
Book
Mare infertility
- C-The pathological causes of mare infertility
a- Ovarian affections
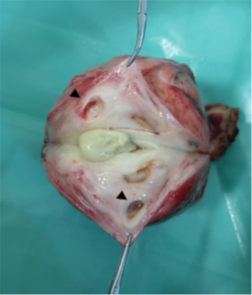
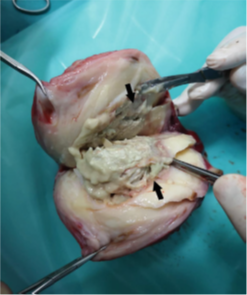
1) Granulosa cell tumor (GCT):
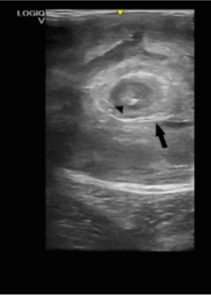
Background: Granulosa theca cell tumor, the commonest tumor within the equine ovary, essentially causes anestrus. They susceptible mares between 5-7 years old. It is usually benign and affects a single ovary. The ovaries are either polycystic or large solid structures and may weigh several kilograms. The most owners complain are associated with behavioral changes associated which include aggressiveness or stallion like behavior and constant or erratic estrus and anestrus with about equal frequency.
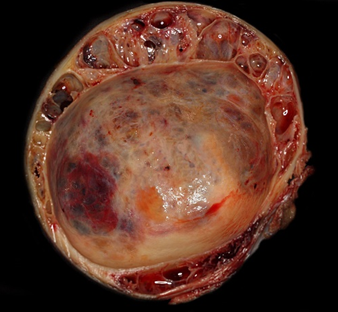
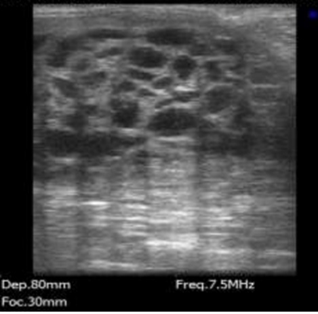
Fig. 1 Granulosa cell tumor with honeycomb structure in the marginal area and formation of a large central cyst.
➡️Symptoms demonstrated by mares with GCT depend on the hormones secreted by the tumors.
• Estrogen, the most common, may result in nymphomaniac behavior (prolonged estrus) in the absence of ovulation.
• Testosterone-producing cysts result in stallion-like behavior.
• Progesterone is associated with constant anestrum/diestrus like behavior.
• Inhibin causes the characteristically small contralateral ovary, due to negative-feedback effects on FSH.
➡️Diagnosis:
(1) History (abnormal behavior or cyclicity)
(2) Repeated rectal palpation and ultrasonography.
▪️ In palpation, the affected ovary is usually large, smooth-walled and spherical with typically absent ovulation fossa while the contra lateral ovary is usually small and inactive. The affected may be cystic and/or abnormally firm.
▪️ In ultrasound examination, the ovaries are either polycystic or large solid structures with marked increase in size (10-20 cm in diameter but may be 40 cm or larger).
(3) Hormonal assay: Testosterone, inhibin and anti-Mullerian hormones assessment. Serum inhibin and testosterone are elevated in 87% and 54%, respectively, of mares with granulosa cell tumors.
▪️ A serum testosterone concentration of >100 pg/ml is considered diagnostic for a GCT, specially in those exhibit stallion-like behavior.
▪️ Serum levels of anti-Müllerian hormone (AMH) have been shown recently to be a reliable means of identifying GCT as it is produced by granulosa cells and in healthy mares serum The sensitivity of AMH for detection of known GCTs is 98%, compared to sensitivities of 80% for inhibin, 48% for testosterone and 84% for the combination of inhibin and testosterone. Median serum AMH in mares with histologically confirmed GCTs is 66.0 ng/ml. Median serum AMH in reproductively normal, non-pregnant mares is 0.30 ng/ml, and in pregnant mares is 0.22 ng/ml.
(4) Differential diagnosis: clotting hematoma - Ovarian teratomas
▪️ A clotting hematoma can be differentiated from a GCT by the normal activity of the controlled ovary, normal cyclicity, and the presence of the ovulation fossa on the ovary. A hematoma causes enlargement of only one pole and regresses over time (usually within 30 days).
