Book
Newborn Assessment Guide
- Initial Nursing Assessment of Newborns
Purpose:
- Identify the nursing needs of each sick child to develop an appropriate nursing plan based on those needs.
Procedures:
A. Patient Admission by the Nursing Staff:
- The responsible nurse introduces herself to the child's guardians and greets them.
- The nurse verifies the patient's information (full name, mother's full name, age, gender, nationality, and medical record number).
- The nurse prepares an identification bracelet for the newborn, including:
- Full name if a birth certificate is available.
- Mother's full name and medical record number if a birth certificate is not available.
- The bracelet should indicate "Son/Daughter of [Mother’s Name]."
- Conduct a comprehensive physical assessment.
B. Nursing Assessment:
- The responsible nurse or an accredited assistant nurse conducts the initial nursing assessment for newborns upon admission.
- The newborn assessment includes:
- Vital signs measurement
- Length, weight, head circumference, and abdominal circumference
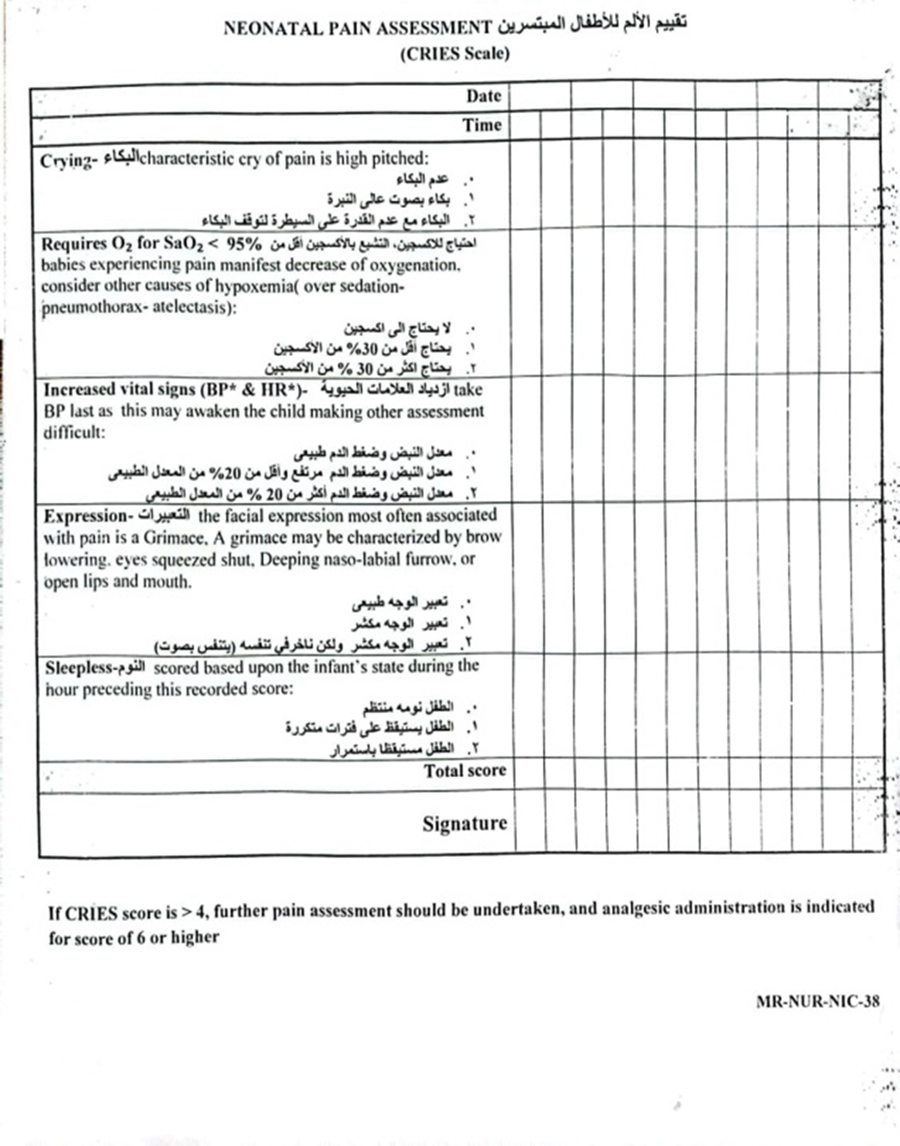
- Pain assessment using the CRIES scale
- Vaccination status
- Neurological condition
- Nutritional assessment
- Skin condition screening
- Examination for congenital anomalies
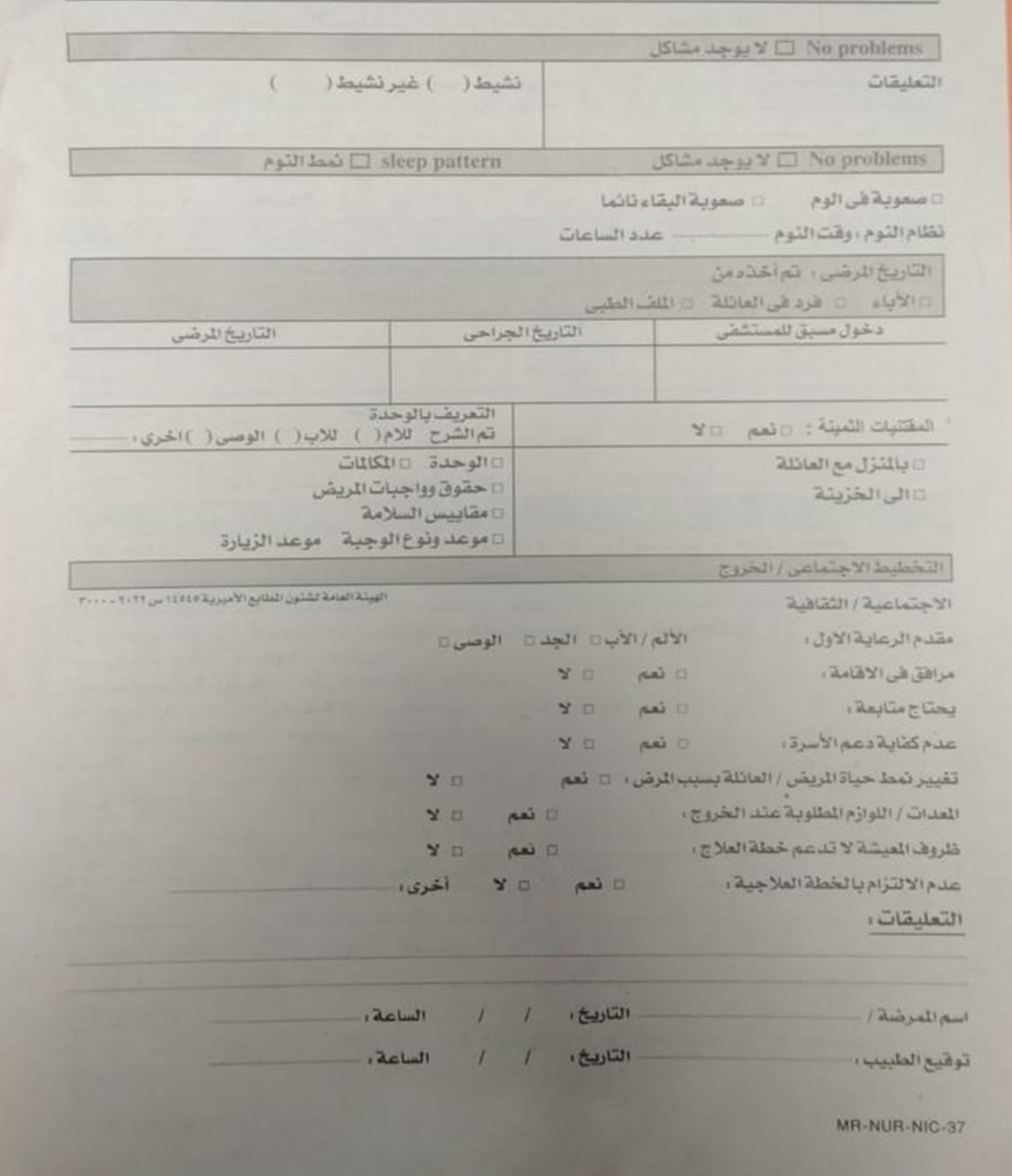
- Sleep pattern
- Medical history (obtained from the guardians)
- Discharge planning
C. Reassessment:
- The responsible nurse re-evaluates the child's condition whenever there is a change in treatment, care stage, or diagnosis, documenting it in the nursing notes.
