Book
Neonatal Resuscitation Guide
- Neonatal Resuscitation
Introduction:
The first moments of a newborn’s life are considered the “golden moment” and are
among the most critical and dangerous for the infant’s survival. Therefore, the
neonatal nurse must anticipate potential problems the newborn may face due to
the inability to initiate effective ventilation, ensuring successful
resuscitation without complications.
The role of the neonatal unit nurse can be divided into five stages:
First: Before Birth (Preparation):
- Respond immediately upon receiving the birth notification and ensure the resuscitation kit is complete.
- Ensure the resuscitation area is prepared and contains:
- A clean, functioning warming device, securely mounted vertically on the wall and turned on 10–20 minutes before birth.
- A manual or electric suction device, clean and functioning, specifically for neonates; check suction power to ensure it is between 80–100 mmHg.
- An oxygen source connected to a flowmeter and oxygen tubing.
- A neonatal resuscitation kit or mobile emergency trolley, checked and signed off at the start of each shift, containing:
- Neonatal Ambu bag (200–750 mL) with face masks (sizes 0, 1, 2).
- Laryngoscope with straight blade: size 0 for preterm, sizes 00 or 1 for full-term, with functional light check.
- Endotracheal tubes (sizes 2, 2.5, 3, 3.5, 4).
- Cannulas (sizes 24, 26), suction catheters (size 6), umbilical catheters (sizes 3.5, 5).
- Sterile scalpel and umbilical clamp.
- Sterile gloves and mucus suction device.
- Adhesive tape, airway devices.
- Feeding tube (size 6).
