
كتاب
دليل مشكلات الجهاز التنفسي
- الاختناق الوليدي
یحدث الاختناق الولیدي نتیجة عدم وصول الأكسجین بصورة كافية إلى خلايا المخ و أنسجة الجسم، وذلك بسبب عدم قدرة المشیمة أو الرئة على القیام بعملیة تبادل الغازات في مرحلة ما حول الولادة، فیولد الطفل ولدیه:
· زیادة في حمضیة الدم ( ph < 7.45).
· مقیاس أبجار(Apgar score) أقل من 3 فى الدقيقة الخامسة بعد الولادة.
· تشنجات
· اضطرابات بوظائف أجھزة الجسم المختلفة
ویعتبر الاختناق الولیدي من أھم أسباب التأذي الدماغي عند حدیثي الولادة. وبحسب درجة الاختناق قد تحدث وفاة، شلل دماغي، أو إعاقة ذھنیة، أوقد ینجو الطفل في بعض الأحیان. ومن ھنا تأتي أھمیة إنعاش القلب فور الولادة، وذلك لتلافي مخاطر الاختناق التي قد یتعرض لھا.
الأسباب :
أولاً: أسباب خاصة بالأم أثناء الحمل أو الولادة
1. عوامل تؤدي إلى نقص كمیة الدم الواردة للجنین عن طريق المشيمة
▘ الانفصال المبكر أو الأوضاع الغیر طبیعیة للمشیمة.
▘ التفاف الحبل السري وتعقده حول عنق الجنین .
▘ سقوط الحبل السرى.
▘ انفجار الرحم .
▘ الولادة المتعسرة .
2. عوامل نقص تركیز الأكسجین في دم الأم
▘ إصابة الأم بقصور في وظائف القلب، وظائف الرئة، أو بعض أمراض الجھاز العصبي .
▘ إصابة الأم بمرض الغدة الدرقية.
▘ إصابة الأم بمرض السكري .
▘ إصابة الأم بتسمم الحمل.
▘ إصابة الأم بالعدوى أثناء الحمل .
▘ تدخین الأم سلبیاً أو إیجابیاً أثناء الحمل.
▘ تناول الأم لبعض المھدئات أو الأدویة أثناء فترة الحمل بدون استشارة الطبیب.
ثانیًا: أسباب خاصة بالولید
o الطفل ناقص النمو.
o استنشاق العقي .
o صعوبة التنفس الشديدة.
o العيوب الخلقية للقلب المصحوبة بالزرقة.
o الأنيميا الناتجة عن النزيف الشديد أو تكسير كرات الدم الحمراء.
o الصدمة الولیدیة.
o الإصابة بالعدوى والتسمم الدموي .
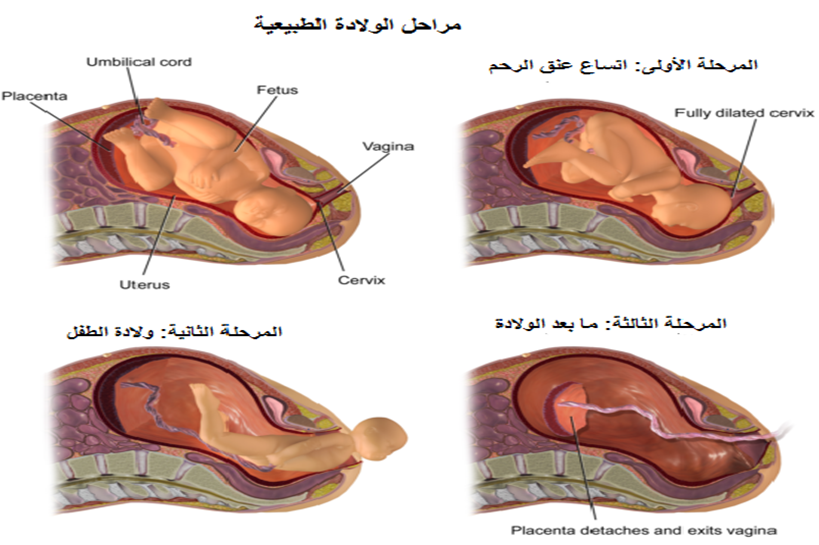
يأتى الأختناق الوليدى نتيجة طول المرحلتين الأولى والثانية من الولادة أكبر من 20 ساعة للحمل الأول وأكثر من 14 ساعة للنساء اللاتي لديهن ولادة سابقة.
