
Book
Respiratory System Disorders Care Guide
- Nasal Continuous Positive Airway Pressure (Nasal CPAP)
Nasal CPAP is a non-invasive, safe ventilatory support system that does not require an endotracheal tube. It delivers a continuous positive pressure of oxygen-enriched air to keep alveoli open and prevent collapse during exhalation. It can be delivered via mask, nasopharyngeal catheter, or endotracheal tube, though nasal CPAP is the most commonly used.
Indications
- Respiratory distress from Hyaline Membrane Disease in preterm neonates due to surfactant deficiency, to improve lung efficiency and reduce the need for invasive ventilation.
- PaO₂ < 50 mmHg despite oxygen therapy ≥60% using simpler methods.
- Moderate respiratory distress: tachypnea (>60 breaths/min), grunting, or subcostal retractions, such as:
- Transient neonatal tachypnea
- Meconium aspiration
- Apnea of prematurity in low birth weight infants.
- Post-weaning from mechanical ventilation.
Contraindications
- Respiratory failure requiring invasive ventilation.
- Persistent apnea with bradycardia unresponsive to CPAP.
- Upper airway malformations (cleft palate, nasal obstruction).
- Diaphragmatic hernia.
- Severe, unstable cardiac disease.
Nasal CPAP Components
- Gas Source: Provides a humidified mixture of oxygen and compressed air.
- Pressure Generator: Creates continuous positive airway pressure.
- Interface: Connects the circuit to the neonate’s airway (nasal prongs or mask).
Circuit Components
- Gas Delivery Circuit:
- Oxygen and compressed air inlets.
- Oxygen blender to mix oxygen and air to the required FiO₂.
- Flowmeter (8–10 L/min) and manometer to monitor pressure.
- Humidifier: Heats and humidifies the inspired gas with a temperature sensor.
- Pressure Generator: Maintains continuous positive pressure at the end of exhalation to keep alveoli open.
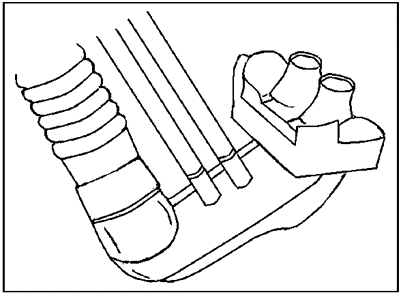
Positive Pressure Generator (CPAP Generator)
Other Methods to Generate Positive Pressure (Bubble–CPAP)
- Immerse the free end of the exhalation tube under the water surface to a depth of 5 cm to generate the desired positive pressure in the alveoli.
- Attach a graduated measuring tube to the outer wall of the sterile water bottle.
- Fill the bottle with sterile water until the water level reaches 7 on the measuring tube.
- Immerse the tube end under the water to 5 cm, leaving a 2 cm gap between the tube end and the bottom of the bottle to prevent excessive alveolar pressure.
- Ensure the appearance of air bubbles after connecting the neonate and starting the CPAP device.
- Connect the device’s exhalation tube to a valve.

Nasal Prongs (Double-Prong Catheter)
- Connection: Attaches to the end of the generator to deliver the inhaled gas circuit to the infant.
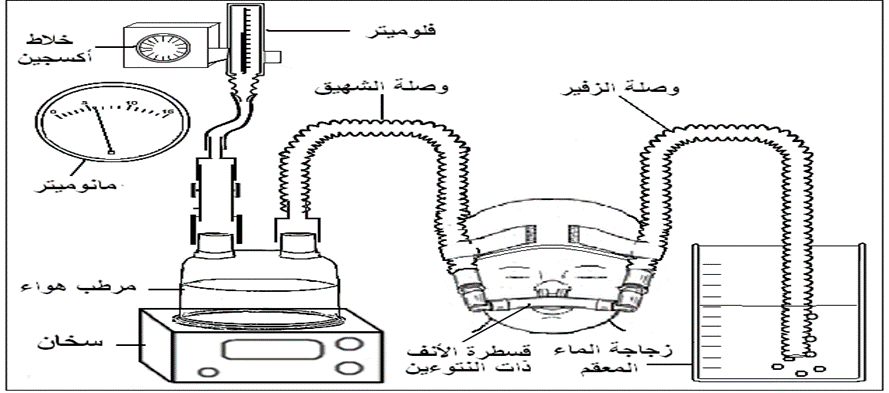
Device Connections
- Short Corrugated Tube: Connects the flow meter (on the oxygen blender) to the humidifier.
- Inhalation Tube: A long corrugated tube carrying the humidified inhaled gas from the humidifier to the positive pressure generator and the double-prong nasal tube, delivering warm, moist air to the infant.
- Exhalation Tube: A corrugated tube connecting the double-prong nasal tube to the positive pressure generator at the back, connected to a manometer to monitor the generated pressure.
(Bubble CPAP)
Nurse’s Role:
The device must always be ready for use at any time in the neonatal care units, with all necessary connections available, including all sizes of double-prong nasal catheters according to the infant’s weight and gestational age.
Preparing the Infant for Connection to the Device
- Infection Control: Follow strict infection control measures to prevent respiratory infections and ensure the device functions efficiently:
- Wash hands thoroughly before handling the device, catheter, or infant.
- Wear sterile gloves during airway suctioning.
- Keep all tubing off the floor or away from contamination sources.
- Device Setup:
- Connect the oxygen and air supply to the oxygen blender, adjusting the oxygen flow rate to 8–10 L/min.
- Set the oxygen concentration to the required percentage.
- Connect the short corrugated tube to the oxygen humidifier and insert the temperature probe into the designated port.
