
Book
Mare infertility
- B- The non-pathological causes:
1. Transitional period
It is the period between the anestrus season and the breeding season in mare. During this period, the sexual behavior of the mare tends to be erratic. The mare comes into heat, and the ovaries become larger and develop many small follicles that usually regress and do not ovulate. It may last for 50–70 days or more before the first ovulation of the season. At the onset of the transition period the follicular diameter reaches 20–25 mm while at the late transition, one or more follicles are ≥30 mm in diameter. The total number of follicles present on each ovary increases during the transition, and ultrasound examination reveals a ‘grape-like’ cluster of small to medium-sized follicles (Fig. 6). The transitional follicles do not produce sufficient levels of estradiol and its levels in peripheral blood remain low until approximately 5–7 days before the first ovulation of the year.
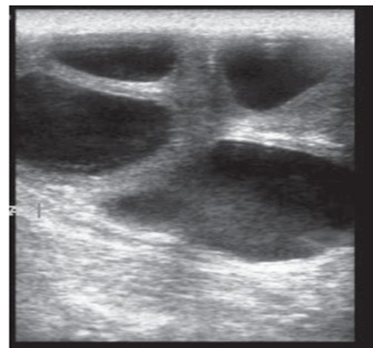
Figure (6): Ultrasonographic picture of mare ovary during the transitional period (Pozor, 2017)
2. Aging.
Broodmare can give offspring every year and the fertility peak is achieved at the age of 6–7 years. Around the age of 15 years, mares' fertility decreases gradually, unfavorably affecting the reproduction ratio. The clinical causes of decreasing fertility in older mares include anatomical abnormalities in the vulva, increased inflammation susceptibility of the uterus, uterine fibrosis, endometrial cyst formation, and increased incidence of ovulation failure. Furthermore, old mares may demonstrate limited reproductive performance because of functional changes in ovaries. In addition, older mares are susceptible to the risk of Cushing syndrome which contributes to lower reproductive performance manifesting in disrupted heat behavior and decreased fertility.
3. Prolonged luteal phase
Prolonged luteal activity usually results from the persistence of the corpus luteum or the sequential development of luteal glands. Luteal tissues originate either from an unovulated follicle or after ovulation occurring during the follicular or luteal dominance. The persistence of corpus luteum may occur with severe damage to the endometrium resulting in loss of the uterine luteolytic mechanism. The occurrence of ovulation towards the end of diestrus may confuse the origin of prolonged luteal activity. The immature diestrus corpora lutea may not respond to the uterine luteolysin, leading to prolonged luteal activity. Pseudopregnancy sometimes describes the persistence of the corpus luteum, especially when the luteal persistence is caused by embryonic loss after the embryo has blocked the uterine luteolytic mechanism.
This condition can be treated using PGF2α.
4. Shortened luteal phase
The shortened luteal phase is attributed to premature luteolysis which is commonly associated with endometritis due to the production of prostaglandin by uterine inflammation or bacterial endotoxin production.
Diagnosis and Treatment require an endometrial culture and a biopsy to confirm the endometritis and microorganism identification. The treatment of endometritis usually results in the return of normal diestrus intervals.
5. Persistent estrus
It is a constant or erratic estrus behavior. The affected mares are being irritable, kicking when their sides are touched, leaning on the handler, striking, urinating, or wringing their tails. Furthermore, it shows signs of agitation, discomfort, or submission. Persistent estrus occurs due to several factors including the seasonal transition, ovarian pathology as gonadal dysgenesis or granulosa cell and related tumors, vaginal inflammation due to a foreign body, or aspiration of air into the vagina when the mare is working (mares with little body fat), and abnormalities of the bladder or urethra, such as cystitis or urethral masses, may result in frequent urination that is interpreted as persistent estrus. The pregnant mares may show constant or irregular estrus in response to teasing by a stallion. During the intense training, the mares usually show agitated, estrous-type behavior which is termed “submissive, cowering behavior”. In the cowering behavior, the mare is resentful of the approach of a stallion when teased, and appears fearful with the attempt to escape.
