
كتاب
INFERTILITY IN PET ANIMALS
- Reproductive problems of bitches and queens
Female reproductive physiology and endocrinology in dogs and cats have become relatively well understood. As a result, we now have a better understanding of reproductive disorders which may be produced from pathological abnormalities in the reproductive system.
1. Ovarian problems
A. Ovarian cysts:
1. Follicular cysts (Estrogen producing cysts):
⮚ Occurs in older bitches and queens, especially in females who have never delivered a litter.
⮚ These cysts are formed from the failure of ovulation.
⮚ Should be distinguished from other cysts that grow from or inside the ovaries or adjacent ductal remnants, such as cystic rete ovarii, subsurface epithelial structures, and paraovarian cysts.
Diagnosis:
Clinical symptoms:
1. Prolonged or irregular proestrus/estrus.
2. Vulvar swelling and hemorrhagic vulvar discharge.
3. Irregular interestrus interval.
4. Infertility.
Hormone assays
● Increased serum estrogen concentration.
● Prolonged exposure of the endometrium to elevated estrogen concentrations may induce cystic endometrial hyperplasia-pyometra complex.
Vaginal cytology: changes associated with high estrogen levels.
D. Ultrasonography
The ultrasound examination reveals the presence of single or multiple hypoechoic to anechoic large follicles (> 1cm in diameter) (Fig. 9).
The diameter of the single cyst ranges from 1 to 5 cm, while the diameter of multiple cysts can be up to 10 cm in bitches.
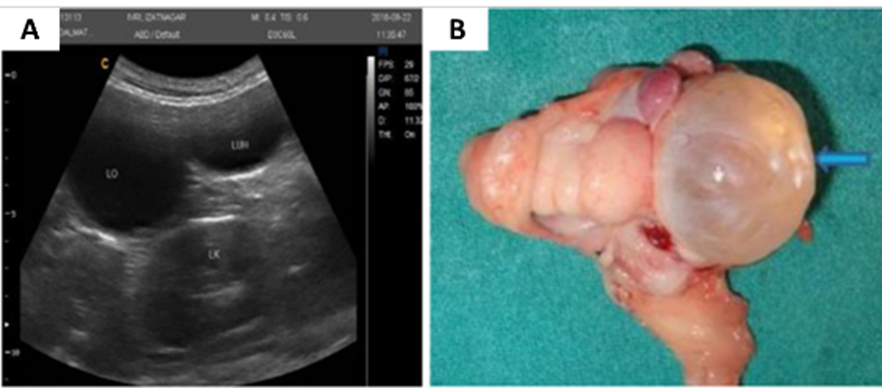
Fig. 8: Representative ultrasonography images showing cystic ovary (A) and gross photographs showing follicular cysts in the ovary (blue arrow) (B) (Sasidharan et al., 2021).
Treatment:
1. Induction of ovulation by using human chorionic gonadotropin or gonadotropin-releasing hormones can be used but with less success.
● Human chorionic gonadotropin for treatment of ovarian cysts (220 IU/Kg IV once or 500 IU, IM, two doses with 48-hour interval).
● GnRH for treatment of follicular cysts (50 µg, IM).
● LH for treatment of follicular cysts (50 mg IM).
2. Ovariohysterectomy is the treatment of choice for ovarian cysts.
2. Lutein cyst and cystic corpus luteum (Progesterone producing cysts):
● Lutein cysts are lined with luteal tissue and have thicker and opaque walls.
● It is believed that luteinized cysts originate from follicular cysts after granulosa cells have undergone complete or partial luteinization.
● They produce progesterone in low concentrations for a prolonged period.
● lutein cysts are ranging from 1.5 to 3.0 cm in diameter.
The normal corpus luteum in the dog shows central cavitation for a short time after ovulation. A persistent fluid-filled cavity may indicate an incomplete luteinization and therefore is defined as cystic corpus luteum. It is believed that this condition has no clinical significance.
● Treatment of lutein cysts: serial PGF2α administration (0.25 mg/kg) or ovariectomy has been suggested.