▪️ Ovarian teratomas, arising from germ cells and containing hair, teeth, bone, cysts, etc., have been reported but very rarely occur and, unlike teratomas seen in stallions, are benign. They are unilateral in occurrence, allowing the other ovary to function normally; pregnancy rates may or may not be affected significantly.
➡️Treatment: Surgical removal of the affected ovary.
▪️ Most mares return to normal estrous cycles within 6-8 months following the ovariectomy, with a range of 2-16 months.
▪️ Fertility usually returns to presurgical status after estrous cycles have been re-established. Approximately 75% of mares resume normal cyclicity within 2 years after removal of GCT.
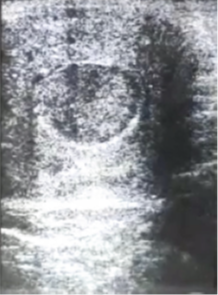
2) Hematoma formation:
It is characterized by failure of normal ovulation of the dominant preovulatory follicle.
Diagnosis: This depends on daily ultrasonographic monitoring of follicular growth during estrus. The findings include:
▪️ Normal follicular growth up to about ovulatory size (35-40 mm); however, these follicles continue to grow rapidly and reach to a large size (60-90 mm).
▪️ Echogenic particles at the time of follicle enlargement. The echogenicity increases and apparent clotting occurs.
➡️Treatment: No specific treatment for this syndrome is currently known. Treatment with hCG or suppression of follicular activity with progesterone followed by prostaglandin has no effect on hematoma formation.

Fig. 2 Ultrasound image of an ovarian hematoma. Source: . Card (2011).
3) Follicular regression:
Follicle growth without ovulation during the breeding season is extremely rare but may occur.
➡️Diagnosis: For its diagnosis, ovarian activity should be followed throughout the breeding season by ultrasonography at least three times weekly. Multiple follicles less than 10 mm are present and, periodically, a follicle would grow to 18-20 mm and gradually regress.
➡️Treatment with an administration of prostaglandin (to lyse any luteal tissue) and hCG (at peak follicle growth) had no effects.
a- Uterine affections
1) Endometrial gland hypoplasia
Uterine hypoplasia (underdevelopment) is characterized by an inability of the uterus to develop adequately in order to maintain a pregnancy. The endometrial glands are those most significantly affected, tending to be very small and so incapable of adaptation to support a pregnancy. As a result, even if fertilization does occur, the early embryonic death rate is high. Covering mares
too close to puberty is associated with high rates of early embryonic death rate, due to hypoplasia, simply because the uterine development to date is inadequate. The actual age at which the uterus is fully mature depends very largely on the individual mare, 18 months to 4 years is considered acceptable. Hypoplasia at 4 years old or over is indicative of a problem, which is likely to be permanent and may be associated with chromosomal or hormonal abnormalities .
2) Bacterial endometritis
Endometritis, can be acute or chronic, is an inflammatory process of the uterus. It may be caused by non-pathological or pathological conditions. Infectious endometritis is one of the main obstacles limiting reproductive efficiency in horses. Mares with defective vulvar conformation can aspirate air and bacteria into the vagina, which can develop into endometritis. Mares can harbor the organisms in the vestibular area, particularly the clitoral fossa and sinuses and, at the time of mating or of gynecologic examination, may transfer the organisms into the uterus
The bacteria can gain access to the uterus as
(1) Contaminants and commensals.
(2) Opportunist, e.g., Streptococcus zooepidemicus (the most commonly isolated bacteria mainly in the initial stages), Escherichia coli (the next most common isolate), and Staphylococcus spp., causing acute endometritis.
(3) Venereally transmitted as the stallion’s penis is colonized by similar organisms. Three bacteria are venereally transmitted: Taylorella equigenitalis (contagious equine metritis organism), Klebsiella pneumoniae (capsular types 1, 2, and 5), and some strains of Pseudomonas aeruginosa.
