
Book
Complete denture maintenance and care
- Methodology
A comprehensive search for guidelines was undertaken to identify the most relevant guidelines to consider for adaptation.
Inclusion/ exclusion criteria followed in the search and retrieval of guidelines to be adapted:
▪️ Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence).
▪️ Selecting only national and/or international guidelines
▪️ Specific range of dates for publication (using Guidelines published or updated in 2015 and later)
▪️ Selecting peer reviewed publications only
▪️ Selecting guidelines written in English language
▪️ Excluding guidelines written by a single author, not on behalf of an organization to be valid and comprehensive, a guideline ideally requires multidisciplinary input
▪️ Excluding guidelines published without references as the panel needs to know whether a thorough literature review was conducted and whether current evidence was used in the preparation of the recommendations.
The following characteristics of the retrieved guidelines were summarized in:
- Developing organization/authors
- Date of publication, posting, and release
- Country/language of publication
- Date of posting and/or release
- Dates of the search used by the source guideline developers
All retrieved Guidelines were screened and appraised using AGREE II instrument (www.agreetrust.org) by at least three members. The panel decided on a cut-off point or ranked the guidelines (any guideline scoring above 50% on the rigor dimension was retained).
The GDG decided to adapt the American College of prosthodontics guidelines 2011 (ACP) for maintenance and care (1).
Evidence assessment
According to WHO Handbook for Guidelines, we used the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach to assess the quality of a body of evidence, develop and report recommendations. GRADE methods are used by WHO because these represent internationally agreed standards for making transparent recommendations. Detailed GRADE information is available on the following sites:
▪️GRADE working group: http://www.gradeworkingroup.org
▪️ GRADE online training modules: http://cebgrade.mcmaster.ca/
▪️ GRADE profile software: http://ims.cochrane.org/revman/gradepro
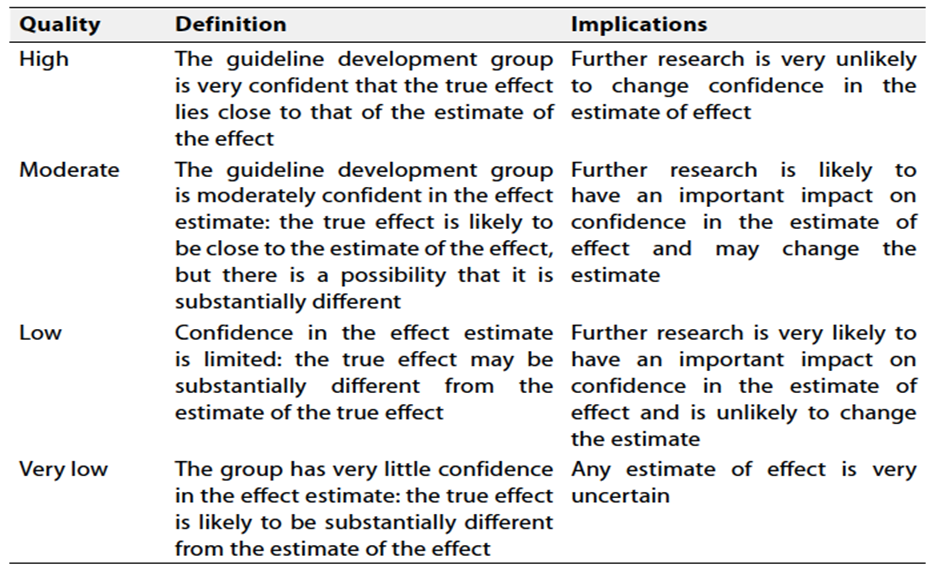
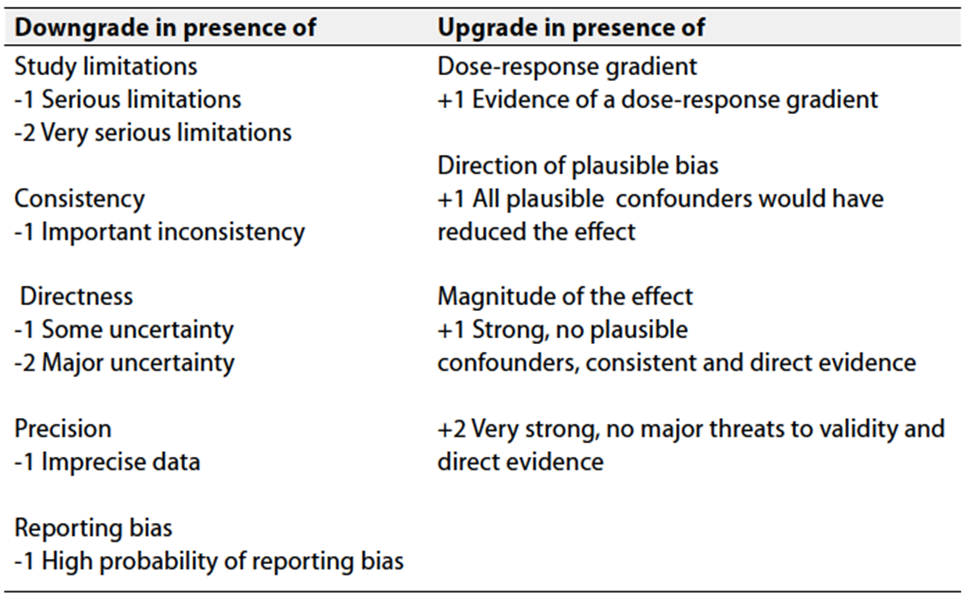
Table 2: Factors that determine How to upgrade or downgrade the quality of evidence
The strength of the recommendation
The strength of a recommendation communicates the importance of adherence to the recommendation.
Strong recommendations
With strong recommendations, the guideline communicates the message that the desirable effects of adherence to the recommendation outweigh the undesirable effects. This means that in most situations the recommendation can be adopted as policy.
