
Book
Guidelines for Obstetrics and Gynecology Nursing Procedures
- Gynecological Surgeries
Dilation and Curettage (D&C) Procedure
Definition:
Dilation and Curettage (D&C) is a minor surgical procedure in which the cervix is dilated (opened) to carefully remove tissue from the inside of the uterus. The tissue may be removed using suction or a metal instrument called a curette.
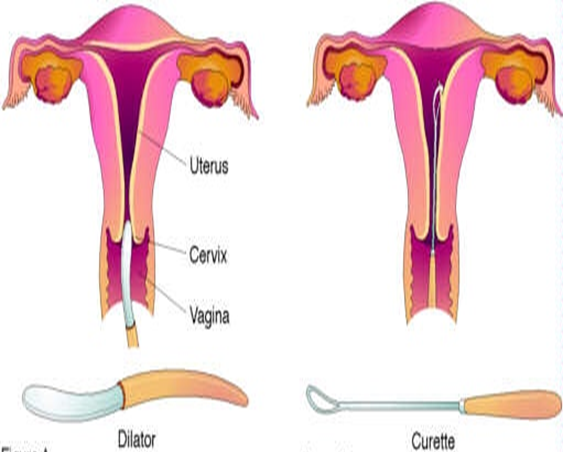
Body Parts Involved
- Vagina
- Cervix
- Uterus
Where is D&C Performed?
Dilation and curettage (D&C) can be performed in a doctor’s office, surgical center, or hospital.
Indications for D&C
D&C is a common gynecological procedure used for both diagnostic and therapeutic purposes.
Diagnostic Indications:
- Cervical canal obstruction.
- Intrauterine adhesions.
- Endometrial biopsy to detect conditions like tuberculosis or malignancies of the cervix.
- Initial step before procedures such as uterine evacuation.
- Determining ovulation timing in cases of infertility.
- Investigating amenorrhea (absence of menstruation).
Therapeutic Indications:
- Removal of polyps or large tissue masses.
- Emptying the uterus in pregnancy-related cases.
- Incomplete miscarriage management.
- Removal of pregnancy remnants.
- Evacuation of a molar pregnancy.
- Treatment of severe menstrual pain.
- Infertility due to cervical stenosis.
- Drainage of accumulated blood.
- Removal of an intrauterine contraceptive device (IUD).
Absolute Contraindications
- Desired intrauterine pregnancy.
- Inability to visualize the cervical opening.
- Obstructed vagina.
Permanent Contraindications
- Severe cervical stenosis.
- Cervical or uterine malformations.
- Previous endometrial destruction.
- Bleeding disorders.
- Acute pelvic infection (except for removing infected endometrial contents).
- Obstructive cervical tumor.
D&C Procedure
Preparation for D&C – Required Supplies:
- Betadine solution.
- Sterile gauze.
- Formalin container for biopsy samples.
- Sterile gloves (various sizes).
- Sterile pack for draping and surgical gowns.
- Sterile instrument tray.
- Nelaton catheter.
Surgical Instruments (16 Tools):
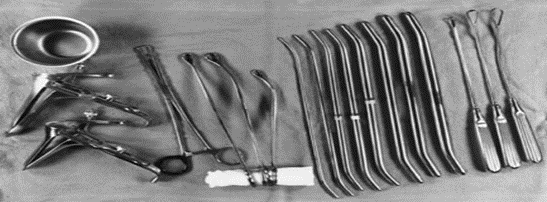
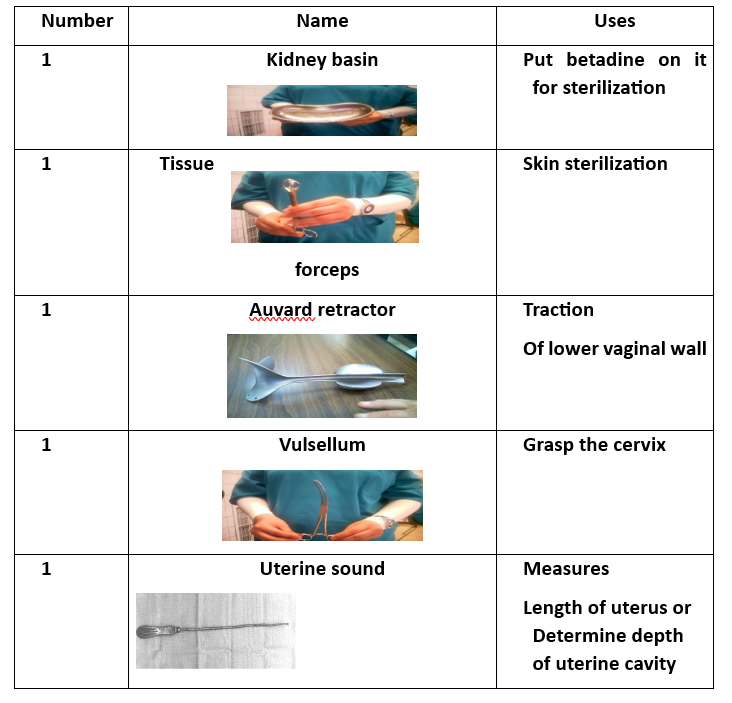
- Instrument Tray (for collecting tools).
