
Book
Guidelines for Obstetrics and Gynecology Nursing Procedures
- Pelvic Organ Prolapse
Introduction
Pelvic organ prolapse occurs when one or more pelvic organs slip from their normal position, leading to bulging into the vaginal canal. Affected organs include the uterus, vagina, bowel, and bladder, due to weakened muscles and supportive ligaments.
Definition
Pelvic Organ Prolapse (POP) is the downward displacement or protrusion of pelvic organs beyond their normal anatomical boundaries.
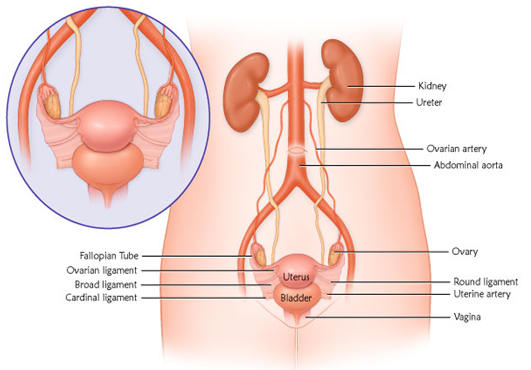
Factors Maintaining Organ Position
- Normal uterine position.
- Deep pelvic muscles.
- Supportive ligaments of the uterus, vagina, and ovaries.
Causes of Pelvic Organ Prolapse
1. Predisposing Factors:
- Congenital weakness.
- Birth-related injuries.
- Pelvic infections.
2. Triggering Factors:
- Increased pelvic pressure.
- Pelvic tumors.
- Obesity.
High-Risk Groups
1. Age:
- Younger than 18 years.
- Postmenopausal women.
- Pregnant women.
2. Medical Conditions:
- Chronic lung diseases.
- Jaundice.
- Chronic constipation.
3. Obstetric History:
- Multiple childbirths.
- Twin or multiple pregnancies.
Classification of Pelvic Organ Prolapse
- Vaginal Prolapse:
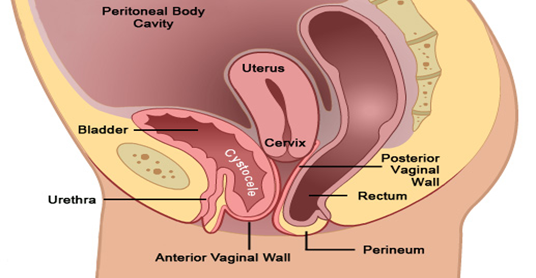
- Anterior Vaginal Wall Prolapse (Cystocele): Downward displacement of the bladder into the vaginal canal.
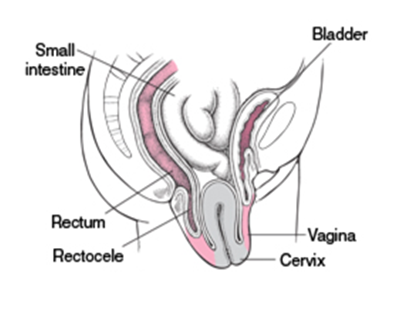
Posterior
Vaginal Wall Prolapse (Rectocele): Downward displacement of the rectum into the
vaginal canal
- Uterine Prolapse: Descent of the uterus from its normal position into the vaginal canal.

- Ovarian Prolapse: Descent of the ovaries from their normal position into the pelvic or vaginal area.
- Total Vaginal Prolapse: Complete prolapse of the vaginal walls, often occurring after a hysterectomy, where the top of the vagina collapses downward.
Symptoms
- Prolapse of pelvic organs.
- Pelvic pain.
- Difficulty urinating.
- Pain during intercourse.
Treatment
- Pelvic floor exercises.
- Support devices (Pessary).
- Surgery.
- Lifestyle changes.
Types of Pelvic Organ Prolapse
Anterior Vaginal Wall Prolapse
- Cystocele: Prolapse of the upper third of the anterior vaginal wall with the bladder.
- Cystourethrocele: Complete prolapse of the anterior vaginal wall with the bladder and urethra.
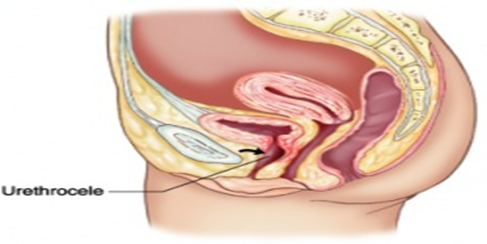
- Urethrocele: Prolapse of the lower third of the anterior vaginal wall with the urethra.
Posterior Vaginal Wall Prolapse
- Rectocele: Prolapse of the anterior wall of the rectum with the middle third of the posterior vaginal wall.
- Enterocele: Prolapse of the upper third of the posterior vaginal wall with the peritoneum and bowel.
Combined Prolapse
- Cystorectocele: Prolapse of both the anterior and posterior vaginal walls.
Pelvic Prolapse After Hysterectomy
- Vaginal vault prolapse: Prolapse of the vaginal apex after hysterectomy.
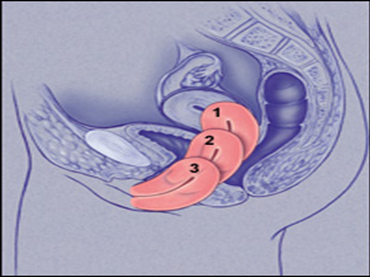
Uterine Prolapse
- First degree: Mild prolapse of the uterine cervix.
- Second degree: Prolapse with the cervix protruding from the vagina.
- Third degree: Complete uterine prolapse (Procidentia).
Combined Uterine and Vaginal Prolapse
- Uterine prolapse followed by vaginal prolapse.
- Vaginal prolapse followed by uterine prolapse.