➡️Classification of equine endometritis:
1. Acute infectious endometritis
2. Chronic infectious endometritis
3. Endometriosis (chronic degenerative endometritis)
4. Persistent mating-induced endometritis (also referred to as delayed uterine clearance)
➡️Diagnosis
1. A diagnosis of endometritis can be made by collection of concurrent endometrial swab and smear samples during early estrus for bacteriologic culture and cytologic examination, respectively.
\Methods:
1. A non-guarded endometrial swab on a sterile extension rod is carefully passed via a sterile speculum through the cervix into the uterine body and, after withdrawal, is placed in transport medium. A second swab culture is obtained immediately afterward for the endometrial smear.
2. A guarded swab is passed into the uterine lumen using a sterile speculum or enclosed in a disposable plastic armlength glove. The swab tip is exposed only when it is in the uterine lumen. A swab specimen for cytologic examination should again be obtained.
➡️Interpretation.
Diagnosis of acute endometritis is based on the presence or absence of significant numbers of neutrophils in the smear. Mares that have > five neutrophils per high-power field (×40) on a cytology smear should be considered to have active endometritis
N.B. A positive culture result, with no evidence of inflammatory cells in the smear (usually could be considered the result of a contaminant during collection.
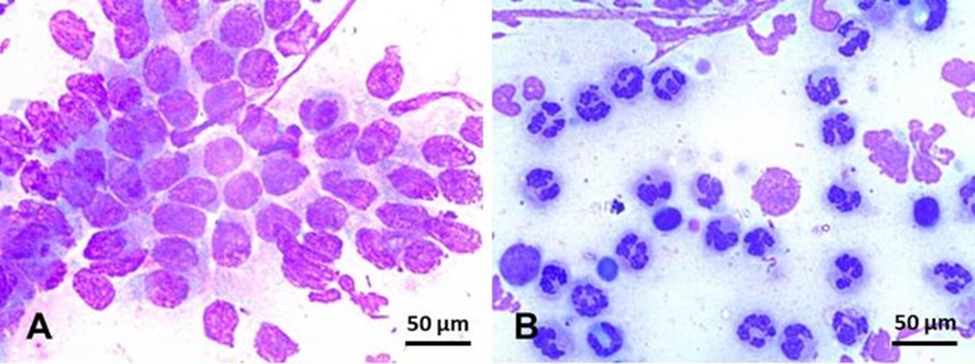
Fig. 3 Endometrial cytology in mares stained with Romanowsky-type stain (×100).
(A) Negative endometrial cytology; in this slide, endometrium epithelium cells, can be seen in the absence of inflammatory cells.
(B) Positive endometrial cytology; few endometrium epithelium cells can be seen in this slide, but, conversely, hyper-segmented neutrophils are overly represented in this smear. Scale bars 50 µm (A and B). Source: Canisso et al. (2020).
2. Endometrial Histology
In some cases, endometrial biopsy may be a useful diagnostic aid. The technique involves the insertion of a biopsy instrument (60–70 cm in length) through the cervix and into the uterus. With the biopsy instrument in the uterine lumen, a gloved hand is inserted into the rectum to allow manipulation of the instrument into the desired position. The sample is obtained by closing the jaws of the instrument and tugging sharply. To avoid damage, the tissue is carefully transferred into a fixative solution by dislodging it from the jaws of the punch with a fine hypodermic needle.
3. Uterine Luminal Fluid
Intraluminal uterine fluid can be graded I to IV according to the degree of echogenicity. The more echogenic the fluid, the more likely the fluid is contaminated with debris, including white blood cells. Ultrasonographic appearance may be proportional to the size and concentration of particulate matter within the fluid, rather than the viscosity of the fluid (e.g., purulent exudates can appear non-echogenic). Air has hyperechogenic foci, and fluid with air bubbles appears cellular. Urine in the bladder can appear echogenic, despite being a watery liquid
➡️Treatment
The approach to treatment is based on the infusion of various antibiotics (based on in vitro antibiotic sensitivity) suspended in water or saline, into the uterine lumen during estrus.
▪️ A buffered, water-soluble antibiotic combination dissolved in 30 ml (in young mares) or 80 ml (pluriparous mares) in of sterile water and then instilled through the cervix into the uterus via a sterile irrigation catheter is a sufficient volume to cover the entire endometrial surface in most mares.