- Fill the humidifier with sterile water to the marked level, turn on the device, and set the temperature to 37°C.
- Select the appropriate cap size for the infant’s head.
- Select the correct nasal catheter size by measuring the infant’s nostrils; proper fit is crucial:
- Too small → leakage, difficult to maintain pressure.
- Too large → nasal mucosal injury.
- Attach the nasal catheter to the generator and temporarily cover with a finger to check that the manometer shows the correct pressure (5 cm H₂O).
Connecting the Infant to the Device
- Wash hands or use alcohol rub.
- Ensure no obstruction in the infant’s posterior nasal passages (congenital defect in some cases).
- Connect the infant to the monitoring system (oxygen saturation and vital signs).
- Wear gloves.
- Suction the nose, mouth, and pharynx using the largest catheter that can pass without resistance.
- Positioning: Raise the bed 30°, place a folded sheet under the infant’s shoulders, slightly extend the neck to keep the airway open.
- Place the appropriately sized cap, bending its edge 2–3 cm above the ears.
- Insert the double-prong nasal catheter and secure with the cap’s attached strings, ensuring:
- Catheter fills both nostrils completely.
- Skin around the nose is not under tension.
- Catheter does not press on the nasal septum.
- Space between the septum tip and the catheter bridge.
- Catheter does not rest on the upper lip.
- Secure the exhalation corrugated tube to the forehead via cap straps.
- Insert a gastric feeding tube for stomach suction, connecting it to a syringe to release excess air.
- Clean the upper lip and cheeks with warm water, dry, and apply prescribed moisturizer to prevent pressure sores.
Monitoring the Infant on the Device
- Check every 2–4 hours:
- Respiratory status: rate, nasal flaring, chest retractions, breath sounds.
- Body temperature.
- Circulation: capillary refill, blood pressure, heart rate.
- Neurological status: activity, movement, reflexes.
- Gastrointestinal: abdominal distention.
- Monitor devices for proper function.
- Suction as needed (nose, mouth, pharynx, stomach). Shorter suction intervals (<2 hours) may be needed if:
- Increased respiratory effort.
- Higher oxygen requirements.
- Apnea or bradycardia episodes.
- Record volume and color of secretions.
- Verify device function via checklist.
- Reposition infant every 4–6 hours to prevent secretion accumulation.
- Drain and dispose of condensation in tubing regularly.
Weaning from Nasal CPAP
Indicators for weaning:
- Overall improvement in the infant’s condition.
- Spontaneous, comfortable breathing.
- Reduced respiratory rate, absence of chest retractions, improved color.
Weaning Steps:
- Gradually reduce oxygen concentration by 2–5% at a time until reaching 21%, guided by pulse oximetry or arterial blood gas analysis.
- Temporarily remove the nasal catheter and observe:
- Increased breathing rate.
- Chest retractions.
- Decreased oxygen saturation.
- Apnea episodes.
- Cyanosis.
- If any signs appear → weaning fails; resume CPAP and attempt again after 24 hours.
- Do not attempt weaning if alveolar collapse is likely, as prevention is better than treatment.
Feeding During Nasal CPAP
- If stable, feed via the gastrointestinal tract using gravity or syringe pump.
- Suction excess stomach air before feeding.
Potential Complications of Nasal CPAP
- Nasal septum injuries from prolonged catheter pressure.
- Skin injuries from device straps.
- Abdominal distention.
- Increased secretions.
- Pneumothorax.
Checklist for Neonatal NCPAP Monitoring (Filled by Responsible Nurse Each Shift)
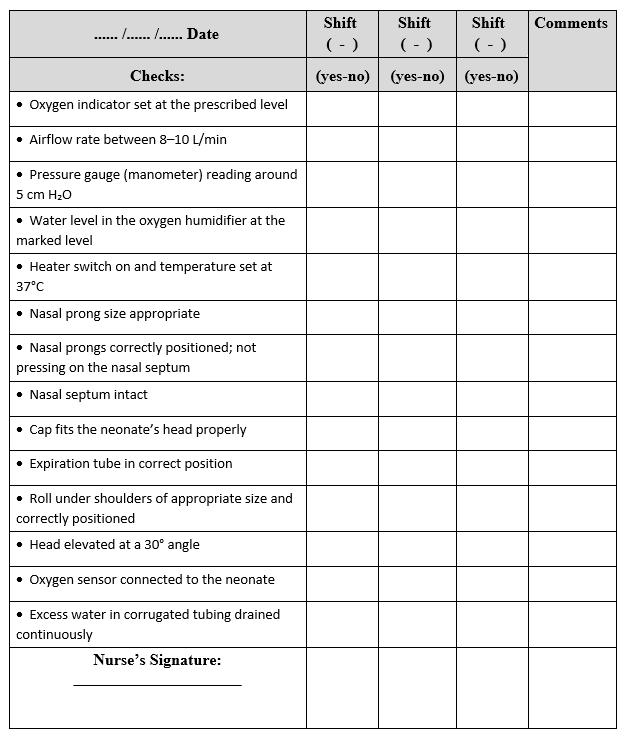
Checklist for Preparing the Neonatal Continuous Positive Airway Pressure (NCPAP) System
|
Date ....../ ....../ ...... |
Shift ------ |
Shift ------ |
Shift ------ |
Comments |
|
Check |
Yes / No |
Yes / No |
Yes / No |
|
|
Nasal CPAP device ready for use |
||||
|
Sufficient number of connections and various sizes of nasal prongs available |
||||
|
Sterile water bottles available |
||||
|
Oxygen humidifier ready for use |
||||
|
Nurse’s signature: |
