
Book
Guidelines for Obstetrics and Gynecology Nursing Procedures
- Cesarean Section (C-Section)

- Introduction
- Definition
- Reasons for Performing a Cesarean Section
- Types of Cesarean Delivery
- Risks
- Risks for the Mother
- Risks for the Baby
- Procedure
- Prevention of Complications
- Post-Cesarean Nursing Care
Introduction
Cesarean section (C-section) is a major surgical procedure. While it can be life-saving for both the mother and the baby, it is also associated with some side effects that may take a long time to recover from. Physicians estimate that complete recovery from a C-section takes about 4 to 6 weeks, but many studies suggest that the total recovery time may be longer. It is important to note that the duration of recovery varies from one woman to another. However, a mother can recover more quickly by focusing on self-care, taking care of her baby, allowing her body the necessary rest, and receiving proper medical care.
Definition
A Cesarean section is a surgical procedure in which the doctor makes an incision in the abdomen and uterus to extract the baby. In some cases, the procedure is planned in advance, while in others, it becomes necessary during labor.
A Cesarean section is a type of non-vaginal birth, in which the surgeon performs a surgical incision in the abdomen and uterus to deliver the baby when vaginal delivery is not possible.
Reasons for Performing a Cesarean Section
Not all of the following conditions require a C-section, but the procedure is performed when vaginal delivery is not possible or carries risks for the mother or baby. The primary reasons for a Cesarean section include:
Maternal Reasons:
- Post-term pregnancy: If the pregnancy exceeds 40 weeks without the onset of labor.
- Prolonged labor (failure to progress): One of the most common reasons for a Cesarean section. The cervix may fail to dilate adequately despite strong contractions lasting several hours.
- Presence of maternal health conditions, such as:
- Severe heart disease
- HIV infection
