further injuries to the heart muscle, ensuring the patient feels comfortable.
2. Continuous Monitoring in the ICU:
- Continuous monitoring of the patient’s condition while in the Intensive Care Unit (ICU), especially during intermediate care, and the ability to interpret and read the ECG to detect any complications or arrhythmias.
3. Gas Exchange Impairment:
- The nurse should be aware of the signs of hypoxia (lack of oxygen in the brain), which include:
- Blood pressure changes
- Arrhythmias
- Difficulty breathing
- Dizziness
- Headache
- Unsteadiness
- Nausea
- Anxiety
- Discomfort
- If any of these signs occur, the nurse should inform the physician immediately.
4. Administering Oxygen:
o Administer oxygen according to the patient's condition. The nurse should also care for the patient's mouth, teeth, and lips, which may become cracked due to the use of oxygen (apply cream).
o The nurse should:
- Listen to the patient's breath sounds.
- Measure the rate, depth, and rhythm of breathing every hour.
- Administer diuretics and monitor the body’s electrolyte levels.
- For chest pain, the nurse should assess and document a complete description of the pain and the activities that may have triggered it.
- Provide complete rest to reduce oxygen consumption.
- Perform an ECG during pain episodes.
- Administer pain-relieving medications and vasodilators as ordered.
5. Encouraging Smoking Cessation:
- The nurse should encourage the patient to stop smoking, as it is a major cause of the condition.
6. Care for Vomiting and Nausea:
- For patients experiencing vomiting and nausea, the nurse should:
- Position the patient comfortably (semi-sitting).
- Place a kidney dish beside the patient.
- Record and report the contents, color, quantity, and odor of vomit.
- Provide small, frequent meals and fluids.
- Administer antiemetic drugs as prescribed by the physician.
- Provide oral care.
7. Dietary Care:
- The patient may be placed on a special diet based on their condition, such as:
- Reduced salt intake (e.g., in cases of hypertension or edema).
- Reduced fats and cholesterol for patients with high cholesterol.
- Low-calorie meals with 5 to 6 small, fat-free meals daily.
- Avoid foods that may cause bloating or excessive gas.
- Avoid foods that are extremely hot or cold.
8. Reducing Anxiety:
- The nurse should help reduce the patient's anxiety by reassuring them, making them feel comfortable, and encouraging them to express their fears about the illness.
- The nurse should also encourage the patient to engage in activities (such as reading newspapers or books) to reduce fear.
9. Sexual Activity:
- The nurse should offer the following advice to the patient and their partner to enjoy a fulfilling sexual relationship while minimizing stress on the heart:
- Ensure adequate rest before sexual activity.
- Find a comfortable position for both partners.
- Consider taking nitroglycerin before sexual activity to prevent chest pain.
- Avoid sexual activity 1-1.5 hours after eating a large meal.
- Notify the physician if any of the following occur during or after sexual activity:
- Increased heart rate for more than 15 minutes.
- Chest pain not relieved by nitroglycerin.
10. Physical Exercise:
- The nurse should advise the patient to avoid strenuous physical and mental exercises, but engage in moderate exercises that do not induce chest pain, such as walking. Start with short distances in the room and gradually increase the distance over a week with continuous monitoring from the doctor.
11. Helping with Bowel Movements:
- Most patients may experience constipation, so the nurse should:
- Provide fiber-rich food and adequate fluids.
- Avoid spicy foods and provide laxatives.
- Offer bedpans to patients who are immobile, ensuring privacy.
- Develop an activity plan based on the patient’s condition and the doctor’s recommendations.
12. Medication Knowledge and Monitoring:
- If the patient lacks knowledge about the medication (including the type, dosage, frequency, side effects, and expected effects), the nurse should explain the medication regimen and encourage the patient to repeat the information.
- Encourage the patient to rest if they feel dizzy after taking medication.
- The patient should track chest pain frequency, the medication taken, its dose, and frequency.
