
Book
Newborn Assessment Guide
- Physical Examination of the Newborn
A comprehensive evaluation of the newborn's condition is conducted upon admission to the neonatal care unit. Additionally, an assessment is performed at the beginning of each shift, with findings documented in the newborn's medical record. The evaluation includes:
- General Examination
- Vital Signs Measurement (respiration, pulse, temperature, blood pressure) every 3 hours or as per physician’s instructions
- Growth Measurements Monitoring
- Comprehensive Assessment of Various Body Systems
First: General Examination
This includes observing the following:
1. Body Position
- The newborn is observed while lying on their back, with the head slightly flexed forward (chin touching the upper chest) and full flexion of both arms and legs.
2. Skin Condition
- Assessment of skin color (any discoloration—pale or dark), elasticity, presence of scratches, wounds, or birthmarks.
3. Head and Face
- Fontanelles:
- The anterior fontanelle should be open in a diamond (◊) shape.
- The posterior fontanelle is usually closed at birth, but if open, it appears triangular (Δ).
- Birth Trauma Signs:
- Caput succedaneum: Swelling of the scalp due to fluid accumulation, which resolves within a few days without complications.
- Cephalhematoma: Blood accumulation under the scalp, which disappears within weeks.
- Eyes: Checked for discharge, redness, or swelling.
- Nose: Examined for discharge, nasal septum deviation, or blockage during suction catheter insertion.
- Ears: Checked for visible congenital anomalies.
- Mouth: Assessed for cyanosis, discharge, oral thrush, or congenital defects such as cleft lip or palate.
4. Chest (Breast Tissue)
- Temporary breast swelling in newborns is normal due to maternal hormones transferred through the placenta. Breast tissue should not be squeezed to avoid infection.
5. Umbilical Cord
- Checked for signs of infection, including redness, discharge, foul odor, or bleeding.
6. Other Observations
- Any visible congenital abnormalities should be documented during the initial newborn assessment.
Second: Vital Signs Measurement
Vital signs are measured every 3 hours if the newborn is stable. If unstable, they are checked hourly. The vital signs include:
1. Respiratory Rate
