
Book
Newborn Assessment Guide
- Prevention of Pressure Ulcers in Neonates
Purpose:
- To establish a system for assessing the skin condition and safety of neonates upon hospital admission to determine their risk level for developing pressure ulcers.
- To identify neonates most at risk of pressure ulcers and take necessary preventive measures.
- To help heal existing pressure ulcers in affected neonates.
Definitions:
- Pressure Ulcer: A skin injury caused by impaired blood circulation and continuous friction against a bony area of the body, occurring when the skin is under prolonged pressure from a firm surface, such as a bed.
Procedures:
A. Risk Assessment at Admission, Including Skin Evaluation:
- The nurse conducts a pressure ulcer risk assessment and records it in the neonatal nursing assessment form.
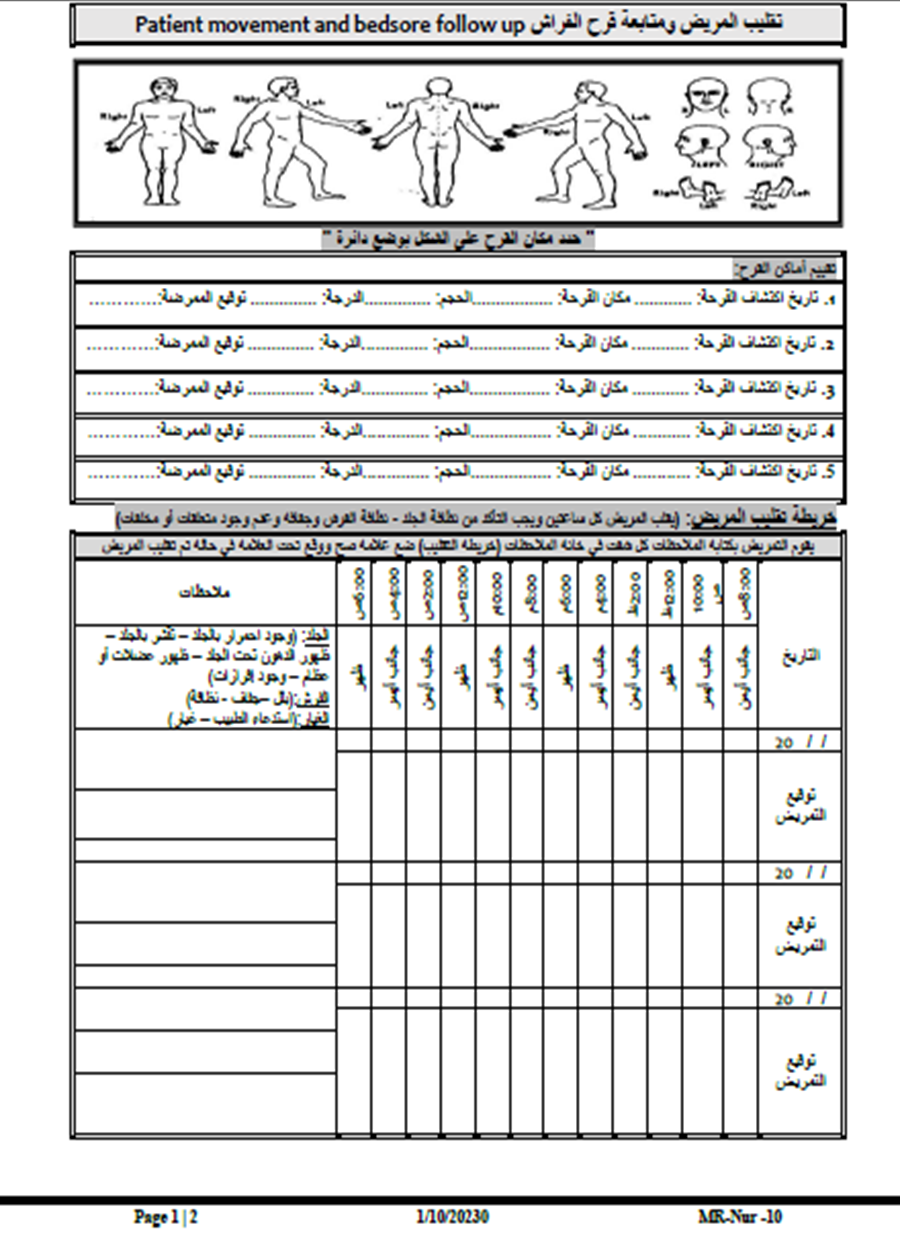
- The nurse examines the skin over bony prominences such as the heels, ankle joints, pelvis bones, coccyx, ears, shoulders, and elbows.