- Advise the patient to avoid alcohol while taking the medication.
- Monitor for side effects and inform the doctor.
13. Patient Education Before Discharge:
- The nurse should plan an individual education program for the patient and their family before discharge, covering:
- Control of risk factors.
- Sexual activity.
- Medications (name, dosage, effectiveness, side effects).
- Home exercise program.
- Importance of regular follow-up and medical check-ups.
- Warning signs and symptoms requiring physician consultation (e.g., chest pain not relieved by nitroglycerin, palpitations, arrhythmias, dizziness).
- Teaching family members cardiopulmonary resuscitation techniques.
- Importance of taking nitroglycerin before exertion.
- How to measure pulse.
- Adherence to a low-salt, low-cholesterol, low-fat diet, and controlling caloric intake.
14. Health Education for Pacemaker Patients:
- Educate the family on providing a calm, respectful, and supportive environment, avoiding negativity, and following the doctor’s instructions.
15. Work and Lifestyle:
- The patient should avoid any strenuous physical or mental work. If possible, replace demanding tasks with less stressful ones.
- Daily life should be free of noise, stress, and fatigue, but this doesn’t mean complete isolation from others.
16. Rest and Environment:
- The patient should have adequate rest, and their living environment should be quiet, well-ventilated, and receive sunlight.
- Bathing water should be lukewarm (not too hot or cold), and the patient should avoid standing for prolonged periods.
17. Visiting Policy:
- Visitors should be few in number and visits should be short, providing comfort and peace to the patient. Avoid discussions that could cause stress or discomfort.
- Nursing Care for Heart Failure (Congestive Heart Failure)
Definition:
Heart failure refers to the inability of the heart muscle to pump an adequate amount of blood to meet the body's needs. This failure can be acute, leading to a sudden cessation of blood pumping by the heart, or chronic, occurring gradually with milder symptoms. Heart failure is often compensated by certain adaptive mechanisms, such as:
- Increased heart rate
- Ventricular hypertrophy (enlargement of the heart, especially the ventricle)
- Ventricular dilatation (expansion of the ventricle)
- Pulmonary congestion (abnormal accumulation of blood in the respiratory system)
Causes:
Heart failure can occur due to one or more of the following reasons:
- Reduced blood volume returning to the heart due to bleeding or dehydration.
- Excessive blood volume entering the heart due to excessive infusion of fluids.
- Impaired blood flow to the heart caused by a narrowed valve or artery.
- Damage to the heart muscle due to various types of injury.
- Increased nutritional demands due to conditions such as severe fever or pregnancy.
Goals of Nursing Care for Heart Failure:
The primary goal of nursing care is to eliminate or reduce the underlying causes of heart failure and to manage the symptoms. The specific objectives of care include:
1. Complete Physical and Resting Care:
- Ensure the patient receives full physical rest to minimize the strain on the heart and prevent further complications.
2. Digitalis (Digoxin):
- Administer Digitalis (e.g., Digoxin) as prescribed, which helps improve heart muscle contraction and control heart rate.
3. Nutritional Support:
- Provide a balanced diet with low sodium and adequate potassium, tailored to the patient's needs and the severity of their heart failure.
4. Vasodilators:
- Administer vasodilators as prescribed to relax the blood vessels, reduce the heart’s workload, and improve blood flow.
Nursing Interventions:
1. Monitoring Vital Signs:
- Continuously monitor the patient’s heart rate, blood pressure, and respiratory status, especially for signs of pulmonary congestion.
2. Fluid Balance:
- Monitor and control the patient’s fluid intake and output, ensuring the patient does not experience fluid overload.
3. Oxygen Therapy:
- Administer oxygen as necessary to improve oxygenation, especially if the patient shows signs of respiratory distress.
4. Positioning:
- Position the patient semi-sitting or upright to improve breathing and reduce the workload on the heart.