- Measured before touching the newborn.
- The normal range for neonates is 40–60 breaths per minute.
2. Body Temperature
- The normal range is 36.5 – 37.5°C.
- Axillary temperature (underarm) is measured using a thermometer held vertically for:
- 5–7 minutes in full-term newborns.
- 7–10 minutes in preterm or low-birth-weight newborns.
- Note: Some neonatal units measure rectal temperature initially to rule out anal atresia, but using a soft catheter for this is safer. The newborn’s bowel movements are also monitored and recorded for the first 48 hours after birth.
3. Heart Rate
- The normal range is 120–160 beats per minute.
- Counted for a full minute using a stethoscope.
4. Blood Pressure
- Measured at admission from all four limbs using a Dynamap device.
- Routine measurements are then taken from the arm without an intravenous cannula.
- Blood pressure varies with crying (increases) and sleep (decreases) and depends on gestational age and postnatal age.
- Normal systolic: 67–84 mmHg, diastolic: 35–53 mmHg.
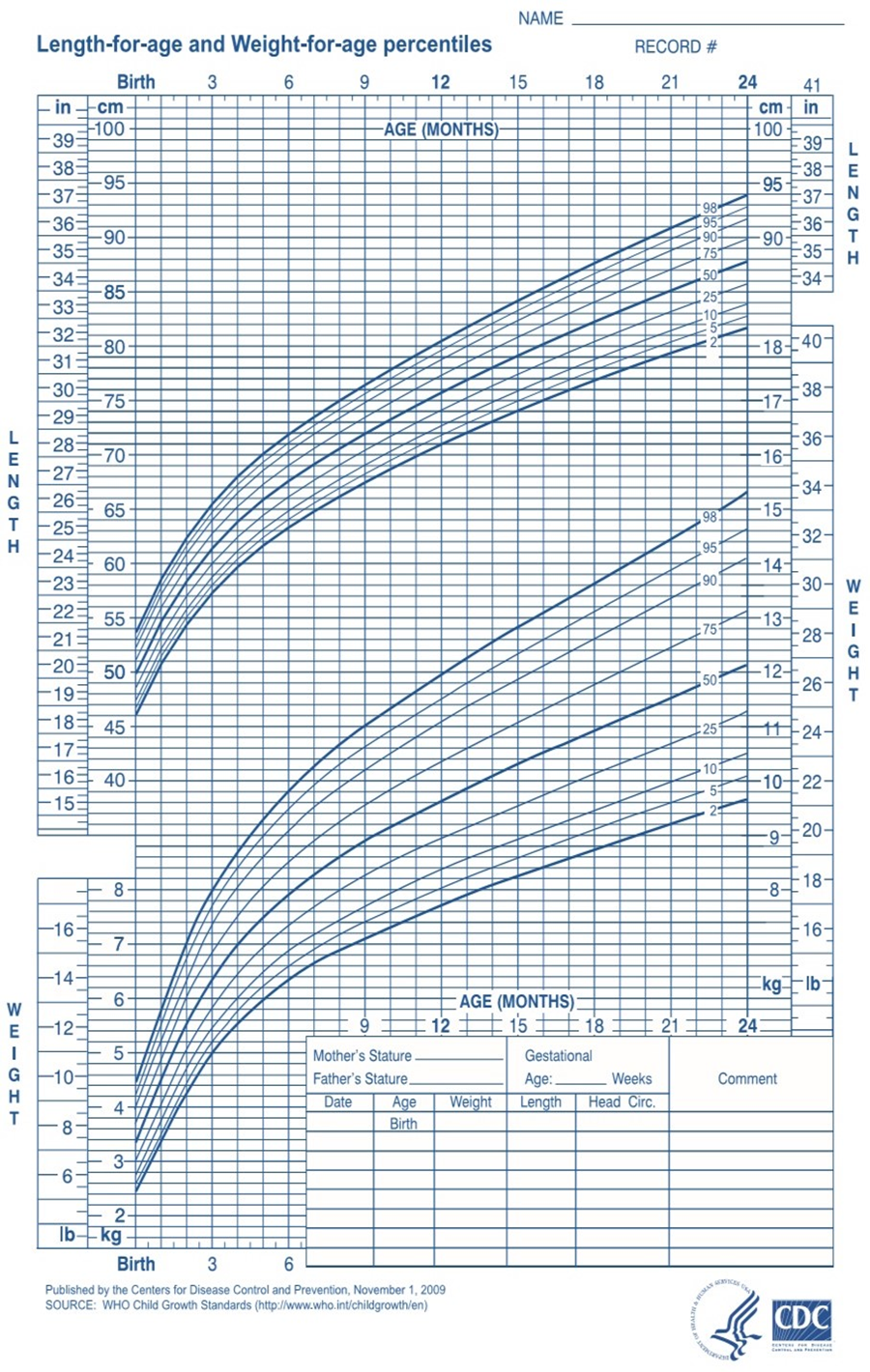
Third: Growth Measurements
1. Weight
- Normal newborn weight: 2700–3850 g.
- Measured once daily (twice daily if birth weight is <1000 g).
- Weight is recorded and tracked using a growth chart, especially for underweight newborns.
- Note: Newborns may lose about 10% of their weight within the first 3–4 days due to fluid loss, urination, and passage of meconium. They regain their birth weight within 10 days.
2. Length
- Normal newborn length: 46–56 cm.
- Measured at admission and then weekly.
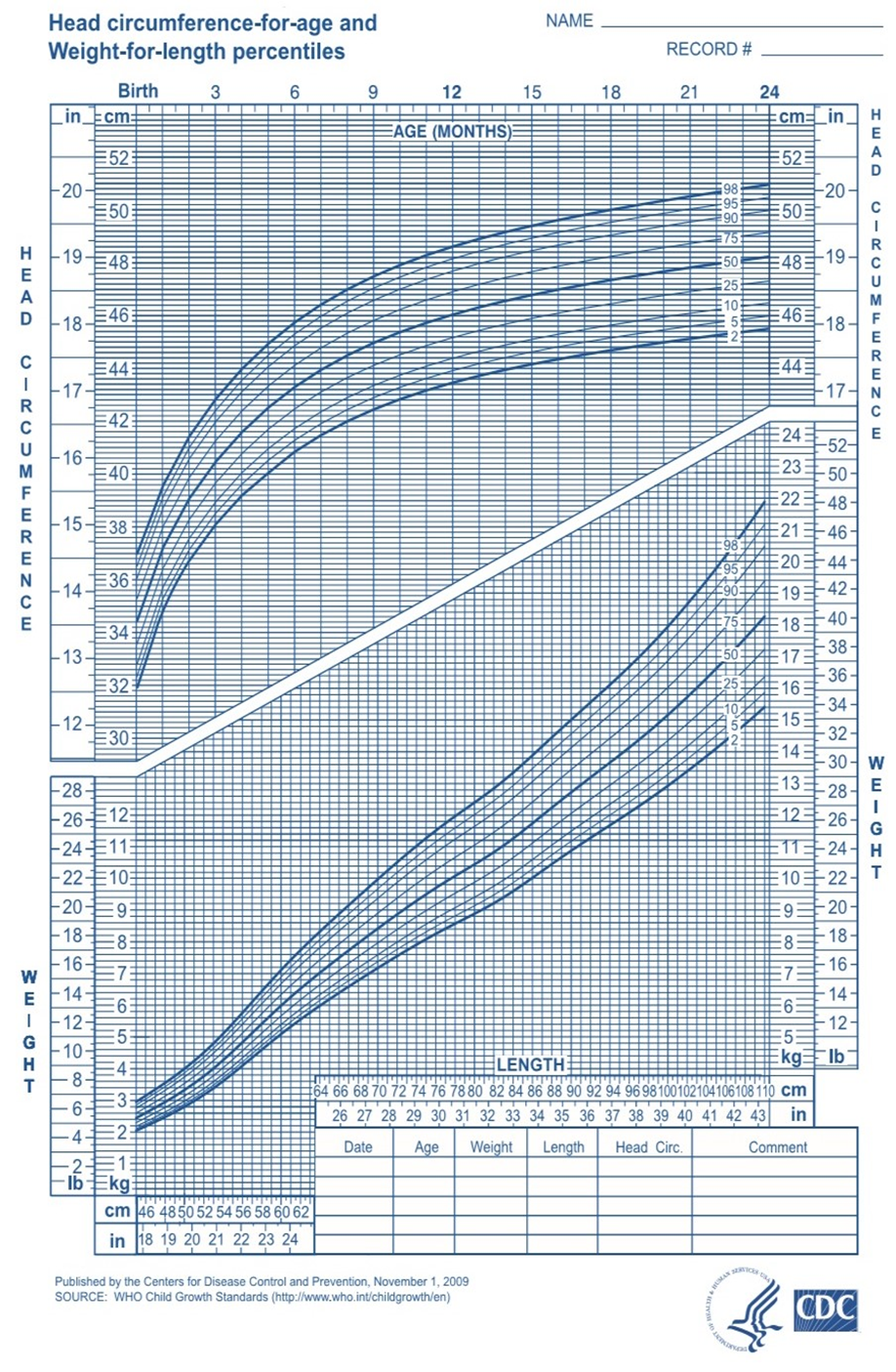
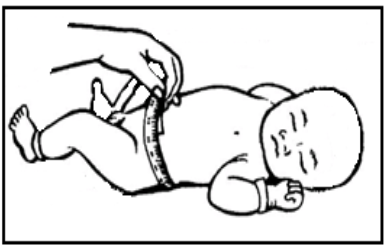
3. Head Circumference
- Normal range: 33–37 cm.
- Measured at admission and weekly.
- Daily measurements are required for newborns with neurological issues (e.g., intraventricular hemorrhage, hydrocephalus, birth asphyxia, or spinal cord infections).
4. Abdominal Circumference
- Normal range: 31–33 cm.
5. Chest Circumference
- Normal range: 30–35 cm.
Fourth: Comprehensive Assessment of Body Systems
1. Nervous and Motor System
The nervous system in newborns is characterized by reflex responses, the most notable being the Moro reflex. The neurological examination includes:
- Movement and Alertness: Whether the newborn is sleeping, awake, tense, stiff, or floppy.
