
Book
Guidelines for Obstetrics and Gynecology Nursing Procedures
- Hysterectomy (Uterus Removal Surgery)
Introduction
Hysterectomy is a surgical procedure to remove the uterus, making pregnancy impossible. It is a major operation with significant risks and benefits, affecting hormonal balance and long-term health. Therefore, it is considered a last resort for treating severe gynecological conditions.
- In 2012–2013, around 30,500 hysterectomies were performed in England.
- The procedure is most common in women in their 50s.
Definition
Hysterectomy is a surgical removal of the uterus through an abdominal or vaginal incision.
Epidemiology
- Second most common surgery among women in the U.S.
- 1 in 3 women in the U.S. undergoes a hysterectomy by age 60.
- Over 600,000 hysterectomies are performed annually.
- More than 90% are for benign (non-cancerous) conditions.
- Over 70% also involve ovary removal (oophorectomy).
Indications for Hysterectomy
Obstetric Indications:
- Uterine rupture.
- Uncontrollable postpartum hemorrhage.
- Placental abnormalities.
Gynecological Indications:
- Infections (e.g., some cases of genital tuberculosis).
- Tumors:
- Benign: Ovarian tumors, leiomyomas (fibroids).
- Malignant: Cervical, endometrial, or ovarian cancer.
- Pelvic organ prolapse: Some cases of chronic uterine prolapse.
- Severe dysfunctional uterine bleeding (DUB).
Types of Hysterectomy
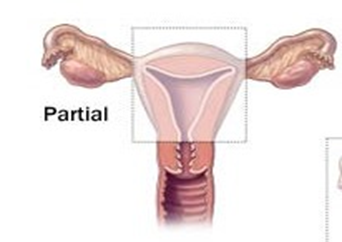
- Subtotal Hysterectomy (Partial Hysterectomy):
- Removes the uterine body while preserving the cervix.
- Commonly performed for postpartum hemorrhage and uterine rupture.
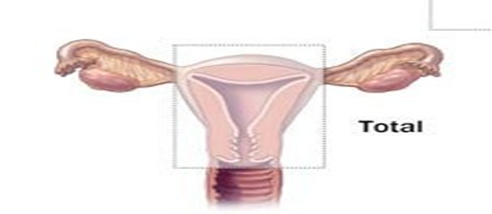
- Total Hysterectomy:
- Removes both the uterine body and cervix.
- Considered more effective than a subtotal hysterectomy.
- Pan-Hysterectomy (Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy - TAHBSO):
- Complete removal of the uterus, ovaries, and fallopian tubes.
- Performed for malignant conditions or severe gynecological disorders.
- Radical Hysterectomy:
- Specifically used for invasive gynecologic cancers.
- Involves the removal of the uterus, fallopian tubes, ovaries, upper two-thirds of the vagina, and pelvic & para-aortic lymph nodes.

Ultra-Radical Hysterectomy:
- Anterior Exenteration: Involves removal of the bladder along with the uterus.
- Posterior Exenteration: Involves removal of the bladder and intestines along with the uterus.
Differences Between Total and Subtotal Hysterectomy
Subtotal Hysterectomy (Partial):
- Removes the uterus but retains the cervix.
- Higher risk of cervical cancer.
- Increased risk of cervical and vaginal infections.
- Easier and shorter surgical procedure.
- Lower risk of bladder and ureteral injuries.
- Lower risk of pelvic organ prolapse.
- Lower risk of pelvic inflammatory disease.
- Reduced likelihood of pain during intercourse.
Total Hysterectomy:
- Removes both the uterus and cervix.
- No risk of cervical cancer.
- No risk of cervical or vaginal infections.
- More complex and longer procedure.
- Higher risk of bladder and ureteral injuries.
- Increased risk of pelvic organ prolapse.
- Higher risk of pelvic inflammatory disease.
- Greater likelihood of pain during intercourse.
Types of Hysterectomy Procedures:
- Abdominal Hysterectomy (AH).
- Vaginal Hysterectomy (VH).
- Laparoscopic Hysterectomy (LH).
Abdominal Hysterectomy:
- Involves an incision in the abdominal wall.
- Provides better visibility of the abdominal cavity.
- Higher risk of complications.
- Leaves a large scar after healing.
Factors Affecting the Choice of Abdominal Hysterectomy:
- Ovarian disease.
- Limited uterine mobility.
- Cancer.
- Large fibroids (leiomyomas).
- Lack of surgical expertise or confidence.
- Pelvic adhesions.