- Preeclampsia or severe hypertension, which poses a risk to the mother’s health
- Sexually transmitted infections (e.g., herpes), which could be transmitted to the baby during vaginal delivery
- Mechanical obstruction in the birth canal, such as:
- Large fibroid tumors blocking the birth canal
- Severe pelvic fractures, leading to a narrow birth canal
- Uterine rupture
- Failure of assisted vaginal delivery (forceps or vacuum extraction). If these methods fail, a Cesarean section is required.
- Previous uterine rupture
- Previous classical (vertical) Cesarean section
- Poor perineal healing from previous childbirth or Crohn’s disease
- Bicornuate uterus
- Rare cases of postmortem childbirth
- Maternal exhaustion and inability to actively participate in labor
Fetal Reasons:
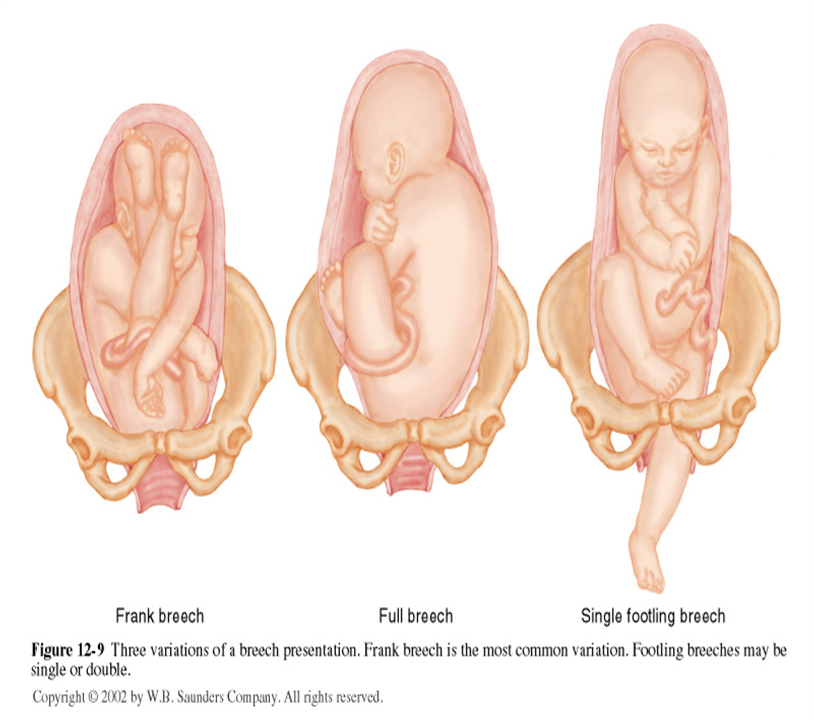
- Abnormal fetal positioning: If the baby or babies are in an abnormal position, making vaginal delivery impossible. These include:
- Breech presentation (buttocks or feet first)
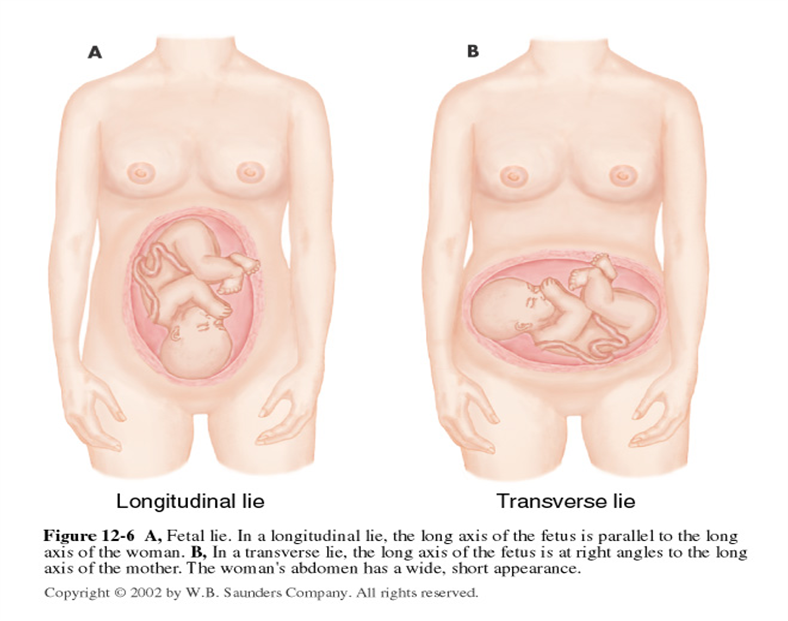
- Transverse lie (baby positioned sideways)
- Shoulder presentation (shoulder enters the birth canal first)
- Fetal Macrosomia: If the baby is large and weighs more than 4 kg, making it disproportionate to the mother’s pelvis.
- Umbilical Cord Issues: Such as vasa previa (abnormal fetal blood vessels crossing the cervix) or umbilical cord prolapse.
- Multiple Pregnancies: If the pregnancy involves more than one baby and the first fetus is in an abnormal position, or if the pregnancy involves three or more fetuses.
- Fetal Oxygen Deficiency: If the baby is not receiving enough oxygen, indicated by abnormal fetal heart rate patterns.
- Severe Hydrocephalus: A condition in which the baby’s head becomes abnormally large due to fluid accumulation.
- Umbilical Cord Prolapse: If a loop of the umbilical cord slips through the cervix before the baby.
Placental Causes:
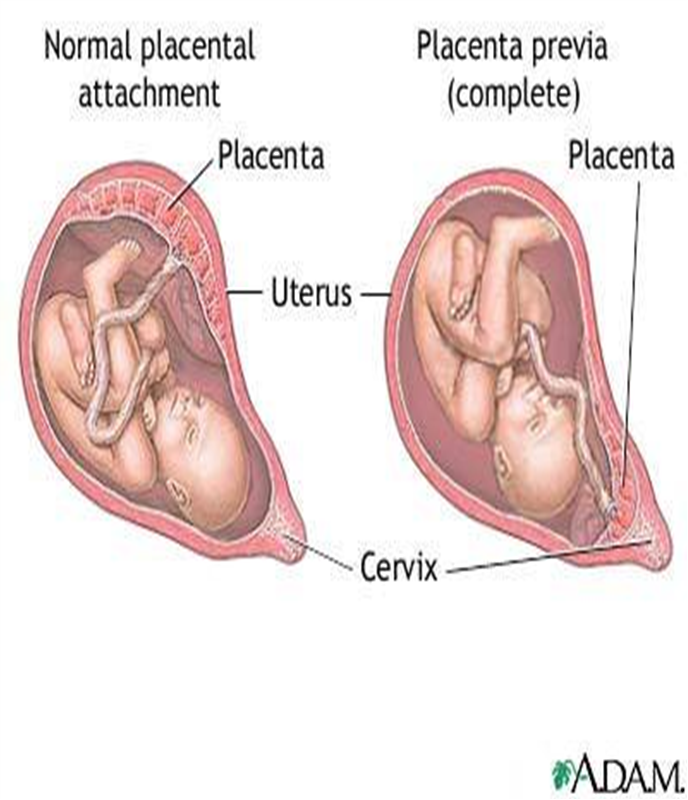
- Placental Problems:
- Placenta previa: When the placenta covers the cervical opening.