الأعراض :
ھناك عدة مؤشرات عند الولادة تدل على احتمالیة إصابة الولید بالاختناق مثل:
· تلون السائل الأمنیوسي بالعقي
· انخفاض مقیاس أبجار
· زرقة أو شحوب بلون الجسم
· اضطراب في التنفس وبطء في خفقان القلب
· تشنج أو ارتخاء عضلات الجسم
درجات الاختناق الولیدي :
الدرجة الأولي – ویمیزھا :
· وجود فترات من زیادة الیقظة والھیاج، مع ظھور رعشة أو حركات غیر طبیعیة على الولید أو حدوثها تلقائيا.
· زیادة رد الفعل الانعكاسي مورو (Moro reflex)
· ضعف المص .
· زیادة معدل ضربات القلب .
· اتساع حدقتي العین.
· لا توجود تشنجات في ھذه الدرجة .
· غالبًا تختفي ھذه الأعراض خلال ٢٤ ساعة.
الدرجة الثانیة – ویمیزھا :
· خمول
· ضعف رد الفعل الانعكاسي مورو
· ضعف أو فقد القدرة على المص
· انخفاض معدل ضربات القلب، وانخفاض ضغط الدم
· ضیق حدقتي العین
· ظھور التشنجات في ٥٠ -70 ٪ من الأطفال خلال ٢٤ ساعة بعد الولادة
الدرجة الثالثة – ویمیزھا :
· غیبوبة
· ارتخاء العضلات
· اختفاء رد الفعل الانعكاسي مورو
· فقد القدرة على المص
· حدوث نوبات توقف التنفس
· انخفاض معدل ضربات القلب، واستمرار انخفاض ضغط الدم
· التشنجات تكون غیر شائعة في ھذه الدرجة، ولكن إن وجدت، فلا تستجیب بسھولة للعلاج
· تصل نسبة الوفاة في ھذه المرحلة إلى حوالي ٥٠ ٪، والنسبة الباقیة تعاني من مضاعفات خطیرة
الفحوصات والتحالیل المعملیة :
· متابعة نسبة الجلوكوز بالدم
· تقییم مستوى الكالسیوم، والصودیوم، والماغنسیوم بالدم
· عمل تحلیل غازات الدم
· عمل صورة دم كاملة
· عمل موجات صوتیة على المخ، أشعة مقطعیة على المخ
العلاج :
1. إن منع حدوث الاختناق الولیدي ھو أفضل طرق العلاج، ویكون ذلك من خلال:
· توفیر الرعایة اللازمة للأمھات طوال فترة الحمل للإكتشاف المبكر للحالات التي لدیھا عوامل خطورة والتعامل معھا في مرحلة ما حول الولادة بصورة تضمن سلامة الأم و طفلها.
· تطبيق خطوات الإفاقة للأطفال حدیثي الولادة بكفاءة.
2. العلاج الداعم للمخ و أجهزة الجسم.
3. علاج التشنجات
4. العلاج باستخدام تبريد الجسم الكلى، و ذلك لوقاية المخ و الحد من مضاعفات الأعتلال المخى المتوسط و الشديد الناتج عن نقص وصول الأكسجين إلى خلايا المخ بسبب الأختناق، و ذلك عن طريق خفض درجة حرارة الجسم.
الرعایة التمریضیة :
· التأكد من أن المجري الھوائي مفتوح دائماً عن طريق وضع الولید في وضع التنشق، والتشفیط الصدري.
· الحفاظ على درجة حرارة الولید حول المعدل الطبیعي.
· إعطاء الأكسجین بالطریقة المناسبة حسب تعلیمات الطبیب.
· متابعة مستوى الجلوكوز في الدم.
· تجھیز وإعطاء المحالیل الوریدیة، حسب تعلیمات الطبیب.
· عمل خریطة سوائل لحساب الداخل والخارج، والتأكد من تجمیع وحساب كمیة البول.
· متابعة حدوث التشنجات وإبلاغ الطبیب فورًا، في حالة حدوثھا.
· متابعة التقييم العصبى لحالة الطفل من حيث: درجة الوعى، النشاط، وضع الطفل، قوة إنقباض العضلات، المص، رد الفعل الانعكاسي مورو، النبض، التنفس، حدقة العين.