3. Cystic rete ovarii:
● These cysts originate from a dilatation of the rete tubules and are lined by a single cuboidal epithelium. The rete ovarii tubules are remnants from embryologic structures and are located in the medulla at the hilus of the ovary.
● Cystic rete ovarii occur in up to 10% of older dogs and these cysts do not produce hormones.
Treatment: If they become large, they should be surgically removed because they may compress the ovarian stroma.
4. Cysts of subsurface epithelial structures (SES):
✔ They arise from the ovarian surface and also be termed as germinal cysts.
✔ Cysts are rarely larger than 5 mm and lined with non-secretory cuboidal or low columnar epithelium.
✔ They are often microscopic in size, multiple in numbers and commonly bilateral.
✔ The SES cysts grow at the surface, typically enlarging the size of the ovary.
Diagnosis:
● Palpation of the caudal pole of the kidney reveals the presence of the swollen ovaries as relatively solid ovoid masses.
● During transabdominal palpation, the dogs occasionally show signs of abdominal distress.
● The cysts of SES are immunoreactive to placental alkaline phosphatase and placental alkaline phosphatase that can serve as a histological marker of SES cyst.
These cysts are usually found by coincidence in older dogs and have no clinical relevance.
5. Extraovarian cysts(GCT):
● Extraovarian cysts originate from the embryonic remains of the paramesonephric duct (Muellerian duct), mesonephric duct (Wolffian duct) or mesonephric tubule.
● These cysts have a smooth muscle wall that distinguishes them from rete tubules
● Usually, these cysts have no clinical relevance.
B. Ovarian tumor
1. Granulosa cell tumor
Common ovarian in bitches, rarely observed in cats (Fig. 10).
Diagnosis:
1. Clinical signs including enlarged abdomen.
2. Clinical manifestations of hormonal disturbance.
3. Abdominal palpation (reveals the presence of intraabdominal mass).
4. Estradiol assay: high estrogen level.
5. Ultrasound.

Fig. 9: Granulosa cell tumor (GCT) in bitch ( Horner er al., 2024)
2. Other ovarian tumors: include fibroadenoma, fibroma, carcinoma, and teratomas.
Treatment: Ovariectomy is the treatment of choice in ovarian tumors.
C. Ovarian remnant syndrome:
● Ovarian remnant syndrome refers to clinical signs indicating the presence of functional ovarian tissue in a previously ovariohysterectomized female dog.
● Ovarian remnant syndrome occurs when a retained piece of ovarian tissue revascularizes and becomes functional.
Clinical signs:
● Dogs with ovarian remnant syndrome exhibit physical changes characteristic of proestrus and estrus, with vulvar swelling.
● Variable amounts of mucoid to serosanguinous vulvar discharge.
● Behavioral signs of estrus, such as tail flagging and attracting and stand to be mounted by male dogs.
Diagnosis:
✔ Presumptive diagnosis of ovarian remnant syndrome requires demonstration of flown vaginal epithelial specimen bitch. The vaginal cytology specimen should be collected when the bitch is in estrus, defined by behavioral changes noted by the owner and physical changes characteristic of proestrus.
✔ Total or predominant cornification of vaginal epithelial cells is indicative of elevated serum estrogen concentration.
✔ Exploratory laparotomy is the treatment of choice.
✔ Lifelong medical therapy with estrus-suppressing drugs, such as megestrol acetate or mibolerone but not a safe method.
2. Uterine problems
A. Cystic endometrial hyperplasia-Pyometra complex
● Pyometra in bitches and queens is a serious problem that affects their life.
● The incidence of pyometra is lower in queens than bitches since they are an induced ovulator.
● Pyometra raises in bitches > 4 years of age and queens > 5 years due to repeated estrous cycles without pregnancy with changes occurring in the uterine wall under progesterone effect.
Diagnosis:
1. History: History of middle-aged animals as well as usage of estrogen and progesterone drugs for estrus suppression, estrus induction, pregnancy termination, and contraception.
2. Clinical signs: Several signs are observed in cases of pyometra including:
● Vulvar discharge (in opened pyometra).
● The vulvar discharge is mucoid to purulent usually of foul smell (Fig. 11).
