
كتاب
Pediatric Intravenous Fluid Therapy
- Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
Steps of implementing Pediatric Intravenous Fluid Therapy strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
3.Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
· Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
Evidence to Decision Tables: (if any)
Guideline Implementation Tools
Educational materials based on this Adapted CPG for Pediatric Intravenous Fluid Therapy have been made available in several forms including:
1. Manual for physician for diagnosis and algorithm for Pediatric Intravenous Fluid Therapy
2. Arabic Educational materials for nurses and mothers
Table 3: Normal maintenance fluids by weight
|
Weight (Kg) |
BSA (m2) |
24h maintenance (mL) (a)(b) |
Maintenance rate (ml/h) (a)(c)(d) |
||
|
3 |
0.2 |
300 |
300 |
13 |
13 |
|
4 |
0.24 |
370 |
400 |
15 |
17 |
|
5 |
0.28 |
430 |
500 |
18 |
21 |
|
6 |
0.32 |
480 |
600 |
20 |
25 |
|
7 |
0.36 |
540 |
700 |
23 |
29 |
|
8 |
0.4 |
600 |
800 |
25 |
33 |
|
9 |
0.43 |
650 |
900 |
27 |
38 |
|
10 |
0.47 |
710 |
1000 |
29 |
42 |
|
12 |
0.54 |
810 |
1100 |
34 |
46 |
|
14 |
0.61 |
910 |
1200 |
38 |
50 |
|
16 |
0.67 |
1000 |
1300 |
42 |
54 |
|
18 |
0.73 |
1100 |
1400 |
46 |
58 |
|
20 |
0.79 |
1200 |
1500 |
49 |
63 |
|
25 |
0.93 |
1400 |
1600 |
58 |
67 |
|
30 |
1.06 |
1600 |
1700 |
66 |
71 |
|
35 |
1.18 |
1800 |
1800 |
74 |
75 |
|
40 |
1.28 |
1900 |
1900 |
80 |
79 |
|
45 |
1.39 |
2100 |
2000 |
87 |
83 |
|
50 |
1.48 |
2200 |
2100 |
92 |
88 |
|
60 |
1.65 |
2400 |
2300 |
100 |
96 |
|
70(e) |
1.79 |
2400 |
2400 |
100 |
100 |
* Not considering weight losses due to dehydration, extra weight associated with obesity or oedema