- Radical hysterectomy cases.
- Hysterectomy during pregnancy.
- Emergency cases.
- Chronic pelvic inflammatory disease.
- Multiple fibroids.
Abdominal Hysterectomy Technique:
- Patient is positioned on her back.
- General anesthesia is administered.
- Thorough abdominal and pelvic examination under anesthesia.
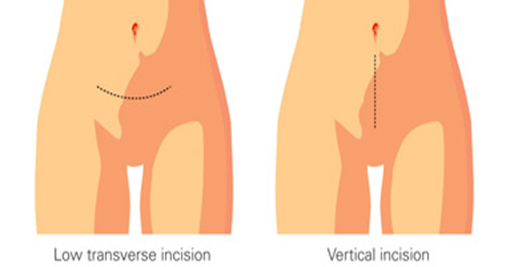
- Surgical Incision:
- Vertical Incision: Used in cases of morbid obesity, suspected endometriosis, or previous abdominal surgeries.
- Transverse Incision: Preferred for benign localized diseases.
- Examine the upper abdominal organs, especially the liver, spleen, and abdominal lymph nodes.
- Place surgical towels to elevate and secure abdominal organs.
- Clamp and ligate the round ligaments.
- Incise the peritoneum between the round ligaments and the bladder.
- Separate ovarian layers, identify the ureter, and ligate ovarian vessels if necessary.
- Incise the ovarian tissue toward the uterus, exposing the uterine vessels.
- Clamp and ligate the uterine vessels at the internal cervical level.
- Clamp and ligate the pelvic ligaments.
- Incise the peritoneum between the pelvic ligaments and the uterus.
- Detach the rectum from the posterior uterus.
- Remove the uterus completely through a vaginal incision below the cervix.
- Close the vaginal vault using absorbable sutures and secure pelvic and rectal ligaments to prevent pelvic organ prolapse.
These steps outline the surgical procedure for an abdominal hysterectomy, which must be performed by a specialized gynecologic surgeon.
Abdominal Hysterectomy Technique
|
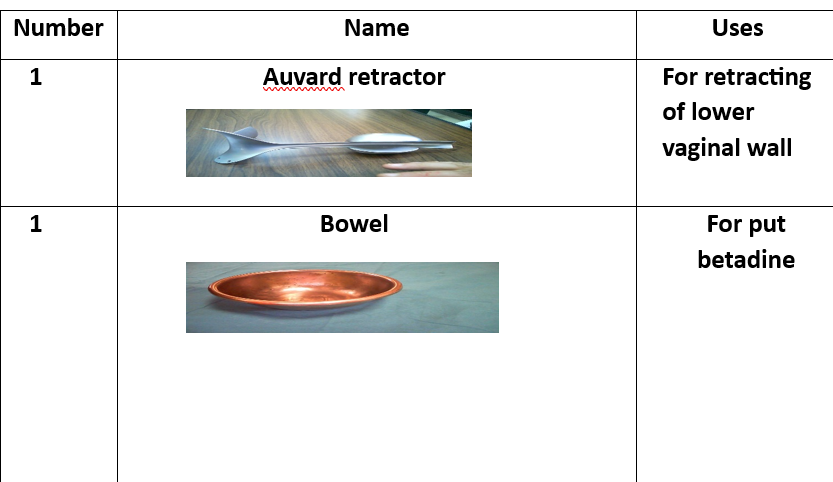
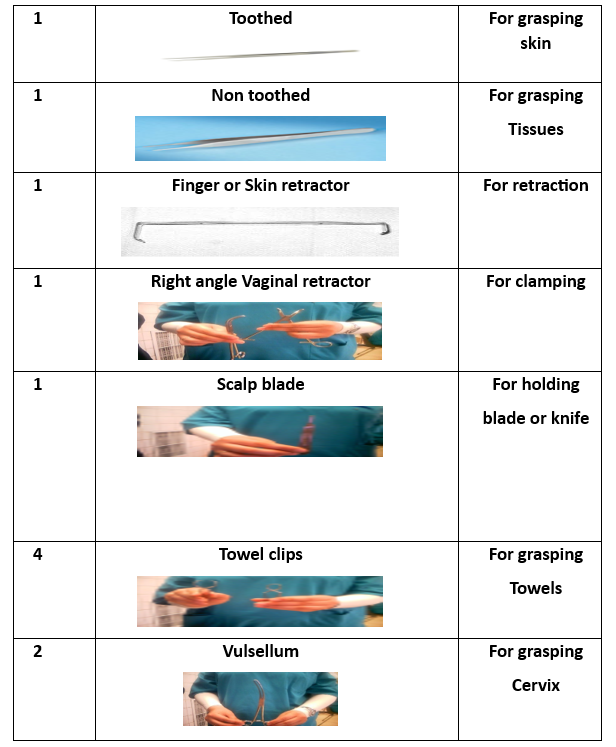