● The color of the vulvar discharges varies from yellow to light chocolate-brown.
● Fever, anorexia, weight loss, depression.
● Vomiting, diarrhea, abdominal distention.
● Polydipsia and polyuria.
● Animals with open cervix pyometra are less systemically ill compared to those with closed cervix.
⮚ The presence of fever in pyometra may be attributed to septicemia and toxemia which causes anorexia and depression.
⮚ Abdominal distention was a marked sign observed in all cases suffered from pyometra due to fluid accumulation in the uterus.
⮚ Polyuria and polydipsia may be attributed to endotoxins release following bacterial invasion which interfere with renal sodium and chloride absorption leading to water absorption impairment. E. coli endotoxins also block receptors of antidiuretic hormone on the collecting ducts, leading to obligatory polyuria with compensatory polydipsia.

Fig. 11: Clinical symptoms of pyometra.
Vomiting (curved arrow) and purulent vulvar discharge (notched arrow) in
pit-bull bitch suffering from pyometra (Abdel-Daym et al., 2022).
3. Abdominal ultrasonography:
The uterus of bitches and
queens suffering from pyometra is characterized by an accumulation of anechoic
to hypoechoic fluid (uterine exudates or pus) with a significant increase in uterine wall
thickness (Fig. 12).
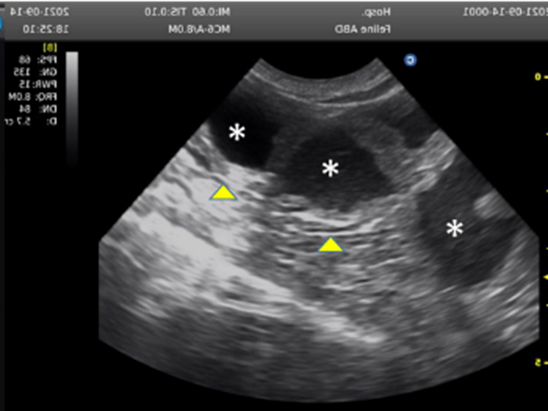
Fig. 12: Ultrasound images of queen uterus showed pyometra. Note the presence of an accumulation of slightly echogenic inflammatory fluid (*) inside the uterine lumen in association with the thickening of the uterine wall (arrow heads) (Abdel-Daym et al., 2022).
Treatment:
1. Surgical therapy: Ovariohysterectomy is the treatment of choice especially in closed pyometra (Fig. 13).

Fig. 13: Enlarged queen uterus during ovariohysterectomy (taken in the clinic of pet animals, Fac. Vet. Med., Cairo University).
2. Medical treatment:
● Used for opened pyometra.
● When animals are not systemically ill.
● In bitches of breeding age.
The medical treatment includes:
a. PGF2 α
● Only the naturally occurring PGF2α should be used.
● PGF2α that induces luteolysis, increases myometrial contractility, promotes expulsion of uterine contents, and may enhance cervical dilatation.
● The dose of PGF2 is 0.25 mg/kg (250 µg/kg) once daily SC for 5 days.
2. progesterone antagonist, progesterone-receptor blocker with or without PGF2α can be used.
● Dose of progesterone antagonist
- 10 mg/kg SC, repeated after 24 hours for Treatment of Unwanted Mating and Pregnancy termination (up to day 45)
- 10 mg/kg SC on days 1, 2, and 7; additional doses on days 14 and 21 if needed for pyometra.
- 10 mg/kg SC on days 1, 2, 8, 15, 28, and 35 for Benign vaginal tumors.
- NB: progesterone antagonist alone can be effective and safe for the treatment of metritis and to induce cervical opening in closed pyometra. The association of progesterone antagonist progesterone antagonist and PGF2α was effective in the medical treatment for open and closed pyometra. Nevertheless, careful case selection is important, and medical treatment is contraindicated in bitches with hepatorenal failure or peritonitis; clinical parameters should be monitored closely throughout treatment.
