
Book
Nursing Guidelines for Burn Treatment
- Treatment of Burn
First: Minor Burns
- Treatment is conducted on an outpatient basis.
- Topical treatment: Sulfadiazine dressings (for children aged 2 months and older and adults) or sterile fatty tulle (except for superficial first-degree burns).
- Pain management: Paracetamol ± Tramadol is usually effective.
Second: Severe Burns
- First Aid:
Upon hospital admission: - Ensure the airway is unobstructed and provide high-flow oxygen, even if blood oxygen saturation is normal.
- Establish an intravenous line through unburned skin if possible (use intraosseous access if intravenous access is unavailable).
- Administer Lactated Ringer's solution: 20 mL/kg in the first hour, even if the patient is stable.
- Administer subcutaneous morphine: 0.2 mg/kg (level 1 and 2 analgesics are ineffective).
- For chemical burns: Wash thoroughly with copious amounts of water for 15–30 minutes, avoiding contamination of intact skin. Do not attempt to neutralize the chemical agent.
Once the patient is stabilized:
- Remove clothing if it is not adhered to the burns.
- Take a burn history: mechanism, causative agent, time of occurrence, etc.
- Assess the burn: extent, depth, charred areas; check for burns to the eyes, functionally significant areas, circumferential burns of the limbs, chest, or neck. Wear a sterile face mask and gloves during the examination.
- Evaluate associated injuries (fractures, etc.).
- Protect the patient and keep them warm using a clean/sterile sheet or a thermal blanket.
- Insert a urinary catheter if burn surface area exceeds 15% of total body surface area (TBSA), in cases of electrical burns, or burns to the perineum/genital area.
- Insert a nasogastric tube if burn surface area exceeds 20% TBSA (done in the operating room during dressing procedures).
- Calculate fluid requirements for the first 24 hours and initiate administration.
- Closely monitor the following: level of consciousness, heart rate, blood pressure, oxygen saturation, respiratory rate (hourly); temperature and urine output (every 4 hours).
- Perform laboratory tests: hemoglobin, blood typing, and urinalysis.
- Prepare the patient for the first dressing procedure in the operating room.
Notes:
- Burns do not bleed initially. Investigate any bleeding if hemoglobin levels are normal or low.
- Burns do not alter consciousness on their own. Changes in consciousness suggest head injury, poisoning, or a preexisting condition like epilepsy.
- Clinical signs of electrical burns vary widely with the type of electrical current. Look for complications (e.g., arrhythmias, neurological disorders).
- General Measures During the First 48 Hours Resuscitation Measures:
Administer intravenous fluids to correct hypovolemia:
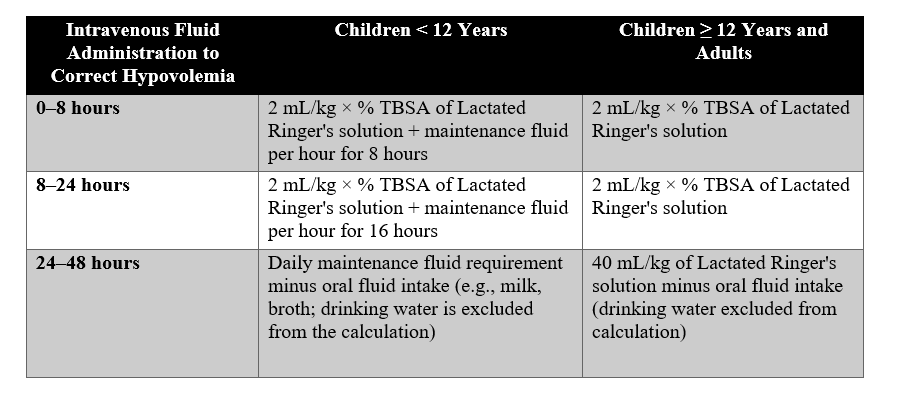
Fluid Requirements During the First 48 Hours by Age
- (A) Maintenance fluid: Alternate between Lactated Ringer's and 5% Dextrose solutions:
- 4 mL/kg/hour for the first 10 kg of body weight.
- +2 mL/kg/hour for the next 10 kg of body weight.
- +1 mL/kg/hour for each additional kg (above 20 kg, up to 30 kg).
Note: Increase fluid volume by 50% (3 mL/kg × % TBSA for the first 8 hours) in cases of inhalation injury or electrical burns. For burns > 50% TBSA, limit calculations to 50% TBSA. Adjust fluid administration based on systolic blood pressure and urine output to avoid fluid overload.
Vascular Resuscitation Targets:
|
Type of Burn |
Systolic BP |
Urine Output |
|
Non-electrical burns |
≥ 60 mmHg (children < 1 year) |
1–2 mL/kg/hour |
|
70–90 mmHg + (2 × age) (children 1–12 years) |
0.5–1 mL/kg/hour (adults) |
|
|
Electrical burns |
Age-appropriate systolic BP |
1–2 mL/kg/hour |
For patients with oliguria despite adequate fluids:
- IV dopamine: 5–15 mcg/kg/min via an infusion pump.
- Or IV epinephrine: 0.1–0.5 mcg/kg/min via an infusion pump.
Discontinue IV fluids after 48 hours if oral fluid intake can meet hydration needs.
Types of Fluids Used in the Burn Unit:
- Crystalloids:
- Lactated Ringer's Solution: The first choice for fluid resuscitation.
- Normal Saline: Used in specific cases, but monitor for metabolic acidosis.
- Colloids:
- Albumin or plasma expanders: Used later to replenish proteins and osmotic pressure.