- The nurse conducts reassessments as follows:
- Vital Signs Reassessment:
- Every 3 hours for preterm infants in incubators or as per the doctor's instructions.
- Every hour for post-open-heart surgery cases and isolation unit patients.
- Documented in the vital signs chart.
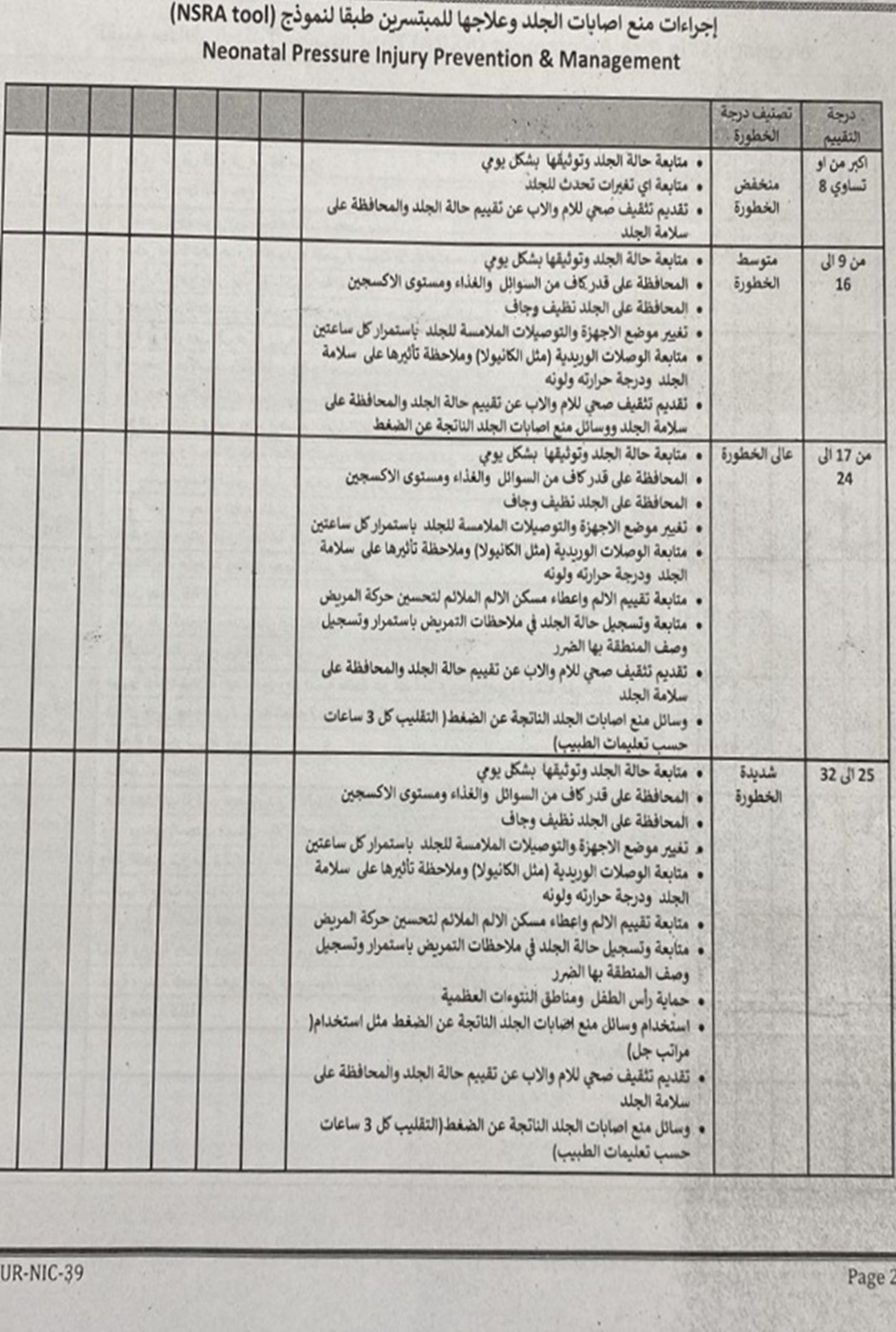
- Skin Condition Reassessment (Bedsores):
- Every 24 hours, documented in the Newborn Skin Risk Assessment (NSRA) form.