3. Oxytocin: can be used to stimulate activity of the uterine smooth muscle (10 IU in bitch and 5 IU in queen).
4. Broad spectrum antibiotic is used until vaginal swab for bacteriology and sensitivity test (Minocycline (25 mg/kg per os [PO] once daily for 14 days) with dihydrostreptomycin (5 mg/kg IM twice daily for 7 days), or Tetracycline (30 mg/kg PO twice daily for 21 days) with streptomycin (20 mg/kg IM once daily for 14 days).
B. Metritis
Is an acute uterine inflammation that affects the mucosal and myometrial layers and occurs during the first week after delivery. Metritis is mostly associated with obstetric manipulation, abortion, dystocia, retained dead fetuses, or retained placenta. Nevertheless, it occurs in some cases associated with natural mating or artificial insemination. Escherichia coli and Proteus are the most commonly isolated bacteria from metritis patients. Diagnosis is based on clinical signs including fever, anorexia, lethargy, decreased milk production, and foul-smelling purulent vulvar discharges, and is confirmed by ultrasonography and radiography. Systemic therapy, either alone or in combination with PGF2α, has frequently had beneficial effects. Ovariohysterectomy is the last choice in complicated cases.
C. Endometritis
Is a chronic subclinical infection of the endometrium that must be distinguished from an acute postpartum infection. In queens it is more difficult to diagnose than a bitch. Infertility (mating with a fertile male at least three times without conception) could suggest a uterine infection. Treatment is successful with broad-spectrum antibiotic or using Aglepristone together with antibiotics for 15 days.
3. Cervical problems: cervical affections that lead to infertility are uncommon, only recorded as a case of cervical sarcoma in Labrador bitch of 1.5 years and manifested by cervical hemorrhage.
4. Vaginal problems
A. Vaginal septum:
Vaginal septum is a congenital abnormality occurs in some bitches characterized by persistence of a vertical septum in the vagina that cause mild to severe clinical signs including recurrent vaginitis, dysuria, urinary dysfunction, difficulty in natural breeding and dystocia.
B. Vaginal hyperplasia
Vaginal hyperplasia is mostly a hereditary problem that occurs during the proestrus, estrus, or at the end of pregnancy due to estradiol levels increasing.
This condition is often referred to as vaginal prolapse, vaginal protrusion, vaginal hypertrophy, and estrual hypertrophy (Fig. 14).
Clinical signs:
1. Vaginal wall protrusion from vulva.
2. Vulvar discharge may present and may have vaginitis.
3. Dysuria may occur.
4. This disorder mostly prevents the male penis from introducing into the female genital tract so affected bitches require artificial insemination.
Differential diagnosis
● Vaginal hyperplasia may be confused with vaginal neoplasia.
● Differentiated by history of proestrus, high estrogen level, tissue histopathology.
Treatment
⮚ It includes either decreasing estrogen stimulus in the animal, removing the prolapsed tissue, or both.
⮚ Even after surgical removal, it is usually recurrent in the same female so ovariectomy prevents recurrence.
⮚ Using topical antibiotics and anti-inflammatories if superficial inflammation or infection is present.
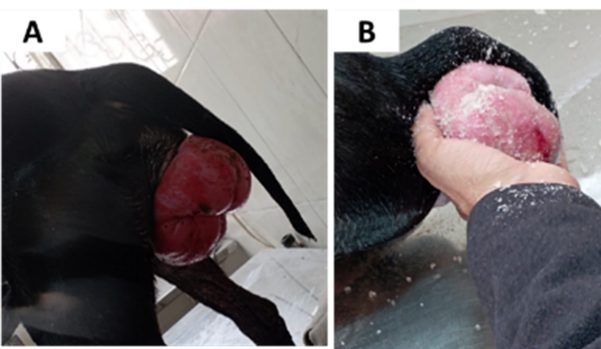
Fig. 14: Vaginal hyperplasia in black Rottweiler bitch (taken in the clinic of pet animals, Fac. Vet. Med., Benha University).
