
Book
Mare infertility
- A- Congenital affections
1. Gonadal dysgenesis
It is associated with defects of the X chromosome, including XO (equivalent to Turner’s syndrome in humans, a chromosomal disorder in which cells have only one X chromosome or are partially missing an X chromosome). It may be seen in mares with apparently normal karyotypes. There is a congenital failure of development of the ovaries which appear as a “streak” (small, almost cylindrical) with no follicular activities. The tubular portion of the female tract is intact but juvenile. The clinical picture is phenotypically normal female mares with small uteri and infantile ovaries. The ovaries lack germ cells and only have stroma.
- Diagnosis based on: a history of non-previous pregnancy, Chromosomal analysis, Rectal palpation, and ultrasonography which reveal small or absent ovaries with no follicular activity are seen if they are present
- Treatment: No treatment is possible for these mares.
2. Hermaphrodites (Intersex)
There are 3 main classes of intersex described in horses: true hermaphrodites, female-pseudohermaphrodites, and male-pseudohermaphrodites. The equine hermaphrodites are usually male pseudo-hermaphrodites including 64 XX and 64 XY karyotypes. Mares generally display masculinization of the external genitalia with cryptorchidism, ventral displacement of the vulva, and a penis-like structure that often resembles a clitoris.
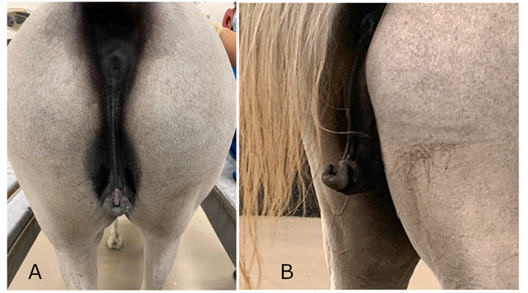
Figure (1): Mare intersex (Pompermayer et al., 2024)
3. Testicular Feminization Syndrome
It is another form of male hermaphrodite in which mares are genetically male with a 64XY karyotype. The mare has normal external genitalia while the cervix and uterus are identifiable, and the vagina is short. Two abdominal testicles are present in the general proximity of normal female ovaries. The mare shows aggressive, stallion-like behavior. It acts aggressively towards other horses and defecates in a pile in her enclosure. It exhibits Flehmen's response and vocalizes in the presence of cycling mares.
- There is no treatment for these conditions.
4. Congenital cervical abnormalities:
Congenital abnormalities of the cervix involve the Müllerian duct system (paramesonephric duct), and are usually associated with several gonadal abnormalities, such as gonadal and testicular feminization. The cervical abnormalities include both aplasia of the cervix (the cervix is not identified or small amounts of rudimentary tissue are present), hypoplasia (a small but fully differentiated organ is present), and double cervix.
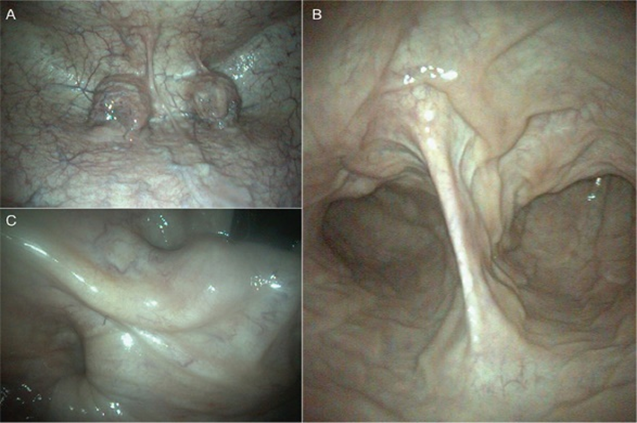
Figure (2): Endoscopic images of mare uterus showing two cervicies (A), frenulum between the 2 cervicies (B), uterine body lumen (C) (Kania et al., 2023)
5. Vaginal abnormalities
Several congenital vaginal abnormalities were recorded in mare including vaginal hypoplasia and transverse vaginal septum. The blind-ending vagina with a hypoplastic uterus beyond is more commonly found in the case of testicular feminization. From the vaginal abnormalities are the abnormalities of the hymen which include imperforate persistent hymen and septate hymen.