- Pain Reassessment:
- Every 12 hours.
- In case of pain occurrence.
- Before and after surgeries.
- One hour after pain relief treatment.
- As per doctor's orders.
- Documented in the pain assessment form.
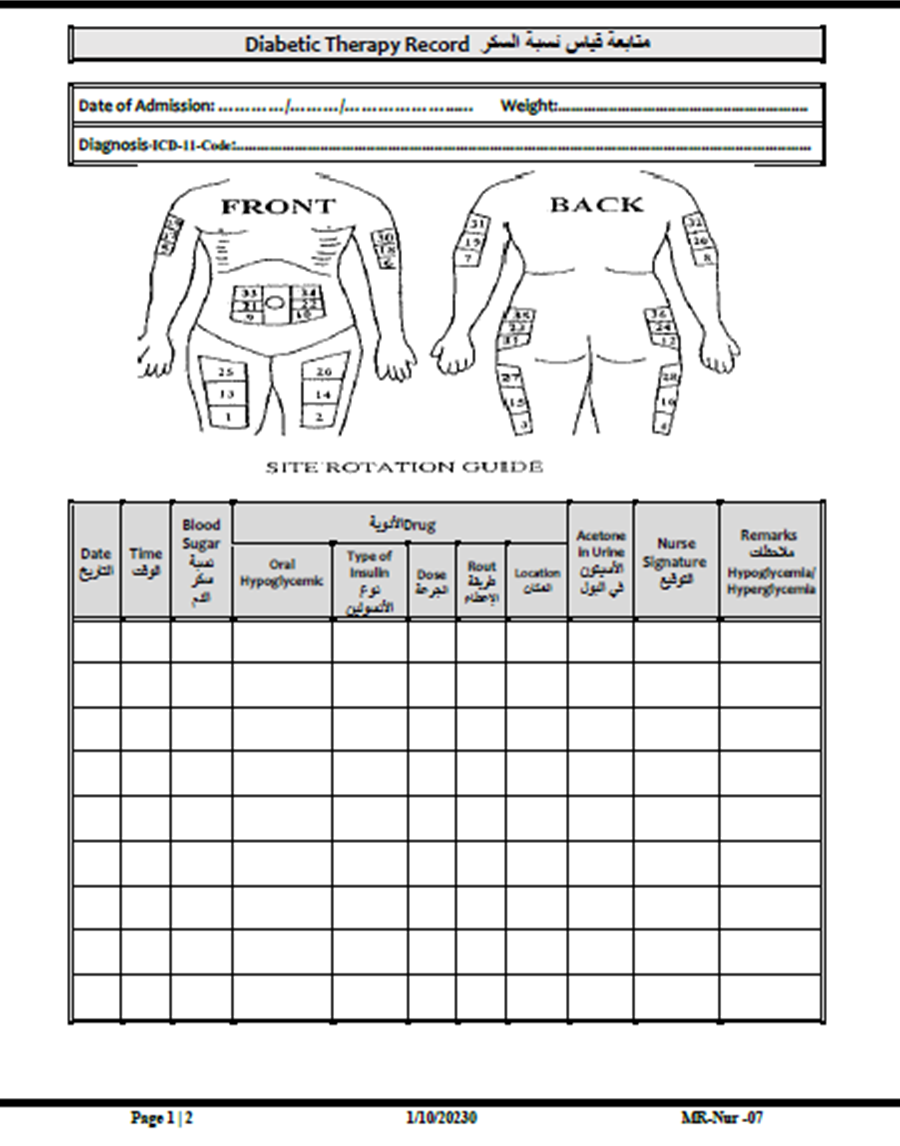
- Blood Sugar Reassessment:
- Every 6 hours (or as per the doctor's orders), documented in the blood sugar monitoring form.
D. Nursing Care Plan:
- The nurse develops a nursing care plan based on the newborn’s needs and updates it in case of any medical interventions or complications.
E. Documentation:
- The nurse completes the initial newborn assessment within 12 hours of admission to the neonatal unit or as per hospital policy.
5. Responsible Personnel:
- The responsible nurse overseeing the case.
6. Attachments:
- Newborn Initial Assessment Form
- CRIES Pain Assessment Form
- Newborn Skin Risk Assessment (NSRA) Form
- Blood Sugar Monitoring Form