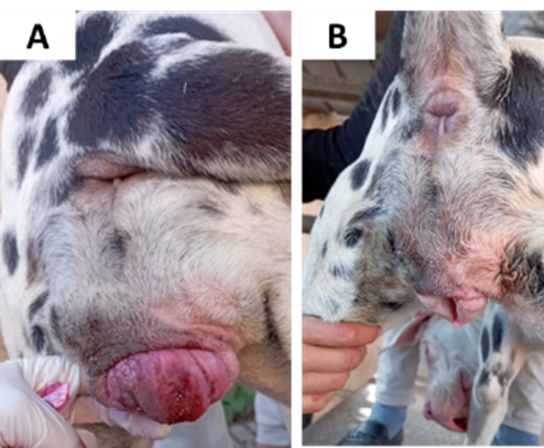
Fig. 15: Vaginal
hyperplasia in bitch before (A) and after (B) treatment (taken in the clinic of
pet animals, Fac. Vet. Med., Benha University).
C. Vaginal prolapse: is rare in queens.
D. Transmissible venereal tumor
● Transmissible venereal tumor (TVT) is the most common vaginal tumor in bitches that is mostly transmitted during sexual intercourse between males and females.
● TVTs are cauliflower-like, pedunculated, nodular, papillary, or multilobulated in appearance (Fig. 16).
● Viable CTVT cells can be transmitted to susceptible animals spontaneously through injured skin or mucosa during coitus, licking, fighting/ biting, sniffing, or scratching.
● Primarily located in the mucous membrane of the external genitalia of either sex.
● In addition to the genital system CTVT can occur anywhere on the body including the skin, oral and nasal cavities, conjunctiva, and even the anal mucosa.
Diagnosis
● Is based on physical examination that revealed large pedunculated cauliflower-like growths at the vagina which are firm in consistency and is confirmed with histopathology or cytology.
● Cytological examination revealed uniform round cells containing light-colored cytoplasm with multiple vacuoles and large nucleus and a prominent, centrally located nucleolus (Fig. 17).
Treatment
The most successful
treatment is chemotherapy applied with Vincristine 0.025 mg/kg b. wt. slow IV
once a week for 4 weeks along with supportive treatment.
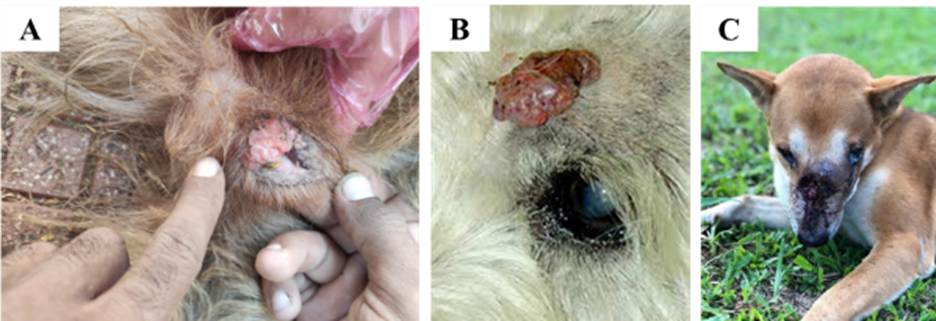
Fig. 16: different sites of TVT growth in bitches. A: vaginal TVT, B: skin TVT, C: nasal TVT.
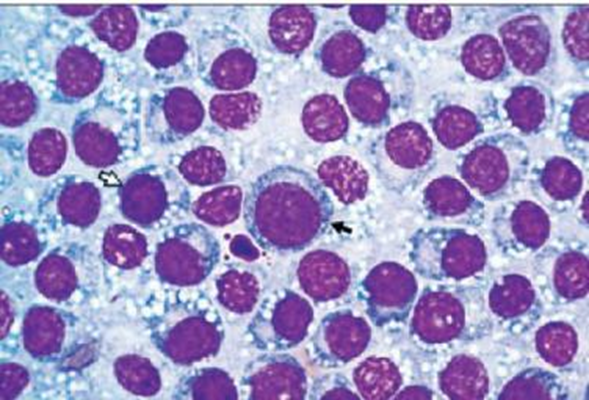
Fig. 17: Cytological examination of canine TVT revealed uniform round cells containing light-colored cytoplasm with multiple vacuoles and large nucleus and a prominent, central-located nucleolus (Flórez et al., 2012).