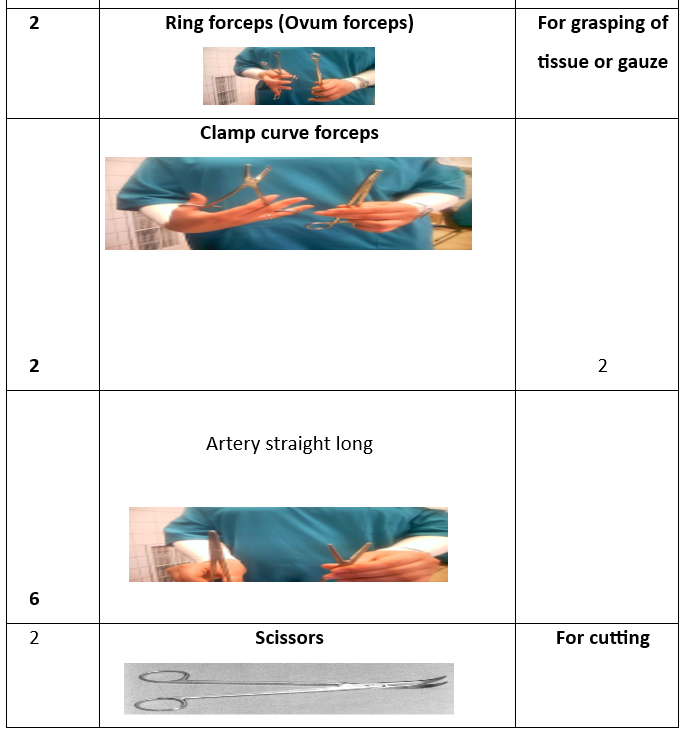
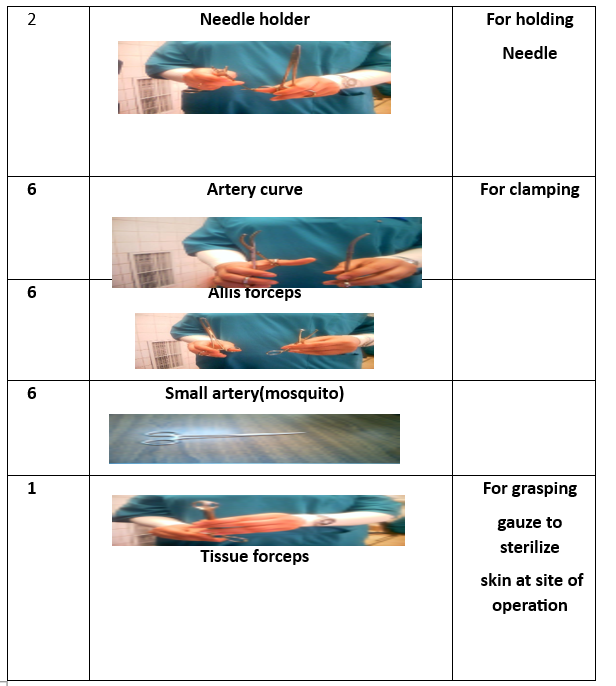
حوض لجمع الأدوات. ملقط الأنسجة. حامل الرحم. ملقط أسنان. ملقط غير أسنان. شفرة скаلب. مقص. مشبك. مشبك فولسيلوم. مقبض الإبرة. مشبك بويضة. ممد ديفير. مشبك كوكر. مشبك آليس. مشبك منحني. مشبك مستقيم. |
1 Kidney basin 1 Tissue forceps 1 Uterine holder 1Toothed 1 Non toothed 1 Scalp blade 1 Scissor 1 Dissector 1 Vulsellum 2 Needle holders 2Rings(Ovum-forceps) 2 Deaverd retractors 2 Right angle clamps 4 Towel clips 4 Kocher forceps 4 Allis 6 Clamps curved 6 Arteries straight 6 Arteries curved
|
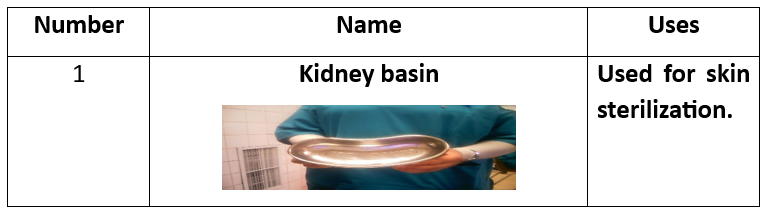
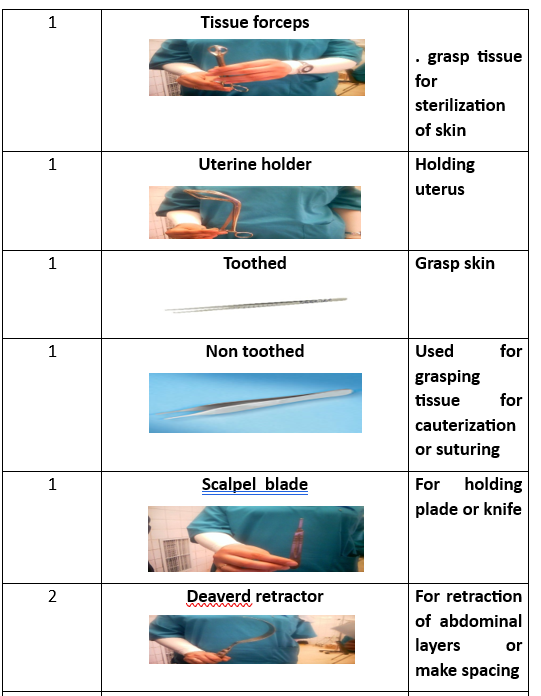
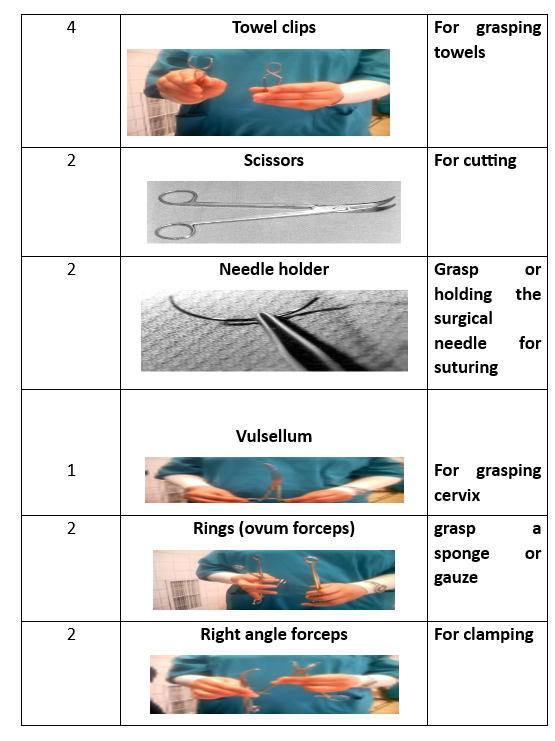
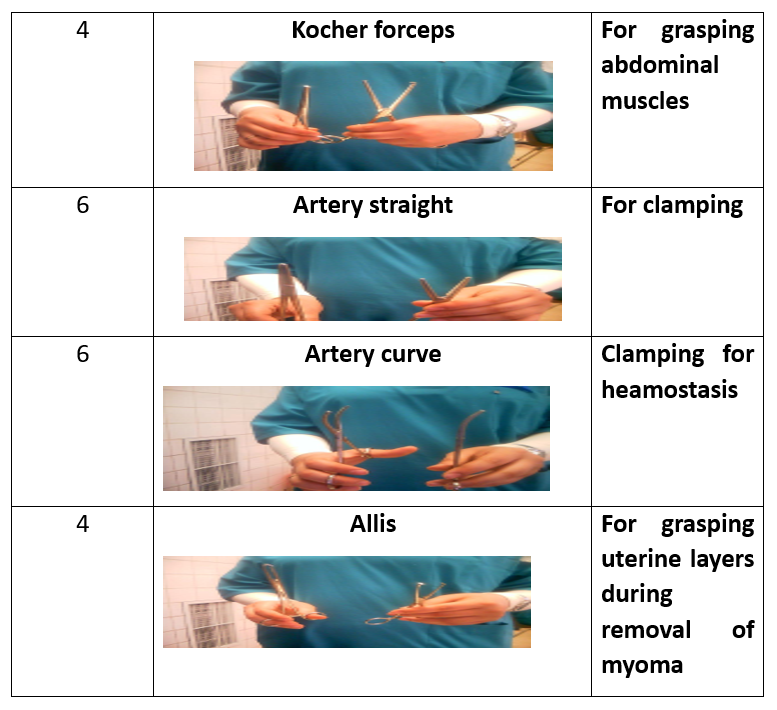
Preparatory Equipment for Abdominal Hysterectomy
(List of preparatory equipment to be provided as needed.)
