Book
Procedural Manual For Delivery Cases
- Neonatal Resuscitation
- Introduction: Most newborns transition smoothly from the womb to life outside, but some may need resuscitation within the first minute, known as the "golden minute."
- Initial assessment: The need for resuscitation depends on:
- Full-term pregnancy or not.
- Presence of good muscle tone.
- Breathing or crying.
- If the answer is yes to all questions, provide routine care: drying, skin-to-skin contact with the mother, and continuous monitoring of the baby's color, breathing, and activity.
- If no to any question, follow these steps in order:
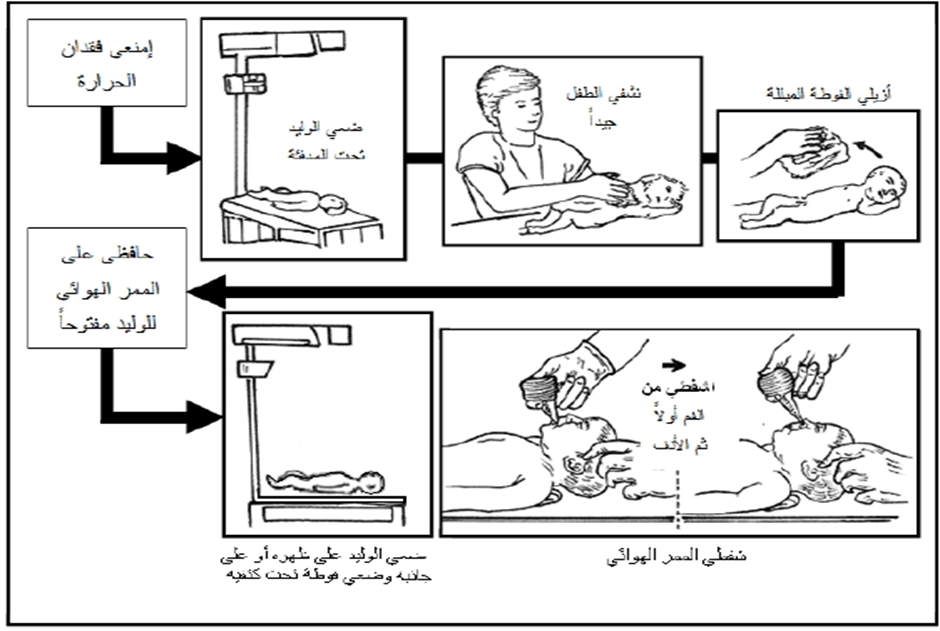
- Stabilization: Provide warmth, clear airways, dry, and stimulate the baby.
- Oxygen administration.
- Chest compressions if heart rate is below 60 bpm.
- Administer medications like adrenaline if necessary.
- Cord clamping: Delayed cord clamping is recommended for at least 30 seconds for full-term or preterm babies not requiring resuscitation.
Assessment
- The newborn's condition is assessed based on three parameters: heart rate, effort in breathing, and color.
- An elevated heart rate during recovery is considered the most important indicator of successful recovery. Continuous monitoring of heart rate is crucial during the recovery process as it is also used to assess the respiratory system and determine the need for further interventions. The assessment is done by attaching three electrodes connected to a heart monitor to track the pulse, as this method is more accurate than manually counting the pulse. Breathing effort is assessed by checking if there is any apnea (cessation of breathing). The newborn’s color is checked for signs of cyanosis (blueness).
Continuing Recovery Steps
· If there is no apnea, and the heart rate is over 100 beats per minute, but the newborn has difficulty breathing or exhibits central cyanosis, the following steps are taken:
- Adjusting the position, clearing the airway, and monitoring the oxygen saturation (SpO2).
- Administering supplemental oxygen as per the doctor's orders and possibly using CPAP if necessary.
- If there is improvement, post-recovery care is initiated. If there is no improvement or if the heart rate falls below 100 beats per minute, ventilation using an ambu-bag is carried out.
· If apnea is present and the heart rate is below 100 beats per minute, ventilation is performed using an ambu-bag and mask, while monitoring the pulse and oxygen saturation (SpO2), as follows:
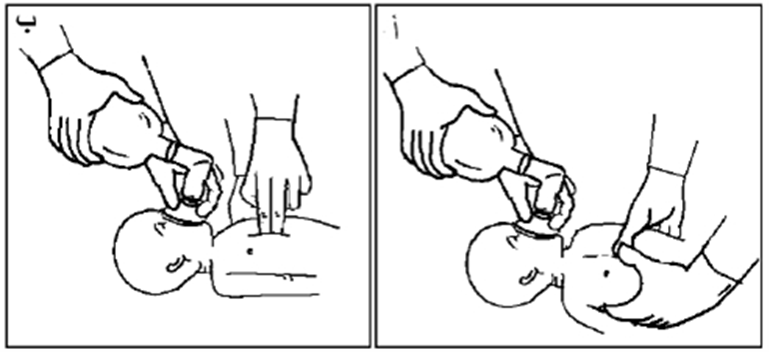
- Ensure the newborn’s head is in the proper sniffing position, placing a towel under their shoulders if needed, and confirming that the airways are clear of secretions.