(a) based on Holliday and Segar formula (the right hand column) and 1500mL/m2 BSA (the left hand column)
(b) values up to 1000mL/24h are rounded to 10mL increments and values >1000mL/24 to 100mL increments
(c) all rates are rounded to whole numbers (mL/h)
(d) all rates express TOTAL NORMAL MAINTENANCE. Deductions based on a restricted regimen or fluid contents of feeds, medications, etc. have NOT been considered
(e) based on adult requirement of 100mL/h
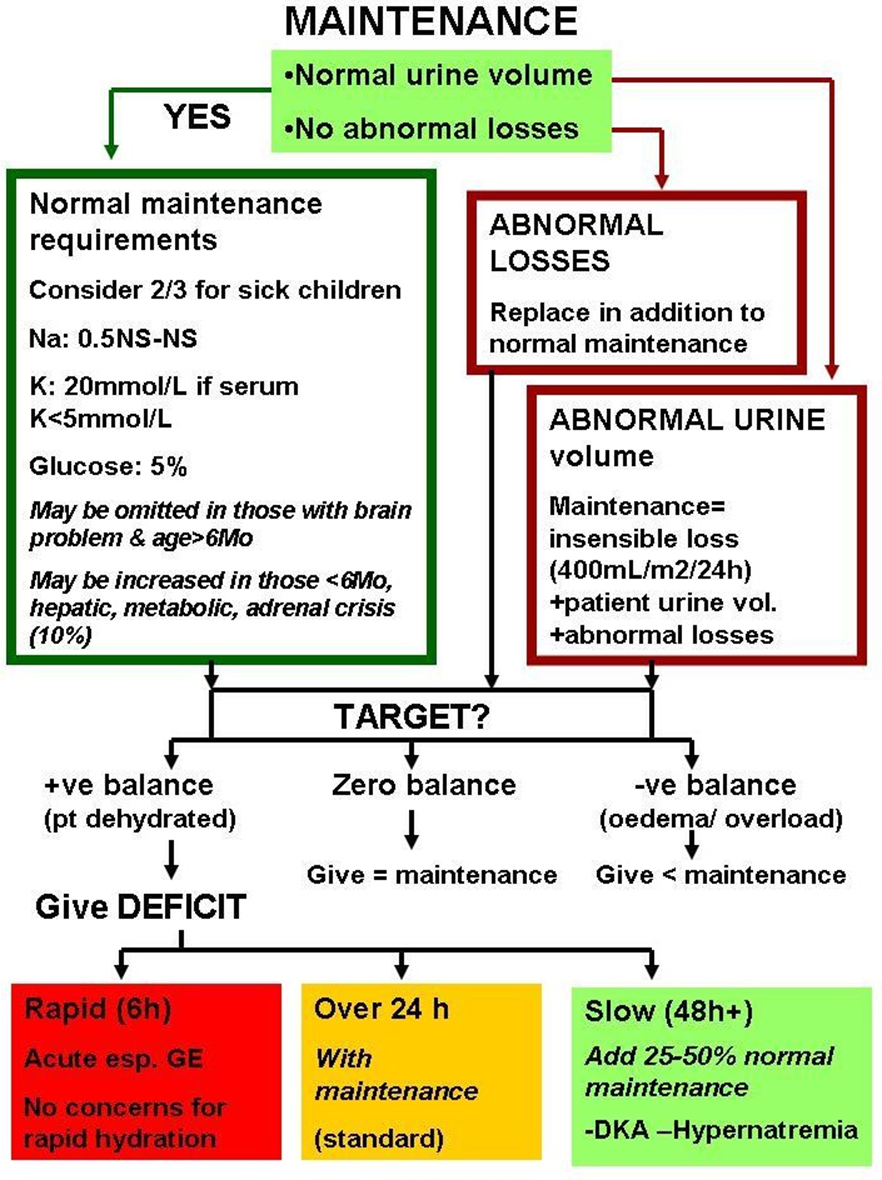
Figure 1: Maintenance & deficit plans chart
Table 4: Types of fluids & mixtures by sodium content (34)
|
|
Na (mEq/L) |
Examples |
Glucose & K content |
|
Isotonic |
±150 |
Normal saline Ringer & lactated Ringer (Na slightly less) |
None K (4-5 mEq/L) in ringer & LR |
|
3/4 NS |
±110 |
Glucose: saline 1:3 |
1/4th source glucose (2.5% if using 10%), No K |
|
|
80-90 |
IV rehydration premixed solutions |
Glucose <5% K varies by brand (8-30mEq/L) |
|
½ NS |
77 |
Glucose: saline 1:1 Half normal saline |
½ source glucose (5% if using 10%, 2.5% if 5%), No K |
|
1/3 NS |
±50 |
Glucose: saline 2:1 Glucose: ½ NS 1:2 1:19 bicarb: glucose (25mL/500) 1:16 bicarb: glucose (30mL/500) |
No K. Using 5%, final glucose: 3.3% (6.7% with 10%) 1.7% 5% 5% & higher Na (60mEq/L) |
|
0.2NS |
±30 |
Glucose 10%: saline 4:1 Glucose 10%: 25%: saline 3:1:1 Commercial maintenance solutions |
8%, No K 11%, No K 10-12%, K 10-20mEq/L |
|
|
0 |
Glucose (all conc.) |
|
Glucose 25% can be used to increase final mixture glucose concentration. To increase K by 20 mEq/L add 5mL KCl per 500 mL, or 1 mL/100mL
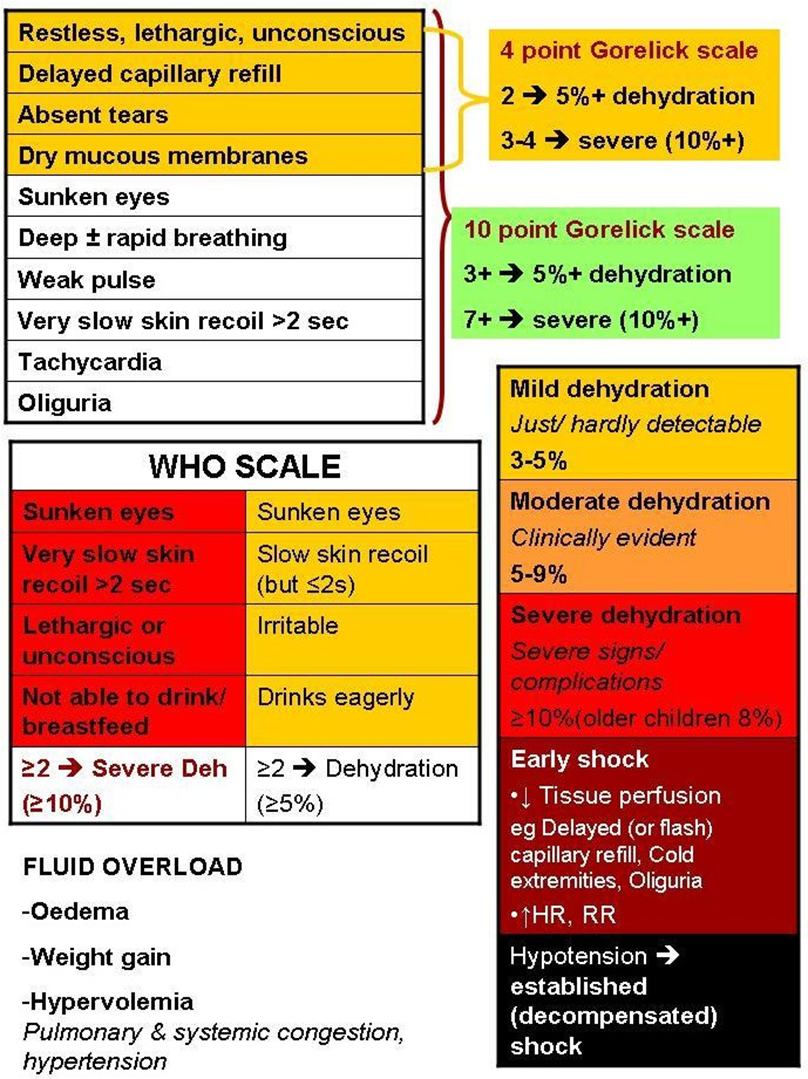
Figure 2: Shock, dehydration & overload assessment chart
Signs of dehydration, shock and overload are shown.