5. Medications:
- Administer prescribed medications, such as diuretics to reduce fluid retention and ACE inhibitors to relax blood vessels, and monitor for any side effects.
6. Patient Education:
- Educate the patient and family about the importance of adherence to medications, lifestyle modifications (e.g., low-sodium diet, quitting smoking), and follow-up care.
7. Monitoring for Complications:
- Monitor for pulmonary edema, renal failure, or cardiogenic shock, and report any signs of worsening heart failure to the physician immediately.
By adhering to these guidelines, nurses can help manage heart failure symptoms, prevent complications, and improve the patient’s quality of life.
Reducing Fluid and Sodium Retention in the Body:
To manage and reduce fluid and sodium retention, the following measures should be taken:
1. Reduce Sodium Intake in Diet:
- Encourage a low-sodium diet to prevent further fluid retention and help control blood pressure. Avoid salty foods and processed meals.
2. Diuretics:
- Administer diuretics as prescribed to help eliminate excess fluid and sodium from the body through urine. Monitor the patient for any side effects, such as dehydration or electrolyte imbalances.
3. Limit Fluid Intake:
- Restrict fluid intake based on the patient's condition and the physician's recommendations to prevent fluid overload.
4. Reduce Stress:
- Manage and reduce patient stress through relaxation techniques, mental support, and environmental changes. Stress can exacerbate symptoms of heart failure and increase fluid retention.
5. Oxygen Therapy:
- Provide oxygen therapy to improve oxygenation and reduce respiratory distress, especially in cases of pulmonary congestion.
6. Remove Pleural and Peritoneal Effusion:
- Draining pleural or peritoneal effusion (fluid accumulation in the chest or abdomen) may be necessary to relieve pressure on the lungs and other organs, improving breathing and circulation.
7. Patient Education:
- Educate the patient about their condition, the importance of adhering to prescribed medications, monitoring fluid and sodium intake, and recognizing signs of worsening symptoms (e.g., swelling, shortness of breath).
These measures, when implemented correctly, will help manage fluid retention, reduce the strain on the heart, and improve the patient’s overall well-being.
Role of Nursing Staff Towards the Patient in Heart Failure:
1. Place the Patient in a Quiet, Cool Room:
- Ensure the patient is in a calm and cool environment to help them rest and sleep, which will aid in their recovery.
2. Ensure Items are Within Reach:
- Keep all necessary items within the patient’s reach, such as medications, water, and personal items, to minimize strain on them.
3. Maintain Comfort and Restful Position:
- Make sure the patient is consistently positioned comfortably to avoid unnecessary strain on the heart and improve circulation.
4. Provide Emotional Support:
- Reassure the patient about their health condition, offering support and encouragement to help them cope with their anxiety or fear.
5. Encourage Post-Discharge Rest:
- Inform the patient about the importance of rest once they return home, especially after hospitalization, and ensure they understand the significance of adhering to a proper recovery plan.
6. Educate the Patient on Digitalis Poisoning Symptoms:
- Teach the patient the signs of digitalis toxicity, such as:
- Nausea
- Vomiting
- Diarrhea
- Headache
- Depression
- Anxiety
- Dizziness
- Seizures
- Delirium
- Memory loss
- Irregular heartbeats (either fast or slow)
- Hives (urticaria)
- If any of these symptoms occur, stop the medication immediately and notify the doctor.
- Administer potassium chloride if advised by the physician.
Before Administering Digitalis:
1. Check the Patient’s Pulse:
- Measure the pulse for one full minute using a stethoscope on the patient’s chest.
2. Assess Pulse Regularity:
- Carefully monitor and record the pulse rate, noting whether it is regular or irregular.
3. Action if Pulse Rate is Low or High:
- If the pulse is too fast or less than 60 beats per minute, hold the digitalis dose and immediately inform the doctor.
4. Monitor for Digitalis Toxicity:
- Observe the patient for any symptoms of digitalis toxicity, including nausea, dizziness, or irregular heart rhythms.