- Placenta accreta: When the placenta abnormally attaches to the uterine wall.
Other Reasons:
- Lack of obstetric skills: In some cases, obstetricians may lack the skills to perform breech deliveries or manage multiple births. While most women can still deliver vaginally under these conditions, a planned Cesarean section carries a lower risk of infant mortality in breech deliveries compared to vaginal birth.
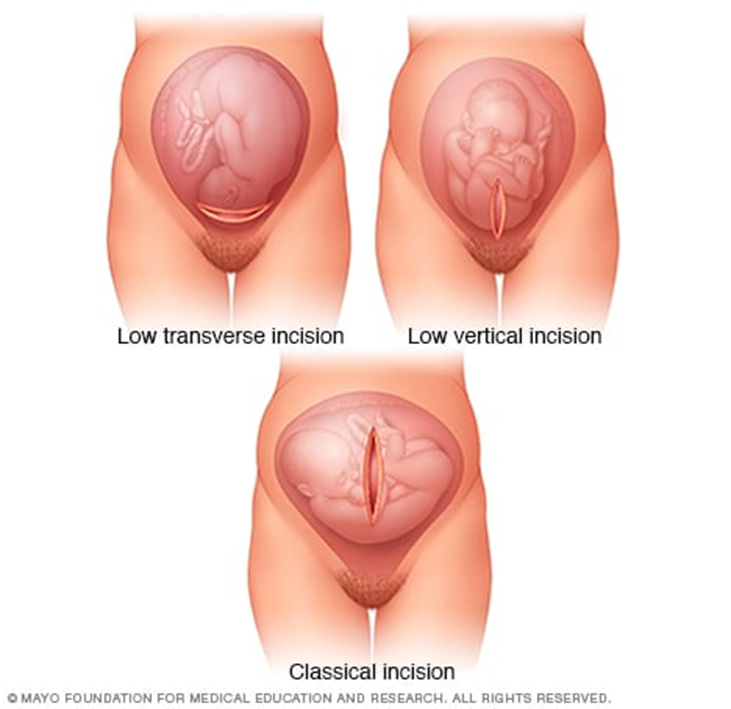
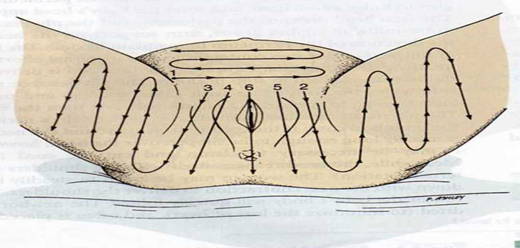
Types of Cesarean Delivery
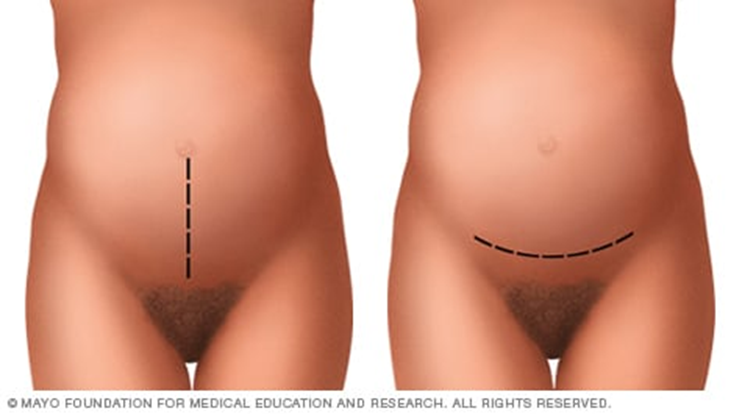
1. Classic Cesarean Section:
- Involves a long, vertical incision in the middle of the abdomen, with both the skin and uterus being cut vertically to extract the baby.
- This method is rarely used today due to the larger incision size and higher risk of complications, such as:
- Increased risk of hernia years after surgery due to weakened abdominal wall muscles.
- Unsafe for vaginal delivery in future pregnancies.
2. Low Transverse Incision (Horizontal Incision):
- The most common type of Cesarean section.