▪️ The number of treatments required depends on individual circumstances, but daily infusions for 3–5 days during estrus works well in most cases. The success of this treatment can be monitored using ultrasonography to identify the presence of intrauterine fluid.
▪️ When antibiotics are combined with oxytocin, a single daily treatment for 3 days has been successful in many cases.
▪️ In addition to the antibiotic therapy, repeated treatment with PGF2α increases the frequency of the follicular phases, thus allowing intrauterine therapy to be used more readily. It also reduces the duration of the luteal phase when progesterone increases the susceptibility to infection.
▪️ Recently, immunomodulators (e.g., Propionibacterium acnes or a Mycobacterium cell wall extract) have been suggested as useful adjunct therapy in treatment of endometritis in the broodmare.
3) Pneumouterus
PNEUMOUTERUS is a predisposing factor for endometritis and suboptimal fertility in the mare
|
Vaginoscopic view of the relaxed cervix. Image source Livesey et al., 2015. |
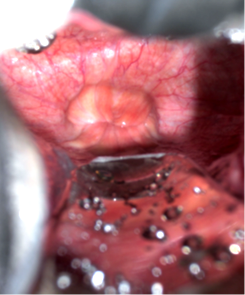
Cervix represents one of the most important internal closure and protection mechanisms. The tight closure of the cervix during the luteal phase and during pregnancy is essential for a successful breeding outcome in the mare. The cervix opens only during oestrous and at parturition. Mares with an incompetent cervix tend to have reproductive problems due to the entrance of microorganisms into the uterine lumen.
➡️Causes of cervical incompetency:
1. Uncommon Inadequate cervical closure that lead to a significant reduction of fertility, embryonic loss or even sterility.
2. Cervical hypoplasia that frequently be associated with ovarian hypoplasia. Mare showed a shortened cervix of 3 cm length associated with regular size and function of the other genitalia. The normal size of a cervix in mares of this breed should be 5–7.5 cm in length (moderate hypoplasia may cause functional incompetence of the cervix and supports uterine contamination and chronic endometritis and fertility problems).
3. Genital abnormalities that commonly associated with lacerations, which can occur during dystocia or even during an apparently uneventful delivery.
4. Pneumouterus after parturition
▪️ After parturition mare show failure to nurse*.
*Sufficient accumulation of air cause uterine distension and activate the stretch receptors in the uterine wall that delay nursing and uterine involution.
▪️ Started to show signs of abdominal pain (pawing, lying down, and looking at the abdomen) approximately six hours postpartum.
▪️ The mare has a slightly increased heart rate (50 bpm)
▪️ Sweating moderately.
▪️ Borborygmi were detected by auscultation of the abdomen.
5. Trauma during parturition was sufficient to result in temporary disruption of the functioning of the physical barriers, allowing an inrush of air into the non-involuted uterus which then became distended.
6. Aging and abnormal vulvar conformation (Long length of vulva above pelvic brim. Dorsal commissure of vulva drawn cranially with advancing age).
7. Excessive weight.
➡️Abdominal examination per rectum revealed:
▪️ The uterus to be distended and gas filled.
A ‘windsucking*’ noise could be detected as air entered the vestibule, even though the mare appeared to have normal external vulvar and perineal conformation, and no neurological deficits.
N:B *sound of air rushing into the vagina indicates that the vestibular fold is not properly separating the vagina from the environment. For windsucking to occur, three physical barriers must disrupt the vulvar seal, the vestibulovaginal sphincter and the cervix.
➡️During routine examination
An air-filled uterus was detected by trans-rectal palpation.
➡️Ultrasound
1) With ultrasound scanning no structure or contents were found in the air-filled corpus uteri due to acoustic extinctions, but hyperechoic reflections (hyperechoic particles between the endometrial folds) were visible in both uterine horns.
2) The mild endometritis - suboptimal fertility- of neutrophilic character, indicating only a mild reaction of the endometrium due to the influx of air.
3) Both ovaries were of normal size and displayed regular follicle development.
➡️Vaginal examination
After the mare’s perineum had been washed 3 times with a disinfectant soap, a Polanski speculum was introduced into the vagina.
▪️ The vaginal mucosa was pinkish, moderately damp, and there were no signs of injury.