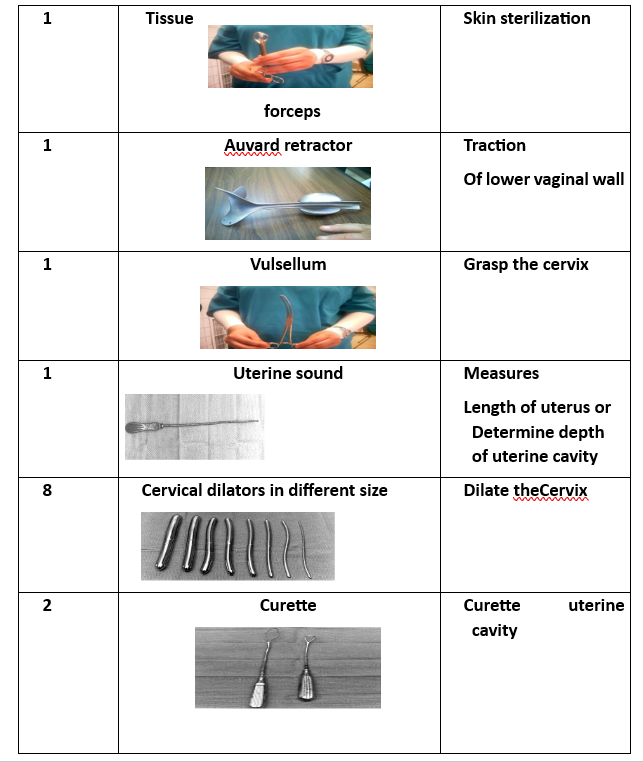
- Tissue Forceps.
- Auvard Speculum (self-retaining vaginal retractor).
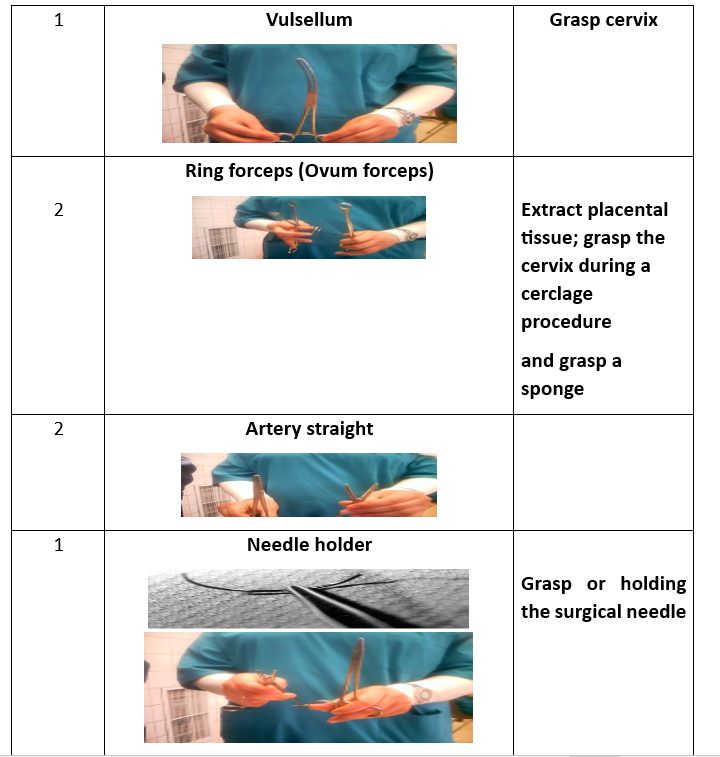
- Cervical Tenaculum (Vulsellum Forceps).
- Uterine Sound (for measuring uterine depth).