- A horizontal incision is made along the pubic hairline, just above the bladder, reaching the uterus.
- The doctor then inserts their hand to pull the baby out.
- This method allows for faster recovery and has a lower risk of complications.
- Future vaginal delivery remains possible with this type of incision.
3. Low Vertical Incision:
- Similar to the classic Cesarean section, but the incision is made lower than in the classic method.
- This technique is used in cases where the fetus is positioned abnormally in the uterus.
Procedure
This surgery typically takes 30–40 minutes and is performed by an obstetrician immediately after the anesthesia takes effect, as follows:
- Under general or regional anesthesia, depending on the woman's health condition, a surgical incision is made in the lower abdomen, just above the pubic area. The surgeon then cuts through the skin layers, subcutaneous tissues, abdominal muscles, and uterine wall to reach the uterus.
- The baby is quickly delivered, followed by clamping and cutting of the umbilical cord, and the removal of the placenta.
- The surgeon stitches the uterine wall with strong, long-lasting sutures, then proceeds to suture the abdominal wall, muscles, and skin layers.
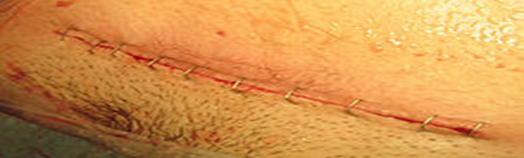
- The skin incision is closed using surgical staples, and a dressing is applied to the wound.
Risks of Cesarean Section
Risks for the Mother
- Since most women undergoing a C-section have severe health conditions, it is often difficult to determine whether the cause of maternal mortality is the surgery itself or the underlying condition. However, the risks of serious complications such as cardiac arrest, hematomas, and organ removal are present, as with all major abdominal surgeries.
- Higher risk of complications in future pregnancies compared to women who have had only vaginal deliveries.
- Adhesions: Formation of scar tissue between the uterus, ovaries, small intestine, or any other abdominal or pelvic tissues, which may cause:
- Infertility: Adhesions can block the fallopian tubes, preventing the egg from reaching the uterus.
- Chronic pelvic pain: Adhesions in the pelvic area can lead to long-term discomfort.
- Small bowel obstruction: Adhesions can disrupt normal intestinal movement, leading to complications in approximately 50% of cases.
- Infections: A C-section increases the risk of endometritis (infection of the uterine lining).
- Postpartum hemorrhage: Severe bleeding can occur during or after surgery.
- Anesthesia complications: Adverse reactions to general or regional anesthesia.
- Blood clots: Increased risk of deep vein thrombosis (DVT), particularly in the legs or pelvic area. If a clot travels to the lungs, it can cause a pulmonary embolism, a life-threatening condition.
- Surgical site infections: The risk of wound infection depends on individual risk factors and whether the C-section was an emergency.
- Surgical injuries: Although rare, bladder or bowel injuries can occur during the procedure, potentially requiring additional surgery.
- Increased risk in future pregnancies: Women with previous C-sections have a higher risk of placenta previa (placenta covering the cervix) and placenta accreta (abnormal placenta attachment), which may necessitate hysterectomy.
- Uterine rupture: The risk of uterine rupture along the previous C-section scar increases if a woman attempts vaginal birth after Cesarean (VBAC).
Risks for the Baby
- Preterm birth risks: Delivering before 39 weeks of gestation for non-medical reasons poses serious risks to the baby, including:
- Increased fetal mortality rates.
- Respiratory problems: Babies born via scheduled C-sections are at higher risk of transient tachypnea of the newborn (TTN) or respiratory distress syndrome, requiring respiratory support and admission to neonatal intensive care.
- Low oxygen levels if there is a delay in performing the C-section.
- Surgical injury: Accidental scratches or cuts to the baby’s skin during surgery, though rare.
- Higher infant mortality rate in early childhood due to complications from preterm birth.
Prevention of Complications
- Antibiotic prophylaxis is effective in reducing the risk of endometritis, urinary tract infections, and surgical site infections, preventing 3 out of 4 cases of post-C-section infections.
- Some physicians believe that manually or instrumentally dilating the cervix during a C-section helps prevent lochia (postpartum fluid) retention, reducing the risk of maternal morbidity and mortality.
Post-Cesarean Nursing Care
After a Cesarean section, the patient is transferred from the operating room to a recovery unit, where healthcare providers monitor her condition as follows:
1. Vital Signs Monitoring:
- Blood pressure, respiratory rate, and pulse are assessed periodically every 4 to 6 hours postpartum.