▪️ The cervix had a diameter of 2 cm and was relaxed.
▪️ At certain times the cervical canal into the uterus could be seen without any manipulation.
➡️Differential diagnosis:
▪️ Mild colic in the immediate postpartum period is common, and is most often associated with the uterine contractions that occur during involution: signs of colic commonly resolve shortly after expulsion of the placenta.
▪️ Rupture of the middle uterine or utero-ovarian artery
▪️ Haematoma in the broad ligament
▪️ Haemorrhage directly into the abdomen
▪️ Haematoma in the uterine wall
▪️ Rupture of the internal pudendal artery or its branch or the vaginal artery, can also cause colic.
▪️ Uterine horn intussusception
▪️ Uterine rupture
▪️ Caecal impaction, caecal rupture, colon rupture small colon ischaemia, tearing of the mesentery of the small colon.
▪️ Diaphragmatic hernia, large colon displacements or torsions.
➡️Treatment
1) After perineum washing, a sterile nasogastric tube inserted through the cervix into the dilated uterus, and two towel clamps applied to the dorsal commissure of the vulvar lips to create a partial seal. A stomach pump was attached to the nasogastric tube and air was evacuated from the uterus.
2) Caslick's operation if the cause abnormal vulvar or vaginal configuration.
➡️Cost considerations
- Decreased fertility with repeated diagnostic/reproductive system/examinations.
- Requires repeated surgery, both to re-do the anatomical defect, and to reverse that correction before foaling (Caslick’s procedure).
4) Uterine luminal or endometrial cysts
Uterine luminal or endometrial cysts are the most common form of uterine lesion (Eilts et al., 1995). They are generally thin-walled, greater than 3 cm in diameter and filled with lymph and may occur singly or in multiples. They are particularly evident in mares of 10 years old or over. Their effect on reproductive performance is disputed. If they are present in any number, they are likely to interfere with embryonic mobility, increasing EED (McDowell et al., 1988), and also to reduce the uterine surface area available for placental attachment, increasing abortion rates (Curnow, 1991).
➡️Treatment may be attempted by puncturing the cysts via curettage, endoscopic manipulation or thermocautery, though they may subsequently recur (Pycock, 2000).
5) Transluminal adhesion
Mare’s pyometra commonly accompanied with occlusion of the cervical lumen - (Mare’s cervix is very susceptible to damage and formation of adhesions) - due to formation of excessive transluminal adhesions, tortuosity and cicatrices that inhibits not only the natural evacuation of the uterine contents; but also it prevents the therapeutic drainage.
Causes
▪️ Traumatic lacerations during parturition.
▪️ Dystocia.
▪️ Repeated cervical manipulation during the intrauterine therapy, artificial insemination and embryo transfer.
▪️ Distorted cervical anatomy
All of these preceding factors increasing risk of pyometra development due to mechanical impairment of uterine clearance mechanisms so dilating the cervix enable the uterine lavage and intra-uterine therapy.
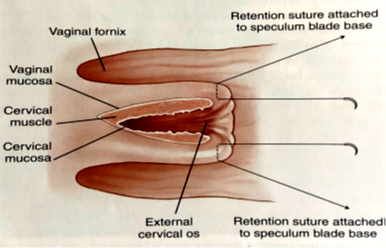
➡️Treatment: Modified Cervical wedge resection (Brinsko, 2023)
|

|
|
Cervical wedge resection. (Modified from Brinsko SP, et al.: Manual of Equine Reproduction, Third Edition, Maryland Heights, MO, Mosby, Inc/Elsevier, 2010). Image source Brinsko (2023). |
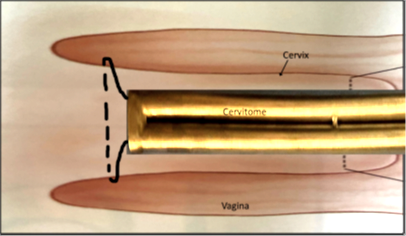