5. Ensure Adequate Potassium Intake:
- Provide potassium-rich meals to prevent electrolyte imbalances, as digitalis can affect potassium levels.
6. Avoid Sodium-Rich Foods:
- Avoid foods high in sodium (e.g., peanuts, chips) and ensure the patient stays away from salt entirely, as this can worsen the condition.
7. Monitor Weight:
- Weigh the patient daily at the same time (typically before breakfast) and using the same scale to monitor fluid retention.
8. Care for the Skin:
- Pay extra attention to skin care, especially in areas that may be swollen, as these areas are more prone to cracking.
9. Oxygen Therapy:
- Administer oxygen therapy if the patient experiences difficulty breathing to ensure proper oxygenation.
10. Document Findings:
- Document everything meticulously, including vital signs, patient observations, any adverse reactions, and interventions, to ensure continuity of care.
By adhering to these guidelines, nurses can help manage the symptoms of heart failure, prevent complications, and provide the best possible care to the patient.
- Nursing Care for Pulmonary Edema Patients
Definition:
Pulmonary edema is the congestion of the lungs due to the accumulation of excess blood in the blood vessels of the respiratory system. This results in significant difficulty in breathing. Pulmonary edema commonly occurs as a result of left-sided heart failure, which causes difficulty in the return of blood from the lungs to the heart. This leads to blood accumulation in the lungs, causing pulmonary edema. If left untreated, pulmonary edema can lead to suffocation and be fatal.
Symptoms:
- Severe difficulty in breathing, especially in the horizontal position.
- Paleness of the face.
- Increased heart rate.
- Expectoration of large amounts of bloody sputum.
- Cyanosis (blue discoloration of the skin and mucous membranes due to lack of oxygen).
The Primary Goal of Nursing Care for Pulmonary Edema:
The main objective of nursing care for these patients is to ensure that the patient receives the necessary amount of oxygen for proper respiratory function and to alleviate symptoms.
Role of Nursing Staff Towards the Patient:
1. Positioning the Patient:
- Place the patient in a 90-degree or 45-degree angle (sitting upright) or allow them to sit on a chair. This position aids the patient in breathing more easily by reducing the workload on the heart and improving lung expansion.
2. Oxygen Therapy:
- Administer 8 liters of humidified oxygen per minute, as this helps maintain adequate oxygen saturation in the blood and reduces breathing difficulty.
3. Medication Administration:
- Digoxin: Give as prescribed to help strengthen the heart's contraction and improve its pumping efficiency.
- Diuretics: Administer Furosemide (Lasix) in doses ranging from 40 mg to 120 mg intravenously (slow infusion) to help remove excess fluid from the body.
- Aminophylline: Administer 250 mg to 500 mg IV to dilate the airways, facilitating easier breathing by relieving bronchospasm.
4. Mechanical Ventilation (If Needed):
- In severe cases of respiratory failure, the patient may need mechanical ventilation to assist with breathing and support life. This is especially critical if the patient's oxygen levels are critically low.
General Care Considerations:
- Monitor vital signs closely, especially respiratory rate, heart rate, and oxygen saturation levels.
- Regularly assess the patient’s lung sounds for crackles or wheezes, indicating fluid accumulation.
- Provide psychological support to alleviate anxiety, as patients with pulmonary edema often feel panic due to their inability to breathe.
- Ensure fluid balance monitoring (input/output), as diuretic therapy can lead to dehydration or electrolyte imbalances.
By following these interventions and closely monitoring the patient's condition, nurses can play a vital role in improving the patient's oxygenation and preventing further complications associated with pulmonary edema.
- References
- National Institutes of Health (NIH): https://www.nih.gov/
- Centers for Disease Control and Prevention (CDC): https://www.cdc.gov/
- American Heart Association (AHA): https://www.heart.org/
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine by Eugene Braunwald
- Harrison's Principles of Internal Medicine (various editions)