- Body Position: Whether the newborn maintains a flexed posture or has muscle laxity.
- Crying: Whether the cry is strong or weak.
- Fontanelle Condition: Whether it is open or closed, bulging or sunken.
- Seizures: Any presence of convulsions, which should be described if observed.
- Muscle Tone: Whether it is rigid, normal, or weak.
- Weakness or Stiffness in Limbs: Such as Erb’s palsy (brachial plexus injury), clavicle fracture, or muscle stiffness.
- Spinal Abnormalities: Any visible congenital defects of the spine.
2. Cardiovascular System
The cardiovascular assessment includes:
- Heart Rate and Rhythm: Ensuring a regular heartbeat.
- Capillary Refill Time: Pressing on the sternum and counting the seconds until the color returns to normal (normal is <3 seconds).
3. Respiratory System
Respiratory evaluation involves:
- Skin Color: Observing if it is pink, blue (cyanotic), or pale.
- Respiratory Rate: Checking if it is within the normal range.
- Symmetry of Chest Movements: Ensuring both sides of the chest move equally with breathing.
- Chest and Abdominal Coordination: Evaluating synchronized movements.
- Signs of Respiratory Distress:
- Increased respiratory rate (>60 breaths per minute)
- Grunting sounds
- Chest retractions
- Episodes of apnea (pauses in breathing)
- Presence of secretions
- Chest Circumference Measurement.
4. Digestive System
The digestive system examination includes:
- Abdominal Shape: Checking for distension or abnormalities.
- Abdominal Circumference Measurement: At the level of the umbilicus.
- Presence of Vomiting: Recording the content and color, if present.
- Passage of Meconium: Ensuring that the first stool (meconium) is passed within 24–48 hours after birth.
5. Genitourinary System
For Female Newborns:
- Mild swelling of the external genitalia (normal).
- Ensuring the labia majora covers the labia minora.
- Possible vaginal discharge or slight bleeding due to maternal hormone transfer.
For Male Newborns:
- Checking that the urinary meatus is at the tip of the penis.
- Ensuring both testes have descended into the scrotum.
- Observing the scrotum for swelling, fullness, dark coloration, and prominent folds.
- Ensuring urination occurs within 24 hours of birth and assessing the color (light yellow) and quantity (1–3 mL/kg/hr).