- Syringes (1 mL, 3 mL, 5 mL, 10 mL).
- Ampoules: Adrenaline, Vitamin K, Solu-Cortef, Atropine.
Second: During Birth:
- Connect the oxygen tubing to the flowmeter and adjust flow to 5–8 L/min.
- Attach an appropriately sized suction catheter to the suction device, keeping it in its pouch.
- Ensure the Ambu bag mask fits properly, and check for leaks by placing it on the palm.
- Connect the appropriately sized laryngoscope blade and confirm the light works; use only when needed.
- Apply infection control measures throughout all steps.
- Assess readiness for neonatal resuscitation:
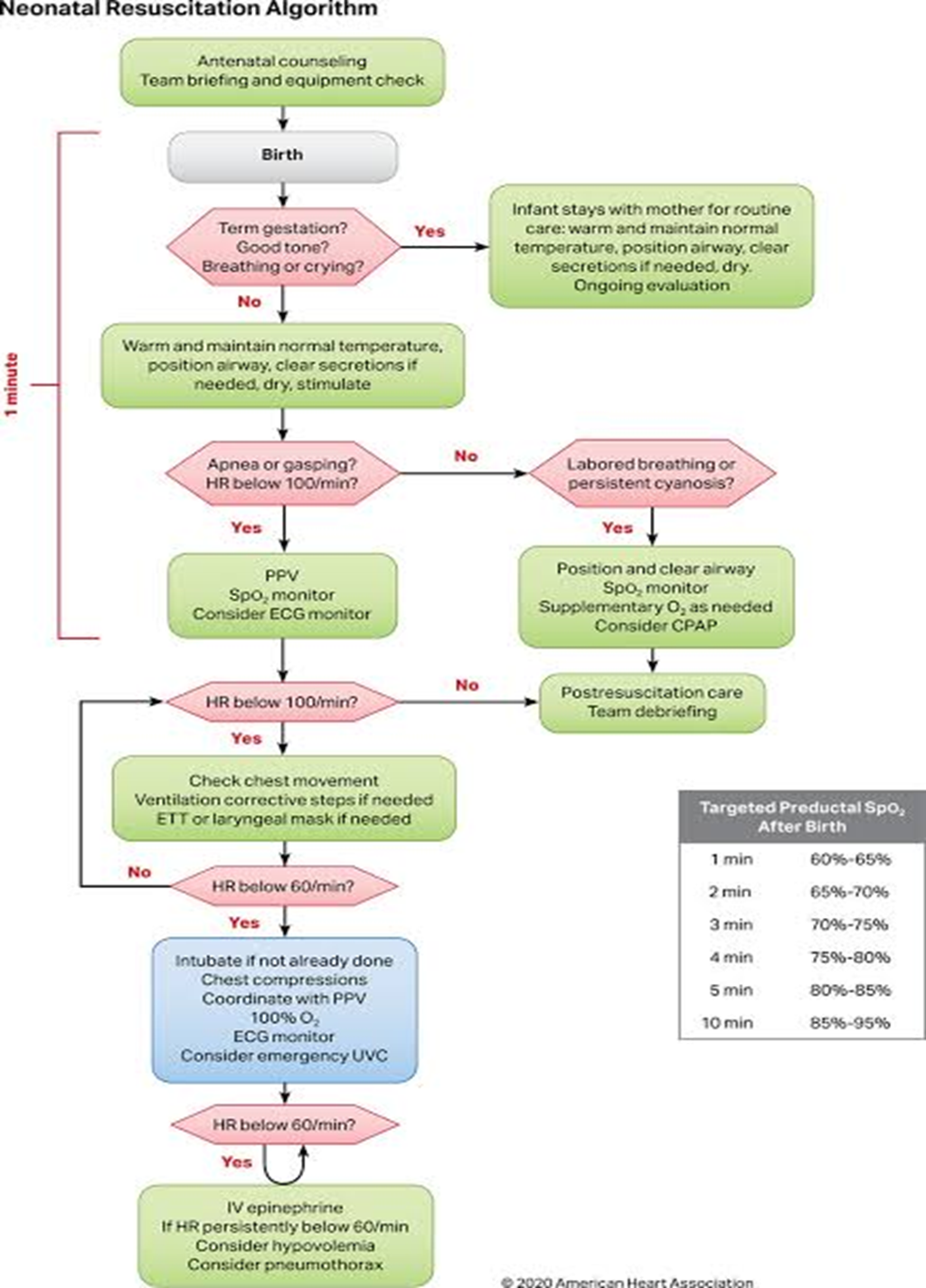
Rapid Initial Assessment (answer three questions):
- Was the gestation full-term?
- Does the newborn have good muscle tone?
- Is the newborn breathing or crying?
- If all answers are “yes,” the newborn stays with the mother for routine care:
- Dry the infant with a sterile towel to maintain temperature.
- Observe breathing, activity, and color continuously.
- Skin-to-skin contact with the mother.
- If any answer is “no,” transfer the newborn to the warming device and follow these steps:
- Stabilize the infant (maintain normal temperature, proper positioning, clear airway if secretions are present, dry, and stimulate).
- Provide oxygen and adequate ventilation.
- Begin chest compressions if needed.
- Administer medications (e.g., adrenaline).
- Delay umbilical cord clamping for 1–3 minutes after birth, unless immediate intervention is required due to asphyxia, to reduce neonatal anemia, improve tissue oxygenation, and stabilize circulation and blood pressure.