Diagnosis depends:
The history of erratic estrus behavior and the response of the mare to the advances of the stallion Rectal palpation and ultrasonographic examination to differentiate between the different causes.
Treatment: it depends on the cause itself; in case of congenital affections (gonadal dysgenesis), the animals must be discarded from breeding. In case of urogenital inflammation, the animal will receive a course of local and systemic antibiotics and anti-inflammatories with a period of sexual rest.
6. Nymphomania
Nymphomania in mares is a high sex drive or mares who act like stallions characterized by excessive estrus-like behavior, hypersensitivity, and aggressiveness against other horses and people. It is attributed to several factors including the granulosa cell tumor and persistent ovarian follicles. Mares may exhibit similar behavior because of persistent estrus during spring transition, bad temper, especially during estrus, or psychological problems. The main symptoms of the in case of nymphomania are hypersensitivity in dermal areas of the hindquarter, tail swishing, and frequent urination, which often results in decreased performance. The symptoms often aggravate during estrus.
Diagnosis and treatment depend on the cause: The persistent follicle is treated with gonadotropins or luteinizing hormone or increasing daylight to ≥16 hr. The granulosa cell tumors require surgical resection.
7. Pseudopregnancy (False pregnancy)
It is a syndrome in which non-pregnant mares that have been bred do not return to estrus. In mares, 5 to 10 % of estrous cycles end in false pregnancies It occurs due to the presence of CL beyond the normal two-week lifespan which results in persistent progesterone production. Several causes are responsible for pseudopregnancy including early embryonic death (EED) after 15 days of gestation with the persistence of the corpus luteum that results in a prolonged luteal phase with a tightly closed cervix and tense and tubular uterus. Furthermore, false pregnancy can occur due to diestrus ovulations, severe uterine pathology, and potentially inadequate prostaglandin release.
Diagnosis depends on the determination of true pregnancy with the presence of the fetus and its fluids and membrane and differentiates it from the pseudopregnancy with persistent CL and an empty uterus.
Treatment: A single dose of prostaglandins will destroy the retained CL, and the mare will return to estrus in three or four days.
8. Poor body condition score.
Body condition scoring (BCS) is a method of estimating the amount of fat on a horse’s body. It is rated on a scale of one to nine. The rating is based on palpation and visual assessments of fat deposits in different body areas (Fig. 7). The ideal BCS for a given horse will depend on the stage of production and should range between four and seven. The BCS of six is ideal for mares going into the breeding season.
The poor body condition due to insufficient energy intake affects the fertility of the broodmares and leads to incomplete follicular maturation, delayed and irregular estrous cycles, reduced conception rates, and higher incidences of embryonic death and/or fetal resorption.
In horses, obesity is defined with a BCS of 8 (fat) or 9 (extremely fat), whereas horses with a BCS of 7 are considered overweight. Mare obesity has adverse effects on reproductive performance including alterations in the duration of the breeding season and the duration of the estrous cycle, early embryonic death, placental restriction, and lowered birth weights.
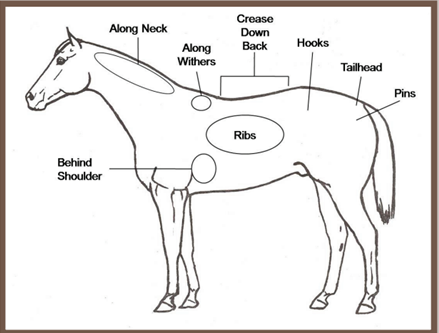
Figure (7): BCS; palpation and visual assessments of fat deposits in different body areas (Henneke et al., 1983).
9. Insulin resistance (IR)
Equine metabolic syndrome (EMS) in the horse is defined as obesity, and insulin resistance (IR) with high blood insulin levels. It can be hazardous to pregnant mares if not treated and mares may be at risk of fetal compromise and abortion. IR is the reduction in tissue sensitivity to circulating insulin (IR), associated with obesity and altered fat metabolism. Both obesity and IR have been associated with abnormal length of the breeding season and length of the estrous cycle in the broodmare. The increased circulating levels of insulin disrupt gonadotropin secretion and accordingly reproductive function.