Assessment of dehydration using 4- and 10- point Gorelick scales and WHO scale are presented (35).
Table 5: Fluid balance sheet
|
Time |
Oral/ enteral |
Trans- fusion |
Medication |
IV1 |
IV2 |
TOTAL IN |
Urine |
Out1 |
Out2 |
UF |
TOTAL OUT |
BALANCE |
|
0800 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0900 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1200 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1300 |
|
|
|
|
|
|
|
|
|
|
|
|
|
8am--2pm |
|
|
|
|
|
|
|
|
|
|
|
|
|
1400 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1500 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1600 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1700 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1800 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1900 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2pm-8pm |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total 8am-8pm |
|
|
|
|
|
|
|
|
|
|
|
|
|
2000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2200 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2300 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0100 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0200 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0300 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0400 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0500 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0600 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0700 |
|
|
|
|
|
|
|
|
|
|
|
|
|
8pm-8am |
|
|
|
|
|
|
|
|
|
|
|
|
|
24h total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSENSIBLE |
|
||||||||||
|
Total day |
|
|||||||||||
Figure 3: Hyponatremia & hypernatremia correction (34) HYPONATREMIA
|
ECF volume |
Pathophysiology |
Examples |
Management strategy |
|
Reduced (hyponatremic dehydration) |
Na loss > water loss |
GE, diuretics, adrenal insufficiency, salt- losing nephropathies, etc |
Rehydrate with higher Na Crude: use NS or 3/4NS & modify according to rate of Na rise Accurate: add 10-12 ml/kg hypertonic saline to total daily fluids |
|
Normal |
Free water gain |
SIADH |
Water restriction (50-70%) Use 0.5NS - NS (unless Na restriction is also needed) |
|
Increased |
Water> salt retention |
Congestive HF, hepatic failure, nephrotic syndrome |
-NS, 3/4NS & ½ NS refer to Na content. Appropriate glucose & K should be added
-Correction rate at no more than 0.5 mEq/Kg hourly, preferably even slower (8/day). Check & modify rate of rise after 6h.
-Severe symptomatic cases: initial partial correction with hypertonic saline, followed by more gradual correction
HYPERNATREMIA
|
ECF volume |
Pathophysiology |
Examples |
Management strategy |
|
Reduced (hypernatremic dehydration) |
Water loss> Na loss |
GE |
Give maintenance + 40mL/Kg/day with 1/3NS- ½ NS Modify according to rate of Na drop: - If too slow: ↑rate or ↓Na content, & vice versa |
|
Normal |
Free water loss |
DI |
Give 40mL/Kg free water (eg G5%) per 24h and the remaining fluids as usual |
|
Increased |
Hypertonic Na intake |
Concentrated formula, sea water, Na bicarbonate, etc |
-½ NS & 1/3NS refer to Na content. Appropriate glucose & K should be added.
-Correction rate at no more than 0.5 mEq/Kg hourly (12/day). Check & modify rate of drop after 6h.
-An accurate calculation is possible, based on urine vol, urine Na, insensible loss & current ECF volume status to determine 24h maintenance water & Na requirements separately. Then, allocate 40 mL/kg of the total volume as free water and give the remainder with the proportional amount of calculated Na.
-PD is needed for refractory hyperNa, intractable acidosis or associated AKI with need for dialysis