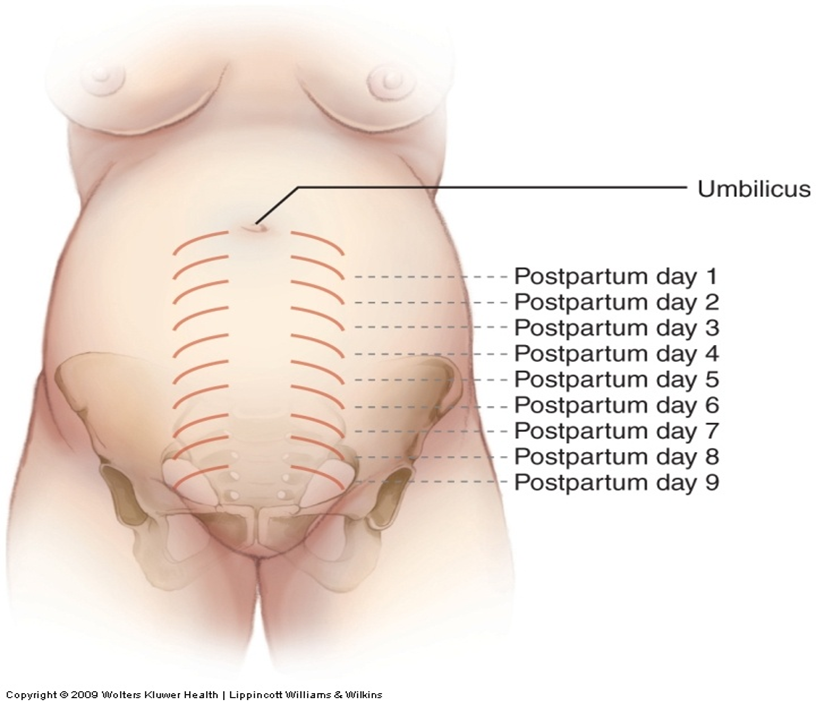
2. Uterine Assessment:
- Consistency: The uterus should be firm, contracted, and spherical.
- Size:
- At the end of the first week, the uterus weighs 500 grams.
- By the end of the second week, it decreases to 350 grams.
- Between weeks two and six, it returns to its normal size of 50–60 grams.
- Position: To be evaluated during postpartum care.
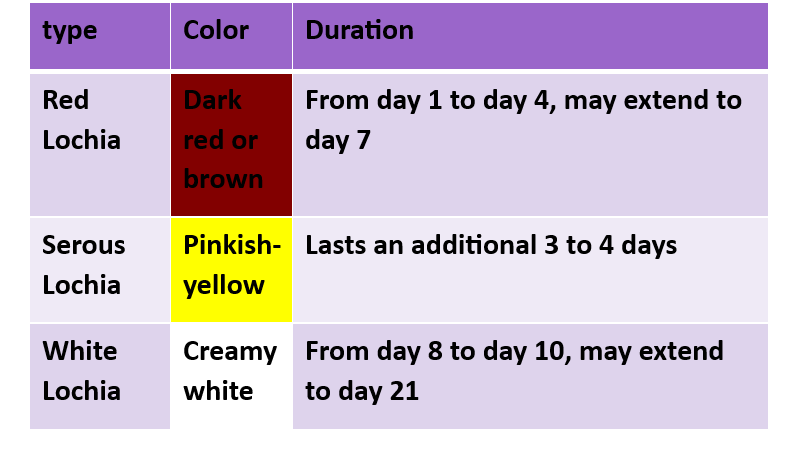
▶️ Lochia (Postpartum Bleeding) Monitoring:
- Assess the amount to detect any postpartum hemorrhage.
1.Very light bleeding: Less than 10 mL per hour.
2. Mild bleeding: Between 10 to 25 mL per hour.


- Moderate bleeding: 25 to 50 mL per hour.
- Heavy bleeding: More than 50 mL per hour.
- Observe the type and color of lochia.


Postpartum Observations
3. Pain Monitoring:
- The woman may experience abdominal cramps similar to menstrual pain due to uterine contractions, which help the uterus return to its normal size and position.
4. Bowel Movement Monitoring:
- Postpartum women often experience constipation due to fasting before surgery, anesthesia, and abdominal muscle relaxation after childbirth.