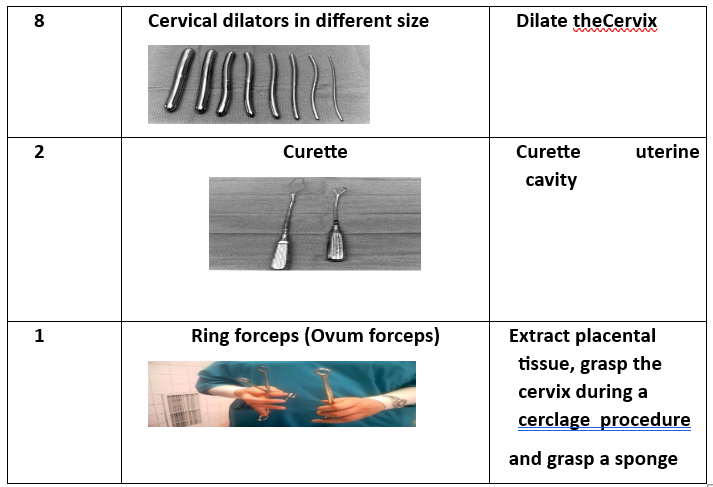
- 8 Cervical Dilators (various sizes).
- Curette (2 pieces) (for scraping uterine lining).
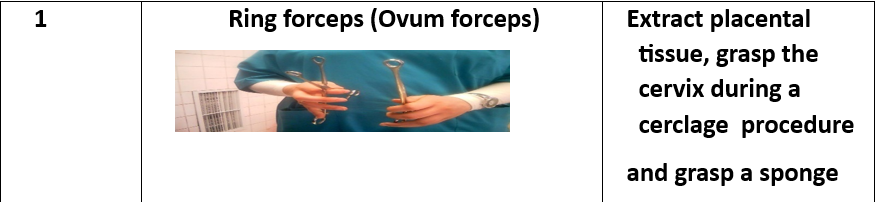
- Ovum Forceps (for grasping uterine contents).
D&C Procedure Steps
- Preparation of Surgical Supplies.
- Manual examination to assess the uterine condition.
- Bladder emptying using a metal catheter.
- Insertion of the Auvard speculum into the vagina.
- Identification of the cervix and securing it with a vertical tenaculum.
- Measurement of uterine cavity depth using a uterine sound.
- Cervical dilation if necessary, using dilators of varying sizes.
- Uterine curettage to remove its contents completely. The presence of air bubbles in vaginal blood is a positive sign indicating an empty uterus. Ovum forceps may also be used for uterine evacuation by grasping and rotating the tissue.
- Collection of endometrial tissue samples for biopsy analysis.
- Cleaning the perineal area with Betadine, placing a sanitary pad, and removing surgical instruments.
Common Complications
- Unusual pain.
- Fever.
- Secondary amenorrhea in reproductive years.
Rare Complications
- Infection or septicemia.
- Neurogenic shock.
- Uterine perforation (a tear in the uterine wall), which may occur during sound insertion, dilation, or curettage.
- Cervical rupture, potentially leading to cervicitis and hemorrhage.
- Asherman’s syndrome (intrauterine adhesions).
- Permanent amenorrhea due to excessive removal of the basal endometrial layer.
Nursing Care
Preoperative Preparation
1. Assessment:
- Obtain complete medical history and explain the procedure to the patient.
- Perform a physical examination.
- Conduct diagnostic tests, including CBC, blood type and Rh factor, urinalysis, and fluid balance evaluation.
2. Patient Preparation:
- Ensure the patient understands the procedure, risks, and benefits.
- The patient should fast for 6 hours before surgery.
- Remove jewelry and metallic objects.
- Bowel preparation via enema.
- Bladder preparation (catheterization if needed).
- Monitor vital signs.
Postoperative Nursing Care
- Hospital observation for 1 to 4 hours.
- Monitor vaginal bleeding.
- Assess consciousness level.
- Monitor vital signs and position.
- Administer oxytocin to ensure uterine contraction and minimize bleeding.
- Monitor intravenous fluids (type and rate).
- Assess pain and cramps and provide pain relief as prescribed.
- Administer antibiotics as needed.
- Blood transfusion may be required in cases of shock or anemia.
- If the patient is Rh-negative, administer Rh immunoglobulin (RhoGAM) within 72 hours post-miscarriage.
- Report persistent severe pain.
- Maintain perineal hygiene.
- Monitor the amount and color of vaginal bleeding.