Steps of Abdominal Hysterectomy Procedure
- Prepare the patient.
- Administer general anesthesia.
- Perform abdominal and pelvic examination.
- Make a surgical incision (vertical or transverse).
- Open the fascia and create an abdominal plane.
- Make a vertical incision in the uterus and approximate its edges.
- Clamp and ligate the round and ovarian ligaments.
- Repeat the steps on the opposite side.
- Remove the uterus.
- Incise the cervix.
- Remove the cervix.
- Close the vaginal vault.
- Irrigate the surgical site.
- Close the pelvic and abdominal layers.
Vaginal Hysterectomy Procedure
Definition:
A surgical procedure in which the uterus is removed through the vaginal canal via an incision at the upper part of the vagina.
Indications:
- Certain cases of uterine prolapse.
- Some cases of dysfunctional uterine bleeding.
- Selected cases of endometrial cancer.
Advantages and Disadvantages of Different Hysterectomy Techniques
Abdominal Hysterectomy
✅ Advantages:
- No limitation on uterine size.
- Can be combined with reconstructive or additional surgeries.
- No increase in postoperative complications.
❌ Disadvantages:
- Longer recovery period.
- Higher risk of bleeding compared to other techniques.
- Vaginal or laparoscopic hysterectomy is preferred for obese patients.
Vaginal Hysterectomy
✅ Advantages:
- Shorter surgery time.
- Faster recovery.
- Less pain and lower cost.
❌ Disadvantages:
- Limited to smaller uterine sizes.
- Limited visualization of the ovaries and uterus.
- Cannot always be combined with other surgical procedures.
Subtotal Laparoscopic Hysterectomy
✅ Advantages:
- Faster recovery and return to normal activities.
- No proven impact on sexual function.
❌ Disadvantages:
- Requires regular cervical cancer screening.
- Possible periodic bleeding.
- No confirmed reduction in pelvic organ prolapse risk.
Laparoscopic-Assisted Vaginal Hysterectomy (LAVH)
✅ Advantages:
- Can be used for larger uteri.
- Can be combined with other surgeries.
❌ Disadvantages:
- Higher cost than vaginal hysterectomy.
- Not recommended for patients with heart or lung disease.
Total Laparoscopic Hysterectomy (TLH)
✅ Advantages:
- Shortest recovery time.
- Allows diagnosis and treatment of other pelvic conditions.
- Fast return to daily activities.
❌ Disadvantages:
- Longer surgical duration.
- Increased risk of ureter or bladder injury.
- Requires high surgical skill.
Single-Incision Laparoscopic Hysterectomy
✅ Advantages:
- Better cosmetic results.
❌ Disadvantages:
- No clinically significant improvements over traditional methods.
- Requires further research.
Robot-Assisted Hysterectomy
✅ Advantages:
- Similar complication rates to conventional laparoscopy.
- May lead to shorter recovery periods.
❌ Disadvantages:
- Longer surgery time.
- Higher costs.
- Requires further research.
Hysterectomy Complications
- Shock.
- Hemorrhage.
- Infection.
- Bowel complications (e.g., acute gastric dilation).
- Respiratory complications (e.g., pneumonia, atelectasis).
- Venous thromboembolism (DVT, SVT).
- Anesthesia-related complications.
- Late complications: Vaginal discharge, pelvic organ prolapse, back pain.
- Menopausal symptoms: Mood changes, irritability (especially in younger women).
Nursing Management for Hysterectomy Patients
Preoperative Care
- Assess the patient’s understanding of the procedure.
- Explain the procedure and provide emotional support.
- Clean the abdominal and pelvic area.
- Administer preoperative medications.
- Ensure informed consent is signed.
Postoperative Care
- Monitor for bleeding.
- Check vital signs.
- Assess vaginal discharge.
- Monitor surgical wounds and bowel sounds.
- Encourage early ambulation.
- Encourage fluid intake.
- Educate the patient on perineal hygiene.
- Restrict physical activity for 4-6 weeks.
- Explain symptoms that require medical attention.
- Provide information on hormone replacement therapy (if needed).
- Encourage routine gynecological check-ups.