Conditional recommendations
These are made when there is greater uncertainty about the four factors above or if local adaptation has to account for a greater variety in values and preferences, or when resource use makes the intervention suitable for some, but not for other locations. This means that there is a need for substantial debate and involvement of stakeholders before this recommendation can be adopted as policy.
When not to make recommendations
When there is lack of evidence on the effectiveness of an intervention, it may be appropriate not to make a recommendation.
Recommendations for the professionals and general practitioners for the maintenance and care of their complete denture:
▪️ Advise the patient to carefully remove the bacterial biofilm daily from both the oral cavity and the surfaces of the complete dentures. (2-4) (Strong recommendation- high grade evidence).
▪️ Advise the patient to soak and brush the removable prosthesis outside the mouth using an effective, nonabrasive denture cleanser. After soaking and brushing, thoroughly rinse it with a denture-cleansing solution before reinserting it into the oral cavity (5-7) (Conditional recommendation-Low grade evidence).
▪️ Advise the patient to have their removable prosthesis professionally cleaned by a dentist or dental professional annually. Ultrasonic cleansers should be used (if available) to minimize biofilm accumulation over time (8-9) (Conditional recommendation- Low grade evidence).
▪️ Advise the patient to avoid soaking dentures in sodium hypochlorite bleach or any products containing sodium hypochlorite for more than 10 minutes (10-16) (Strong recommendation- High grade evidence).
▪️ Advise the patient to store the dentures immersed in water after cleaning, whenever they are not in the oral cavity (Good practice statement).
▪️ Advise the patient to avoid wearing dentures continuously to help reduce or minimize the risk of denture stomatitis (Good practice statement).
▪️ Advise the patient to apply denture adhesive in small, sufficient amounts (three or four pea-sized dollops) on each denture to enhance retention and stability of the prostheses (17-27) (Conditional recommendation - Low grade evidence).
▪️ Advise the patient to completely remove denture adhesive from both the prosthesis and the oral cavity daily (20,22) (Good practice statement).
▪️ Consider arrangement of three-month periodic visits to evaluate the fit and stability of the dentures if extended use of denture adhesives is required (Good practice statement).
▪️ Consider arrangement of an annual follow-up visit with a prosthodontist for maintenance of the removable prosthesis and evaluation of both soft and hard oral tissues (Good practice statement).