Patient Education for Post-D&C Discharge
- Referral to professional support groups if needed.
- Advise the patient to report:
- Heavy, bright red, or foul-smelling bleeding.
- Slight, dark discharge may continue for up to two weeks.
- Instruct the patient to avoid inserting anything into the vagina (e.g., tampons, douching, sexual intercourse) until bleeding stops.
- Inform about possible mood swings and depression.
- Avoid pregnancy for at least one year after a D&C procedure.
- Seek medical help if experiencing:
- Fever, abdominal pain, heavy bleeding, or foul-smelling vaginal discharge.
Cervical Cerclage
Definition:
Cervical cerclage is a surgical procedure performed on pregnant women with an incompetent cervix to strengthen it using a suture (nylon tape).
Types of Cervical Cerclage Procedures:
- McDonald Technique – Performed on women with a normal cervix.
- Shirodkar Technique – Performed on women with a short cervix.
Timing of Cervical Cerclage:
- Before 12 weeks of pregnancy: Procedure is performed vaginally.
- After 12 weeks of pregnancy: Procedure is performed abdominally.
Cervical Cerclage Procedure Preparation
Required Supplies:
- Betadine solution.
- Sterile gauze.
- Nylon suture tape.
- Sterile gloves (various sizes).
- Sterile draping pack and surgical gown.
- Sterile instrument tray.
Surgical Instruments (16 Tools):
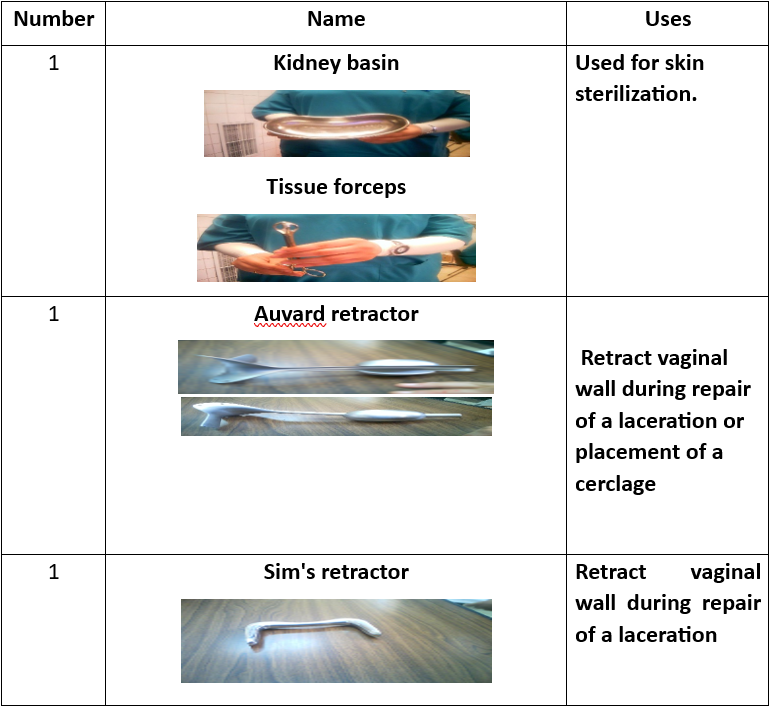
- Instrument tray.
- Tissue forceps.
- Auvard speculum.
- Sims speculum.
- Cervical tenaculum.
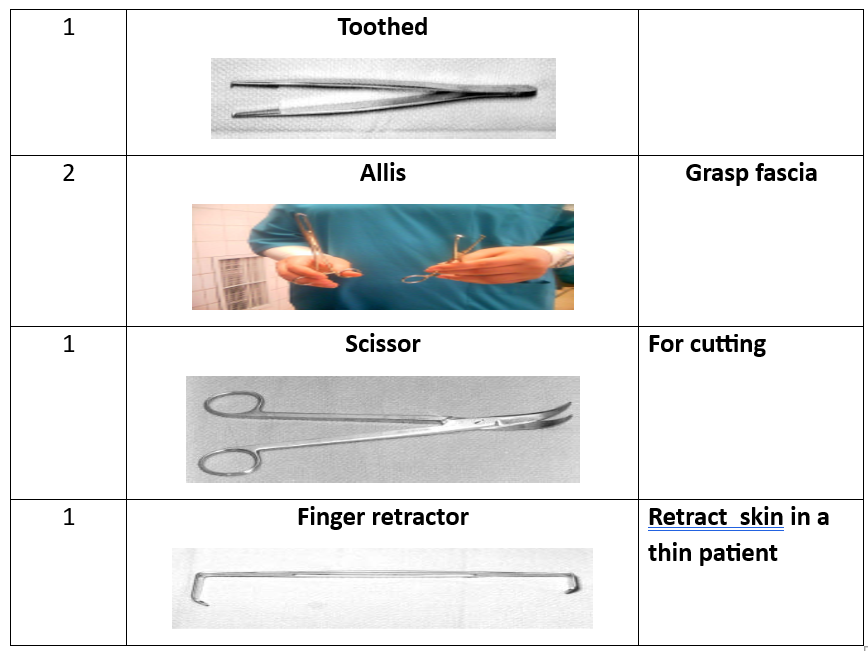
- Scissors.