- A properly-sized mask is placed on the newborn's face, covering the chin, mouth, and nose but not the eyes. Ventilation is done using the (breath – 2 – 3) system, ensuring the appropriate pressure is applied.
- The rise of the chest during ventilation should be monitored, adjusting the pressure based on the chest rise. Endotracheal intubation may be performed if necessary.
· The heart rate is assessed, and if improvement occurs, post-recovery care is initiated. If no improvement is observed despite effective ventilation, and the heart rate remains below 100 beats per minute, ventilation with the ambu-bag and mask continues. If the heart rate drops below 60 beats per minute, intubation is performed (if not done already), and chest compressions are immediately started, along with continued ventilation, as follows:
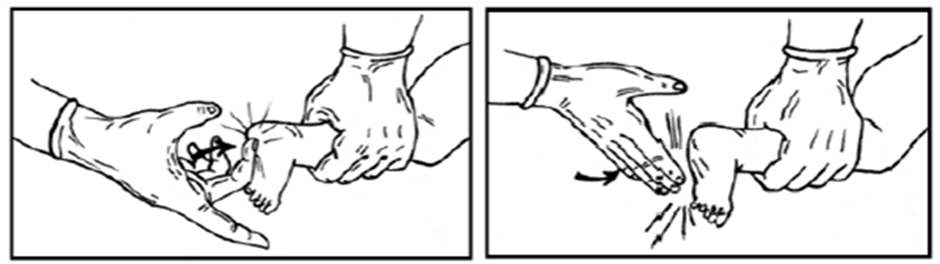
- Place the thumbs on the lower third of the sternum, with the hands wrapped around the newborn's chest, and the fingers meeting behind the newborn’s back. Alternatively, place the middle and index fingers of one hand on the lower third of the sternum, with the other hand supporting the newborn’s back. Apply pressure to the chest, compressing about one-third of the distance to the spine.
- Chest compressions are coordinated with ventilation using the (compress – 2 – 3 – breath) system, which lasts about two seconds per cycle, totaling 120 cycles per minute (90 compressions and 30 breaths per minute).
- This system is used if respiratory compromise is the main issue. If cardiac issues are the primary cause, the higher-pressure system (15 compressions: 2 breaths) is used.
· If the heart rate remains below 60 beats per minute, an umbilical catheter is inserted, adrenaline is administered intravenously, and fluid deficits are corrected, while also preventing the risk of pneumothorax (air in the chest cavity).
These guidelines focus on providing proper care for newborns during the recovery phase, ensuring their heart rate and breathing are closely monitored and supported as needed, with appropriate interventions like ventilation and chest compressions.
Fifth: Administering Medications
- If the heart rate remains below 60 beats per minute, an umbilical catheter is inserted by the pediatrician, and diluted adrenaline is administered intravenously (dosage as per the doctor's instructions). Fluid deficits are corrected by giving volume expanders as per the doctor's instructions (such as 0.9% saline solution or Ringer's lactate solution).
Note: If the newborn requires prolonged ventilation using an ambu-bag, a nasogastric tube (Ryle's tube) should be placed to remove stomach distension, preventing pressure on the diaphragm, which could hinder the full expansion of the lungs.
Ending the Recovery Process
- Recovery efforts are stopped if the newborn does not breathe or has no pulse 15 minutes after full recovery efforts. In such cases, psychological support is provided to the mother and family.
- If the newborn responds to recovery efforts, they must remain under a heating device for monitoring until their condition stabilizes.
- The newborn may be transferred to the neonatal care unit for further required care if necessary, with continuous monitoring of vital signs and any abnormal signs such as (apnea, increased respiratory effort, central cyanosis). The doctor should be informed immediately.
Routine Care for the Newborn After Stabilizing Vital Signs
- Care for the umbilical cord
- Administer Vitamin K
- Apply antiseptic eye drops
- Ensure temperature stability of the newborn
- Initiate breastfeeding
- Foster mother-infant bonding immediately after birth
- Encourage skin-to-skin contact between mother and newborn
- Establish newborn identity
- Weigh the newborn
After Completing the Recovery Process
- Dispose of any tools used for the newborn in their designated place.
- Clean and disinfect the heating device.
- Disinfect the ambu-bag, masks, and laryngoscope blade.
- Record the duration of recovery and document all actions taken for resuscitation in the mother’s or newborn’s medical record, in case the newborn is admitted to the unit.
- Replace used items in the recovery kit when arriving at the neonatal care unit.
This outlines the complete procedure for neonatal resuscitation, administration of necessary medications, post-recovery care, and the hygienic processes to follow after resuscitation efforts.