Third: Initiating Neonatal Resuscitation Steps:
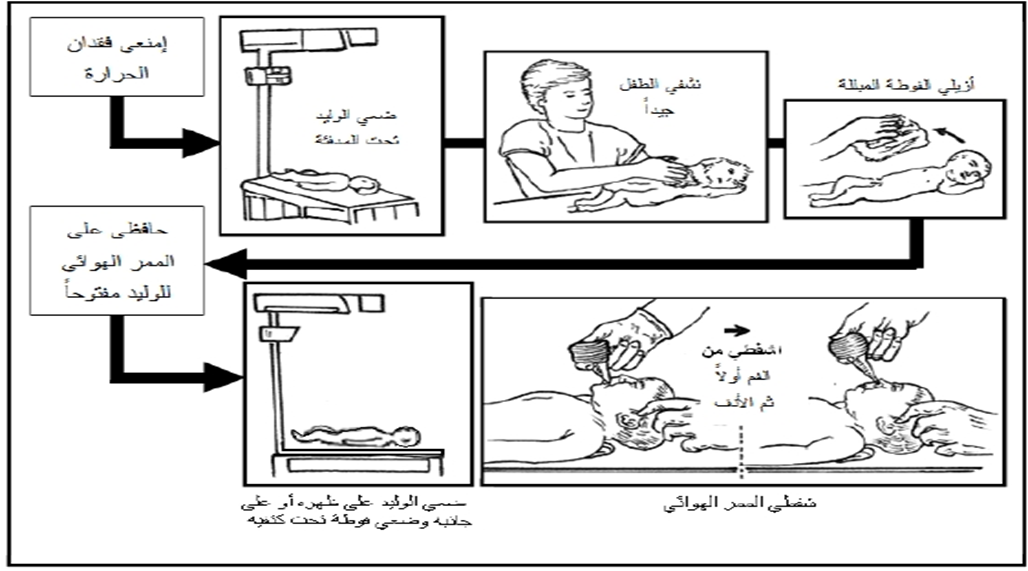
- Receive the newborn in a warm, sterile towel from the obstetrician, avoiding holding the baby by feet or head downward.
- Place the newborn on their back under the warming device, with the head toward the resuscitation nurse.
- Dry the newborn thoroughly, especially the head, and discard wet towels.
- Maintain airway patency by placing a towel under the shoulders (sniffing position).
- Gently suction the mouth first, then the nose, for no more than 5 seconds.
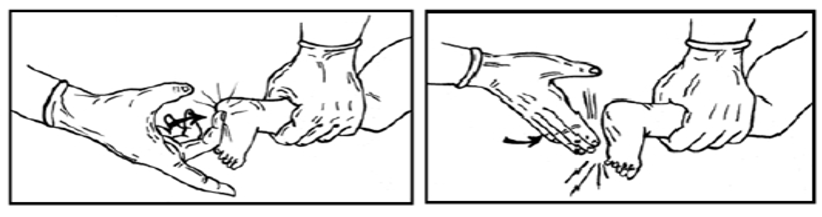
- Stimulate the newborn by gently rubbing the back or tapping the soles of the feet if spontaneous breathing does not start.
- If the amniotic fluid is meconium-stained and the baby is limp, perform full resuscitation on the servo device. Begin ventilation using the Ambu bag and mask if the newborn is not breathing and heart rate is below 100 bpm.
- Endotracheal intubation for meconium suction is no longer routinely recommended.
Fourth: Assessment
- Evaluate the newborn’s condition based on heart rate, respiratory effort, and color.
- An increase in heart rate during resuscitation is the most important indicator of successful resuscitation. Continuous monitoring of heart rate is essential during resuscitation, as it also reflects respiratory status and the need for further interventions. Assessment is done using three electrodes connected to a monitor for accurate heart rate measurement, which is more precise than manual pulse counting. Respiratory effort is evaluated by checking for apnea (pauses in breathing), and color is assessed for cyanosis.
Continuation of Resuscitation Steps
- If there is no apnea and the heart rate is above 100 bpm, but the newborn has respiratory distress or central cyanosis:
- Adjust position, suction the airway, monitor oxygen saturation (SpO₂), provide free-flow oxygen per physician orders, and apply CPAP if needed.
- Reassess the infant: if improved, proceed with post-resuscitation care; if not, or if heart rate drops below 100 bpm, begin ventilation using Ambu bag.
- If there is apnea and the heart rate is below 100 bpm:
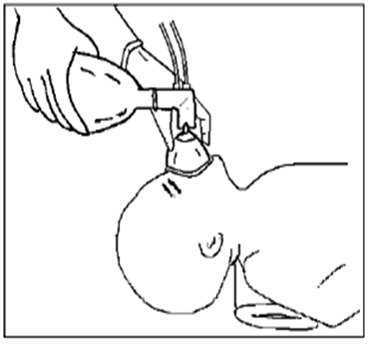
- Perform ventilation using Ambu bag and mask while monitoring heart rate and SpO₂ as follows:
- Ensure the head is in the sniffing position; place a towel under the shoulders if necessary; confirm airways are clear.