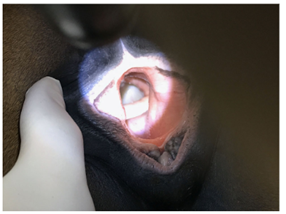
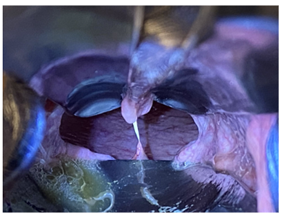
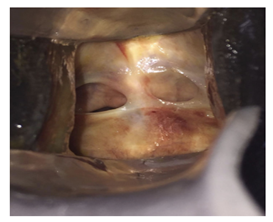
Figure (3): Imperforate persistent hymen and septate hymen (Gormley and Crabtree, 2021)
6. Abnormal perineal (vulvar) conformation
The normal vulval labia are full and firm and meet evenly in the midline, and 80% or more of the vulvar opening is below the brim of the pelvis. The defective vulvar conformation can be congenital (rare) or acquired. The abnormal vulvar conformations result in Pneumovagina or exacerbate the problem. The alterations of vulvar angle and length have been used to determine a Caslick index, which provides an index of the need to perform vulvoplasty. The normal anatomical arrangement is represented at a Caslick index lower than 150.
- Treatment: surgical correction of the abnormal conformation (Fig. 4)
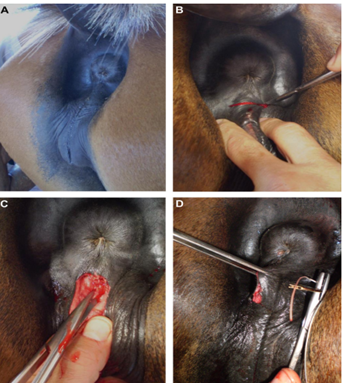
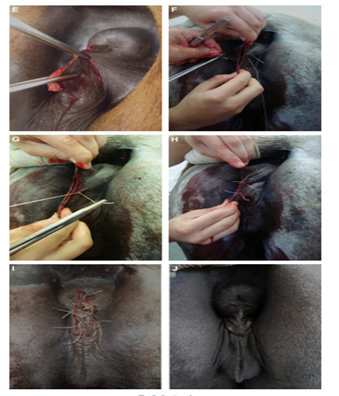
Figure (4): (A); Abnormal vulvar conformation before surgery. (B); Horizontal incision between the anus and the dorsal commissure of the vulva. (C); A 10-cm-deep internal perineum divulsion. (D); Vertical suture with horizontal interrupted U suture. (E); Vulvar horizontal incision fixation into the vertical position. (F); Horizontal U suture. (G); First U stitch. (H); Three U stitches. (I); Final result with a sequence of greater distance (2 cm) and stitches on the borders. (J); Vulva repositioned in the correct anatomical position (Papa et al., 2014).
7. Uterine abnormalities:
Several uterine abnormalities have been recorded in mare including Uterus didelphys and uterine aplasia. The uterus didelphys or uterus bicollis has a double cervix with or without a double uterus and a variable vaginal component, ranging from no abnormality to a complete separation into two halves (Fig. 5). It is associated with mosaic X chromosome aneuploidy (63 XO/64 XX).
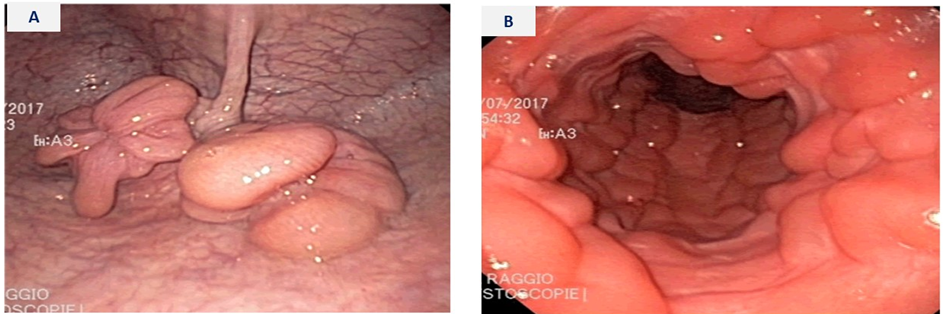
Figure (5): Endoscopic images of mare uterus showing two cervicies (A) and uterine horn and body lumen with no bifurcation (B) (Murcia-Robayo et al. 2018)