E. Canine Brucellosis
● Canine brucellosis is an infectious disease caused by the bacteria Brucella canis, a gram-negative, non-motile aerobic intracellular coccobacillus.
● B. canis is the most common Brucella species found in infected dogs.
● B. canis is a significant cause of reproductive failure in dogs.
● Incidence is higher in stray dogs than in pets.
● Canine brucellosis is a public health concern, as it is a zoonotic disease.
Transmission
● B. canis organisms are shed in urine, vaginal discharge, semen, aborted material (this contains the highest concentration of organisms), milk, nasal secretions, and saliva.
● Transmission usually occurs via ingestion of contaminated materials or when mucous membranes come in contact with vaginal discharge from an infected bitch during mating.
● It may also be transmitted to the female via infected semen.
● Puppies can become infected in utero or during nursing.
● The organs most commonly infected in male dogs are the testes and epididymis, causing signs of orchitis/epididymitis, scrotal dermatitis, oligozoospermia, and infertility.
● The organism can be recovered from the testes and epididymes within 5 weeks of experimental infection" Epididymitis alone occurs more commonly than orchitis or orchitis/epididymitis”.
Clinical Signs
● The most common clinical signs associated with canine brucellosis are late-term abortion, stillborn puppies, infertility, lethargy, and lymphadenopathy.
● Live puppies may be born to an infected bitch, but they may die within a few hours or days.
● Advanced cases may present with testicular atrophy. Another manifestation of canine brucellosis is discospondylitis (with associated anorexia, weight loss, pain, lameness, ataxia, and muscle weakness).
Clinical Signs in male
● Male dogs may have enlarged testicles and scrotal edema.
● Testicular atrophy associated with teratozoospermia, sperm agglutination due to the formation of antisperm antibodies, and eventual spermatogenic arrest may occur in chronic infections.
● Advanced cases may present with testicular atrophy.
● The incidence of discospondylitis is higher in male than female dogs. Ocular signs include uveitis, corneal edema, and optic neuritis.
Diagnosis:
✔ Culture of Brucella canis from blood, lymph node, bone marrow, or infected tissues or discharges.
✔ Blood culture is the most accurate test available in the first 8 weeks following infection.
✔ Agglutination tests identify the presence of antibodies to cell wall antigens of Brucella canis.
✔ A rapid card agglutination test (RCAT; card test) and tube agglutination test (TAT; tube test) are commercially available.
✔ The RCAT gives a positive/negative result while the TAT yields a titer. A titer of greater than 1:200 is considered a positive result.
✔ Agglutination tests remain positive in infected animals from 8 to 12 weeks following infection to 3 months after the animal becomes abacteremic.
✔ The most accurate serologic test currently available is the agar gel immunodiffusion test (AGID) available through Cornell University as this test identifies antibodies to cytoplasmic antigens of Brucella canis, which are very specific to the Brucella sp.
✔ AGID tests are positive in infected animals from 12 weeks following infection to 36 months after the animal becomes abacteremic.
Treatment
✔ Pet animals that are housed singly may be neutered and treated with antibiotics to decrease bacteremia and subsequent shedding of the organism.
✔ Antibiotic regimens (Tetracycline derivatives):
● Minocycline (25 mg/kg per os [PO] once daily for 14 days) with dihydrostreptomycin (5 mg/kg IM twice daily for 7 days).
● Tetracycline (30 mg/kg PO twice daily for 21 days) with streptomycin (20 mg/kg IM once daily for 14 days).
Control of Brucella canis in a kennel
1. Confirm disease.
2. Quarantine kennel (no animals allowed in or out).
3. Determine source of infection (the index case is not necessarily the source of infection).
4. Eliminate the mode of transmission within the kennel.
5. Identify and cull infected animals.
6. Initiate practices to prevent further outbreaks.
7. Kennels should be considered clear of disease only when all animals have tested negative for 3 consecutive months. In closed kennels.
8. Complete eradication of the disease may require 5 to 7 months of testing and culling.
9. In open kennels, the disease may never be eradicated.