- Place appropriately sized mask over the chin, mouth, and nose without touching the eyes. Ventilate following a “1–2–3” system, adjusting squeeze strength according to the newborn’s chest rise.
- Observe chest rise during ventilation and adjust squeeze strength; intubate if required.
- Reassess heart rate:
- If improved, proceed with post-resuscitation care.
- If not improved, continue ventilation; if heart rate drops below 100 bpm, continue Ambu ventilation.
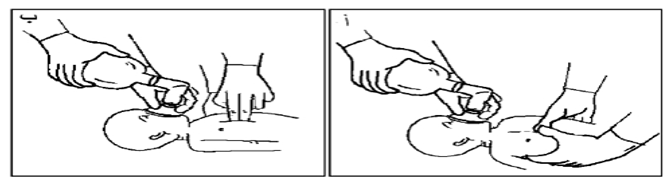
- If heart rate drops below 60 bpm, intubate if not already done and begin chest compressions while continuing ventilation:
- Place thumbs on the lower third of the sternum, wrap hands around the chest with fingers meeting behind the back, or place index and middle fingers of one hand on the lower third of the sternum and the other hand supporting the back. Compress the chest about one-third of its lateral diameter.
- Coordinate compressions with ventilation using the “three compressions” system, taking ~2 seconds per cycle, totaling 120 actions per minute (90 compressions to 30 breaths per minute).
Important Note:
- The “1–2–3” system is used when respiratory compromise is the primary cause.
- If cardiac problem is the main cause, use the higher rate system: 15 compressions : 2 breaths.
- If heart rate remains below 60 bpm:
- Insert an umbilical catheter, administer IV adrenaline, correct fluid deficits, and take measures to prevent pneumothorax.
Fifth: Medication Administration
- If heart rate remains below 60 bpm:
- An umbilical catheter is inserted by the pediatrician.
- Diluted IV adrenaline is administered (dose per physician’s instructions).
- Fluid deficits are corrected using volume expanders as directed (e.g., 0.9% saline or Ringer’s lactate).
Note:
- If prolonged ventilation with an Ambu bag is required, a feeding tube (Ryle tube) should be inserted to decompress the stomach, preventing diaphragmatic pressure and allowing full lung expansion.
Termination of Resuscitation
- If the newborn does not breathe or the heart does not beat after 15 minutes of full resuscitation efforts, resuscitation is stopped, and emotional support is provided to the mother and family.
- If the newborn responds to resuscitation, they should remain under a warming device with close monitoring until stable.
- The newborn may be transferred to the neonatal care unit for ongoing care if needed, with continuous monitoring of vital signs and observation for abnormal signs such as apnea, increased respiratory effort, or central cyanosis, and the physician should be notified immediately.
Ethical Considerations in Resuscitation
- Written consent should be obtained from parents if resuscitation is not to be continued.
- According to physician judgment, resuscitation may not be attempted in the following cases:
- Gestational age less than 22 weeks.
- Severe congenital malformations affecting multiple body parts.
Routine Post-Resuscitation Care
- Care of the umbilical cord.
- Administration of Vitamin K.
- Instillation of antiseptic eye drops.
- Maintain stable body temperature.
- Initiate breastfeeding.
- Promote maternal-infant bonding immediately after birth.
- Encourage skin-to-skin contact.
- Identification of the newborn.
- Record the newborn’s weight.
After Completion of Resuscitation
- Dispose of used instruments in their designated locations.
- Clean and disinfect the warming device.
- Disinfect the Ambu bag, masks, and laryngoscope blade.
- Record resuscitation duration and interventions in the mother’s or newborn’s record.
- Replenish used items in the resuscitation kit upon return to the neonatal care unit.