- Needle holder.
- Scalpel blade.
- Toothed forceps.
- Dressing forceps.
- Ovum forceps.
- Metal catheter.
- Straight clamp.
- Allis clamp.

Shirodkar Technique for Cervical Cerclage
- Bladder emptying using a metal catheter.
- Insertion of an Auvard vaginal speculum.
- Identification of the cervix and securing it with a double-toothed ovum forceps from the front and back.
- Use of an angled vaginal speculum to improve visibility.
- Making a horizontal incision in the anterior cervical mucosa at the bladder reflection.
- Lubricating the suture and placing it at the level of the internal cervical os, tying it at the back to prevent erosion into the bladder, and closing it at the front.
McDonald Technique for Cervical Cerclage
- Similar steps to the Shirodkar technique.
- Cervical suturing is placed at the back, close to the uterine pelvic ligament, without passing into the pelvic cavity.
- Four to five purse-string sutures are placed, ensuring adequate connective tissue inclusion without entering the cervical canal.
- Sutures are left long to facilitate easy removal.
Transabdominal Cervical Cerclage Procedure
- Abdominal incision after the 12th week of pregnancy using a vertical incision in the abdominal and peritoneal layers.
- Bladder peritoneum incision using sharp scissors.
- Pushing the intestines upward and stabilizing the uterine fundus.
- Passing the needle with cervical-uterine sutures from front to back on both sides and tying it at the posterior peritoneal surface using a square knot.
- Inspecting for injuries or bleeding.
- Closing the abdominal incision.
Complications of Cervical Cerclage
- Cerclage failure.
- Infection, including chorioamnionitis.
- Cervical rupture.
- Premature rupture of membranes.
- Preterm labor.
Nursing Care
Preoperative Preparation
1. Assessment:
- Obtain complete medical history (patients with an incompetent cervix usually do not exhibit contractions or other labor symptoms).
- Physical examination.
- Urine test to detect cervical insufficiency and associated congenital anomalies (short cervix, double uterus, or uterine malformations).
- Diagnostic tests:
- Fetal well-being assessment.
- Blood, urine, and biochemical tests.
- Cervical smear to check for STIs or abnormalities.
- ECG and chest X-ray to evaluate heart and lung function.
2. Patient Preparation:
- Explain procedure risks, benefits, and expected outcomes.
- Advise avoiding sexual intercourse for at least 7 days before surgery.
- If cerclage is placed before week 12, it is done vaginally; after week 12, it is performed abdominally.
- Encourage rest and avoidance of strenuous activities.
- Fasting for at least 6 hours before surgery.
- Remove jewelry and metallic objects.
- Bowel preparation via enema.
- Bladder preparation (catheterization).
- Ultrasound scan to exclude fetal abnormalities.
- Monitor fetal heart rate and maternal vital signs.
- Observe for vaginal bleeding.
- Position the patient in the lithotomy position.
- Cleanse the surgical site with 10% Betadine.
- Drape the patient appropriately.
- Administer prophylactic antibiotics as prescribed.
Postoperative Nursing Care
- Monitor consciousness level.
- Observe vital signs and positioning.
- Administer analgesics and oxygen as needed.
- Monitor fluid intake and output.
- Assess vaginal bleeding.
- Evaluate fetal heart rate and tone.
Patient Education
- Advise immediate hospital visit if any of the following symptoms occur:
- Amniotic fluid leakage.
- Reduced fetal movement.
- Fever.
- Abnormal vaginal discharge (foul-smelling).
- Plan for cerclage removal at week 37 before labor.
- Nutritional guidance:
- Increase vegetable intake.
- Consume high-protein foods.
- Drink 1–2 liters of milk daily.
- Ensure adequate fluid intake.