- The nurse checks for areas of redness that persist for more than 30 minutes. For dark-skinned neonates, skin warmth in affected areas should be assessed.
- The nurse classifies the neonate's skin condition as:
- Low risk
- Moderate risk
- High risk
- Severe risk
B. Timeframe for Pressure Ulcer Screening Completion:
- The nurse must complete the screening within two hours of the neonate’s admission to the neonatal intensive care unit (NICU) and record the findings in the neonatal nursing assessment form.
C. Frequency of Pressure Ulcer Risk Reassessment:
- If no pressure ulcers are present at admission, the nurse reassesses the neonate within 24 hours using the Neonatal Skin Risk Assessment (NSRA) Scale:
- Score ≥ 8: Low risk
- Score 9-16: Moderate risk
- Score 17-24: High risk
- Score 25-32: Severe risk
- The nurse performs a daily reassessment every 24 hours using the NSRA scale.
- If a pressure ulcer is present at admission, the nurse documents:
- The number, location, and severity of the ulcers
- The presence of any discharge
Stages of Pressure Ulcers:
- Stage 1: Red or pink area that does not disappear within 30 minutes, similar to a mild sunburn. Skin may feel painful or itchy.
- Stage 2: Red, swollen, and painful skin. Blisters may be present, and the upper skin layers begin to deteriorate.
- Stage 3: The ulcer extends deeper into the skin layers, forming a crater-like wound.
- Stage 4: The ulcer extends into the fat, muscle, or even bones.
D. Actions in Case of Existing Pressure Ulcers:
- The nurse informs the neonate's family about the ulcer's location, severity, and presence of discharge, obtaining written acknowledgment.
- The attending physician is notified to create a treatment plan, which may include consultation with a dermatologist or surgeon.
- For high-risk neonates, the nurse reassesses the skin every two hours to check for redness or dryness and records it in the patient repositioning log.
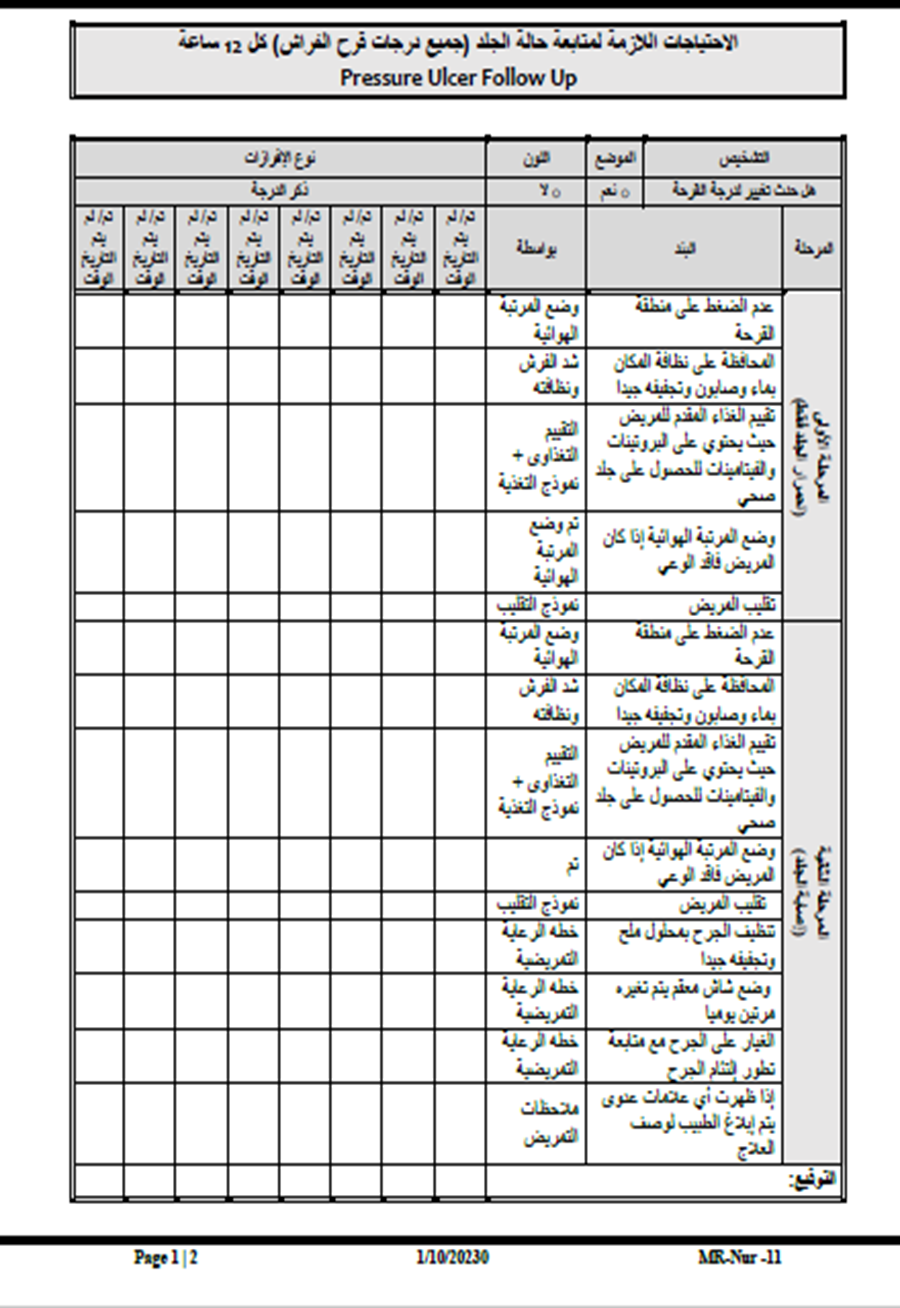
E. Preventive Measures:
- Regular Repositioning:
- The nurse repositions the neonate every two hours and documents it in the repositioning log.
- The neonate's head should be elevated at a 30-degree angle, except during feeding, per physician instructions.
- Skin Protection:
- Use prescribed emollients to reduce friction injuries.
- Avoid massaging over bony prominences.
- Keep the skin clean and dry.
F. Individualized Care Plans Based on Risk Assessment:
- Following the skin assessment, the nurse:
- Reports findings to the physician.
- Develops a care plan to minimize pressure on bony areas, reduce friction, and prevent moisture-related skin damage.
- Establishes a patient repositioning schedule (every two hours or as prescribed by the physician).
- Educates the family on pressure ulcer prevention, documenting it in the health education form and nursing care plan.
