
Book
Respiratory System Disorders Care Guide
- Oxygen Therapy
Oxygen is used as an essential treatment for acute respiratory problems and to prevent the harmful effects that may result from inadequate oxygen delivery to the infant’s tissues, particularly the brain. Oxygen is considered a medical therapy for neonates suffering from respiratory distress; therefore, the oxygen flow rate and concentration must be administered strictly according to the physician’s orders. The nurse is responsible for continuous monitoring to prevent complications resulting from either insufficient or excessive oxygen therapy.
Indications for Use:
- Documented hypoxemia based on arterial blood gas (ABG) results.
- Postnatal resuscitation and cardiopulmonary resuscitation.
- Respiratory distress associated with cyanosis.
- Management of functional impairments of body systems resulting from reduced tissue oxygenation (shock).
- Recurrent episodes of apnea.
Signs of Hypoxemia:
- Increased respiratory rate
- Chest retractions
- Grunting during expiration
- Rapid, shallow breathing
- Recurrent episodes of apnea
- Cyanosis (bluish discoloration of the skin)
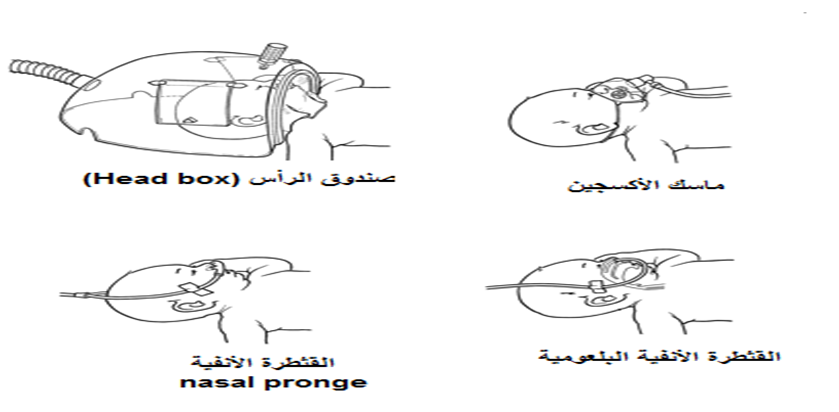
Methods of Oxygen Administration in Neonatal Care Units:
Oxygen may be administered to neonates using one of the following methods:
- Oxygen incubator
- Head box
- Face mask
- Nasal catheter / nasal prongs
- Nasopharyngeal catheter
- Nasal Continuous Positive Airway Pressure (NCPAP)
- Mechanical Ventilation via an Endotracheal Tube
• Different Methods of Oxygen Administration in Neonatal Intensive Care Units (NICUs), Oxygen Flow Rates (L/min), and the Advantages and Disadvantages of Each Method:
|
Method |
Oxygen Flow Rate (L/min) |
Advantages |
Disadvantages |
|
Oxygen Incubator |
6–10 L/min |
- Non-invasive and cost-effective method- Used during oxygen weaning |
- Ineffective in critically ill neonates |
|
Head Box |
4–7 L/min |
- Non-invasive method- Used during oxygen weaning |
- Poor seal with possible oxygen leakage- Difficult to provide adequate nursing care |
|
Face Mask |
3–6 L/min |
- Non-invasive- Simple and inexpensive- Used during postnatal recovery |
- Abdominal distension- Pressure on the face and eyes- Carbon dioxide retention |
|
Nasal Catheter (Nasal Prongs) |
0.5–2 L/min |
- Non-invasive- Effective in some cases of respiratory distress |
- Abdominal distension- Nasal injury |
|
Nasal Continuous Positive Airway Pressure (NCPAP) |
8–10 L/min (oxygen + compressed air) |
- Non-invasive- Effective in severe respiratory distress |
- Abdominal distension- Severe nasal septum injury- High cost |
|
Mechanical Ventilation via Endotracheal Tube |
As prescribed by the physician |
- Effective in severe respiratory distress associated with respiratory failure |
- Invasive method- Risk of respiratory tract infection- Requires advanced nursing care and high-level medical skills- Requires advanced technology (Level III neonatal care facilities)- High cost |
Nursing Care for Neonates on Oxygen Therapy
- Observe and record skin color, respiratory effort, and vital signs, and notify the physician immediately if any abnormalities occur.
- Continuous monitoring of oxygen saturation (SpO₂) using a pulse oximeter, maintaining levels between 89–93%, or as prescribed by the physician.
- Administer humidified oxygen to prevent drying of the airway mucosa, which can increase secretion viscosity and accumulation.
- Observe and record the oxygen flow rate, the method of oxygen delivery, and the oxygen saturation level.
- Suction the airway as needed, documenting the amount and characteristics of secretions removed.
- Perform arterial blood gas (ABG) analysis to assess oxygenation and acid-base status.
- Monitor oxygen concentration using an oxygen analyzer if available, to prevent complications from excessive oxygen delivery.
Complications Due to Hypoxia (Low Oxygen):
- Increased pulmonary artery pressure
- Seizures
- Hypoxic encephalopathy
- Cerebral palsy
- Long-term cognitive and behavioral impairments
Complications Due to Hyperoxia (Excess Oxygen):
- Retinopathy of prematurity and potential vision loss, especially in preterm or low-birth-weight neonates
- Oxygen dependency of the lungs and difficulty weaning from oxygen (chronic lung disease)
- Pneumothorax, particularly with NCPAP or mechanical ventilation