“Cervitomes” used for amputation of the mare’s cervix. The instrument above the ruler is a pair of stainless-steel tubes that were taped together for the first application of this procedure. The instrument below the ruler used for subsequent procedures was fabricated with a hardened head to mimic the Utrecht model fetotome. Image source Brinsko (2023). |
|
|
|
Placement of “cervitome” firmly against the mare’s cervix with wire looped around the cervix for amputation. (Modified from Brinsko SP, et al.: Manual of Equine Reproduction, Third Edition, Maryland Heights, MO, Mosby, Inc/Elsevier, 2010). Image source Brinsko (2023). |
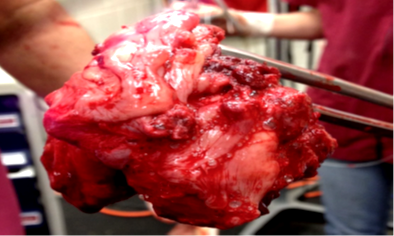
Grossly abnormal cervical tissue removed with Vulsellum forceps after amputation. Image source Brinsko (2023). |

|
|
|
View of cervical stump, immediately after amputation. Note that there is minimal hemorrhage. Image source Brinsko (2023). |
|
6) Abscesses
➡️Ovarian abscess in mare
|
|
|
|
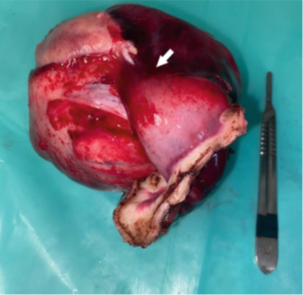
Macroscopic image of the left ovary after surgery. Gross examination revealed (A) adhesion of the uterine horn to the surface of the ovary (arrow) and next to this area the ovary showed a haemorrhagic region. (B) The ovary has small follicles (arrowheads) and (C) two foci of chronic apostematous oophoritis (arrows). Image source Fernández-Hernández et al., 2023 |
||
Primary abscessation
in mares is uncommon
▪️ Most commonly come in unilateral
form.
▪️ Ascending infection from the uterus to the oviduct and ovary is rare in the mare because of the presence of the oviductal papilla.
➡️Causes
Potential complication of OPU
➡️Symptoms
1) lack of appetite
2) Pyrexia
3) Weak intermittent colic
4) Colic and pyrexia tend to be associated with gastrointestinal distress.
5) In some cases after OPU mare show tachypnoea, tachycardia.
6) Lameness and with frequent lateral recumbency.
➡️Hematological finding
1) Mare had hyperfibrinogenemia
2) Neutrophilia
3) Globulinemia
4) Slight increase in serum amyloid
➡️Diagnosis
▪️ Ultrasonographic evaluation of the reproductive tract determined the mare had poor perineal conformation.
▪️ Pneumouterus
▪️ Enlarged right or left ovary with fluid-filled cavities (~5 and 6 cm in diameter).
▪️ Histopathologic evaluation usually reveals an ovulatory hemorrhagic follicle with an adjacent ovarian abscess.
▪️ Ovariocentesis resulting in hematogenous spread of bacteria, or migration of strongyle larva.
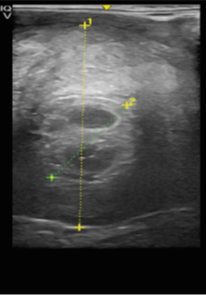
➡️Ultrasonographic diagnosis
▪️ Well delimited structures of approximately 2-6 cm, enclosed within a hyperechoic wall. The structures were surrounded by heterogenous ovarian stroma and contained a trabecular pattern in combination with more organized areas in the same ovary. The right ovary was normal on palpation and ultrasound.

|
|
|
Transrectal ultrasonographic images of left ovary of a pony mare showing two circumscribed structures of approximately 2 × 2 cm, enclosed by a hyperechoic wall, surrounded by heterogenous ovarian stroma and containing a trabecular pattern. |
|
|
|
|
Transrectal ultrasonographic images of left ovary. Ultrasonography shows an enlarged left ovary (9.9 cm) and two well defined structures (4.28 cm), enclosed by a hyperechoic wall (arrow), surrounded by heterogenous ovarian stroma, a fibrous aspect (3 cm) and (B) containing focal hyperechoic areas (arrowhead) encircled by echogenic and homogenous content. Images source Fernández-Hernández et al., 2023 |
|
|
|
|
Transabdominal ultrasonography and abdominocentesis:
▪️ Identified an increased amount of orange-opaque peritoneal fluid (923,000 WBC/μL [85% neutrophils]).