Responsibility:
- Attending physician
- Ward nurses
- Nutrition specialist
Attachments:
- Patient Repositioning Log
- Neonatal Skin Risk Assessment (NSRA) Form
- Pressure Ulcer Staging Guide
- Incident Reporting Form
Incident/Error/Unexpected Event Report Form
1. Injured Party Information:
- Name: ................................................
- File/Card Number: ..................
- Age: ...........
- Gender: ..................
- Department: ...............................................
- Admission Date (for patients): ............................
- Category:
- □ Patient
- □ Employee
- □ Visitor
- □ Other (Specify): ........................
2. Type of Incident:
- □ Error
- □ Accident
- □ Significant Unexpected Event
- (Specify) ..................................................
3. Incident Details:
- Date: ....../....../20......
- Time: .......... (AM / PM)
- Exact Location: ..................................................
4. Incident Description and Contributing Factors:
..................................................
5. Corrective Actions Taken:
..................................................
6. Reporter’s Information:
- Name: ..................................................
- Department: ...............................................
- Physician Notified: ...............................................
- Time Report Initiated: ........................
- Witness (if any): ..................................................
- Contact Number: ............................
7. Supervisor’s Information:
- Name: .........................................
- Position: ............................
- Date: ....../....../20......
- Time: .......... (AM / PM)
- Signature: ..........................
8. Medical Supervision (If Injury Occurred):
(Include patient examination, required tests, results, and
diagnosis)
..................................................
- Name: .........................................
- Date: ....../....../20......
- Signature: ..........................
9. Medical Follow-up Information:
..................................................
- Name: .........................................
- Date: ....../....../20......
- Signature: ..........................
10. Department Head’s Instructions (Verification of Report Details):
..................................................
- Name: .........................................
- Date: ....../....../20......
- Signature: ..........................
11. Hospital Director’s Instructions:
..................................................
The report is submitted to the Hospital Quality Improvement Committee Coordinator for recommendations, implementation, and filing.
- Hospital Director’s Signature: ..................................................
- Date: ....../....../20......