5. Urination Monitoring:
- After delivery, women lose stored body fluids through excessive sweating (especially at night) and urination.
- 2500–3000 mL of urine should be excreted in the first few hours after birth.
- Monitoring fluid intake and output is essential to prevent fluid retention.
6. Lower Limb Monitoring (Legs):
- Watch for signs of deep vein thrombosis (DVT), such as swelling, redness, and warmth, as postpartum women are at higher risk of blood clots.
7. Breast Examination:
- Assess breast size and condition for successful breastfeeding and milk production.
8. Incision Site Assessment:
- Check the wound dressing for bleeding or signs of infection.
- Observe for surgical drains (e.g., Redivac drain) if present.
Emotional Well-Being
Postpartum Emotional Changes:
- Difficult emotional experience.
- Anxiety, sadness, frustration, and fatigue.
- Postpartum blues (baby blues).
- Postpartum depression.
Symptoms:
- Negative emotions lasting beyond two weeks.
- Impact on infant care.
- Need for emotional support from family and friends.
- Seeking professional psychological help.
- Openly expressing feelings.
Early Treatment:
- Observation.
- Postpartum depression is not a weakness.
- It is treatable.
- Emotional support aids recovery.
Postpartum Care for Women
1. Early Mobilization:
- The woman should get out of bed and walk within 24 hours of surgery, once anesthesia wears off.
- This helps reduce pain, prevent blood clots, stimulate bowel movement, and relieve gas pain.
- Painkillers may be given for post-surgical pain.
- Fatigue or nausea may occur due to anesthesia.
- Sufficient fluid intake is recommended to prevent deep vein thrombosis (DVT) and constipation.
2. Urinary Catheter Removal:
- If a urinary catheter was used, it should be removed as soon as possible.
- Typically, the catheter remains for about 24 hours post-surgery since it may be difficult for the woman to use the bathroom immediately due to anesthesia effects.
3. Incision Monitoring:
- The surgical wound should be regularly checked for infection or bleeding.
- The incision should remain covered with a dressing for at least 24 hours.
4. Eating and Drinking:
- The woman can eat and drink as soon as she feels hungry or thirsty.
- In some cases, she may need to wait a few hours until gas or bowel movement occurs, ensuring proper intestinal function.
5. Personal Hygiene:
- Perineal care should be performed using antiseptic solutions as instructed.
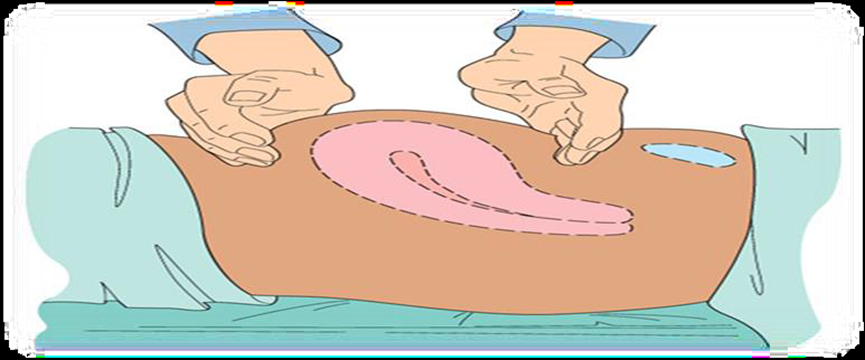
1. Uterine Condition Monitoring and Fundal Massage:
Perform fundal massage every 15 minutes during the first hour after delivery.
Then, perform fundal massage every 2 hours thereafter.
1.الرضاعة الطبيعية


Direct Mother-Baby Contact During Hospital Stay
A mother can begin breastfeeding almost immediately after a Cesarean section. The body produces breast milk as quickly as it does after a vaginal birth. However, certain factors should be considered when breastfeeding, including:
· Breastfeeding Positioning: Finding a comfortable position may be challenging due to the surgical incision site. Using a pillow placed over the abdomen can help reduce the pressure from the baby’s weight. The following positions are recommended:
- Football Hold: The baby’s neck is supported by the mother’s hand, with the rest of the body positioned along her arm. The baby’s legs and feet tuck under the mother's arm, while the baby is lifted to chest level for feeding.
- Side-Lying Position: The mother lies on her side, facing the baby, and uses her hand to guide the breast toward the baby’s mouth. A pillow can be placed behind the baby’s back to prevent rolling over.