▪️ The purulent content produced a massive growth of β-haemolytic Streptococcus equi subsp. Zooepidemicus sensitive to several antibiotics including doxycycline, penicillin and gentamicin.
➡️The differential diagnosis:
“Enlarged” ovary in the mare includes neoplasia, hematoma, transitional ovary, and abscess, (Ovarian abscess is usually uncommon) but usually tends to be associated with a fever of unknown origin and colic.
➡️Rectal diagnosis
▪️ Ovarian abscesses may result from rough handling of the ovary
▪️ Hard non-painful structure could be felt in the left lateral and ventral side of the abdomen.
➡️Treatment
▪️ Initial treatment included antibiotics (trimethoprim-sulfadiazine 30 mg/kg po q12h) for 6 day
▪️ Doxycycline (30 mg/kg po q 12h).
▪️ Anti-inflammatory flunixin meglumine (Flunixin 50 mg/mL; 1.1 mg/kg for 3 days followed 0.5 mg/kg, po, q12h)
▪️ Anti-ulcer medication.
➡️Some cases need surgery
Dissection and secure haemostasis of the mesovarium was achieved using a vessel-sealing system .
▪️ On surgery macroscopic examination of the ovary revealed adhesion of the uterine horn to the surface of the ovary (10 × 10 cm) and close to this area the ovary presented a hemorrhagic region. On macroscopic evaluation, the ovary exhibited small follicles and two foci of chronic apostematous oophoritis.
▪️ For 10 days later after surgery the perioperative treatment consisted of sodium benzyl penicillin (22 000 ui/kg IV q 6h) with gentamicin (6.6 mg/kg, IV, q 24h) and anti-inflammatory therapy (Flunixin Injectable 50 mg/mL; 1.1 mg/kg, IV, q 12h).
▪️ An intensive monitoring plan was established based on general physical examination every 3 h.
▪️ After treatment, the reproductive ultrasonographic exam and hematological evaluation should be return to normal to return mare to the herd.
➡️Postoperative complications:
Incisional infection and peritonitis that treated with incisional and peritoneal drainage and lavage with isotonic saline solution, anti-inflammatory and broad-spectrum antibiotics
refer
7) Neoplasms
▪️ Solid masses in the uterus may be tumors, or intramural hematoma formation. Intramural hematomas form as a foaling injury, and slowly resolve over time.
▪️ The most common uterine tumor is comprise of smooth muscle and is called a leiomyoma.
➡️Leiomyomas:
Are usually first detected using trans-rectal ultrasound examination; they are slow growing, range in size from 2-5cm, and may be pedunculated. As the tumor enlarges it may obstruct the uterine lumen, become necrotic on the surface as it outgrows its blood supply, and subsequently interferes with fertility.
The etiology of Leiomyomas in animals is not fully elucidated, but some studies suggest the influence of oestradiol and progesterone on tumorigenesis. In the mare of the present case, there was no indication of any hormonal imbalance, as evidenced by her normal reproductive cycles.
➡️Uterine adenocarcinomas
Have also been reported and result in significant tissue damage, and uterine discharge.
➡️Lymphosarcoma and melanoma may also metastasize to the uterus.
➡️Oviductal neoplasia (adenoma)
➡️Diagnosis
On trans-rectal ultrasonography, an echogenic mass was detected in the uterine lumen
➡️Differential diagnosis:
1. Large endometrial cyst
2. Abscess
3. Intramural hematoma
The persistence and the gradual enlargement of the mass rule out an intramural hematoma, since the size diminishes, and the ultrasonographic appearance of hematoma characteristically changes over a period of a few months
4. Fibroses (scar tissue)
Neoplasia is generally a disease of older animals
|
Uterus in vivo. Hysteroscopic view of a leiomyoma of in the middle third of the left uterine horn of the 17-year-old Selle Français mare. Image source Nelis et al., 2013 |

Treatment
Benign masses which interfere with fertility may be removed surgically. Malignant neoplasia is usually not treated since the prognosis is generally poor.
Mare must have 70% of her uterus remaining following surgical removal of the tumor for successful pregnancy.