Ovarian Prolapse
Clinical Symptoms
- A feeling of heaviness or pressure in the pelvis.
- Chronic pelvic, abdominal, and back pain.
- Pain during intercourse.
- Unusual vaginal discharge.
- Constipation.
- Frequent or urgent urination.
- A feeling of prolapse or bulging.
Medical Management
The optimal management of pelvic organ
prolapse depends on the following factors:
- Severity of clinical symptoms.
- Severity of prolapse.
- Patient’s age and health status.
- The patient's desire for fertility.
Conservative Management
- Pelvic floor exercises (Kegel exercises): Improve pelvic muscles and reduce prolapse.
- Support devices (Pessary):
• Made from plastic, rubber, or silicone.
• Used for temporary support of prolapsed tissues.
• Can be left in place for up to one year.
• The most common shape is a ring, available in various sizes and shapes.
Conservative Management Devices
- Colpexin Sphere: A vaginal device that supports pelvic muscles and improves exercises.
- Pessary devices:
• Indications: Pregnancy, trial of therapy, awaiting surgery.
• Contraindications: Acute pelvic infection, patient discomfort.
• Complications: Vaginal ulcers, pessary incarceration. - Vaginal estrogen creams:
• For mild prolapse, used for 4-6 weeks.
Surgical Management
- Anterior colporrhaphy.
- Burch colposuspension.
- Sling surgery.
- Vaginal hysterectomy.
- Sacrohysteropexy.
Midline Operations
- Uterine prolapse surgeries:
• Vaginal hysterectomy.
• Sacral fixation of the uterus. - Vaginal prolapse surgeries:
• Sacral fixation of the vagina.
Risks and Instructions
- Consult with a doctor.
- Regular follow-ups.
- Weight reduction.
- Perform pelvic exercises.
Posterior Operations
- Sacrocolpopexy (Vaginal vault fixation): Performed through open, robotic, or laparoscopic techniques.
- Sacrospinous fixation: Performed via vaginal and abdominal routes.
Treatments for Vault and Bowel Prolapse
- Sacral fixation of the vault.
- Sacrospinous ligament fixation of the vault.
- Iliococcygeus muscle fixation of the vault.
- McCall culdoplasty (muscle contraction fixation).
- Uterosacral ligament suspension.
Treatments for Vaginal Prolapse
- Iliococcygeus muscle fixation of the vagina.
- Pelvic muscle reconstruction (Perineorrhaphy).
- Obliterative vaginal operations.
Posterior Operations
- Repair of posterior wall prolapse.
- Repair of fascial defects.
- Placement of mesh in the posterior vaginal wall.
Traditional Treatments
- Repair of the anterior and posterior vaginal walls.
- Sacral fixation of the vaginal vault.
- Sacrospinous fixation of the vagina.
Classical Surgical Treatment Technique
Equipment and Supplies
- Betadine (disinfectant).
- Sterile towels.
- Sterile surgical gloves (various sizes and large quantities).
- Sterile bag for sterilization and draping.
- Sterile bag for surgical instruments.
- Surgical sutures and needles.
- Sterile towels for teaching.
Classic Repair Procedure
Surgical Instruments
- Instruments for vaginal hysterectomy (50 instruments).
- Additional instruments:
• 4 Breisky instruments for incision opening.
• Metallic catheter.
• Double-toothed forceps.
• Single-toothed forceps.
• Dissector scissors.
Steps for Procedure
A) Anterior Vaginal Wall Repair (Vaginal Approach):
- Empty the bladder using a metal catheter.
- Make a longitudinal incision in the anterior vaginal membrane.
- Separate the vaginal membrane from the pelvic muscles.
- Expose the bladder and urethra.
- Support the tissue around the bladder.
- Remove excess skin.
- Check for bleeding and remove instruments.
B) Posterior Vaginal Wall Repair (Vaginal Approach):
- Empty the bladder.
- Place Breisky instruments.
- Place forceps in the labia.
- Make a triangular incision in the skin.
- Separate the pelvic muscles from the posterior vaginal membrane.
- Extend the incision to the rectal margin.
- Suture the pelvic muscles.
- Close the incision.
- Strengthen pelvic muscles.
- Check for bleeding and remove instruments.
Surgical Complications in Pelvic Organ Prolapse Management
- Bladder prolapse under pressure (SUI).
- Pain during intercourse (Dyspareunia) or inability to have intercourse (Apareunia).
- Surgical failure due to:
• Poor surgical technique.
• Failure to recognize or treat bowel prolapse.
• Inadequate anterior vaginal wall repair.
• Pregnancy after surgery.
• Weak support due to infection or development.
Complications of Pelvic Organ Prolapse
- Keratin formation in the vagina.
- Pressure ulcers.
- Enlargement and elongation of the cervical neck.
- Inflammation and swelling of the cervical neck.
- Obstruction of urinary pathways (bladder pressure on the ureter, ureteral and kidney infection).
- Pessary incarceration.
- Cancer of the cervical or vaginal area.
Nursing Management for Pelvic Organ
Prolapse
Building a Positive Nurse-Patient Relationship
- Establish trust with the patient and family.
- Take patient history, perform physical examination, and review tests.
- Guide the patient to prevent pelvic organ prolapse.
Prevention Across Life Stages
- Childhood: Proper nutrition, avoiding constipation, healthcare.
- Adolescence: Maintain healthy pregnancy, avoid early pregnancy.
- Pregnancy: Prenatal care, avoid sexually transmitted diseases.
- Birth: Bladder and rectum care, breathing exercises.
- Postpartum: Perineal washing, proper nutrition, Kegel exercises.
- Menopause: Regular checkups, cervical screening, hormone therapy.
Patient Instructions on Pessary Use
- Avoid inserting anything into the vagina.
- Regular checkups to prevent inflammation and infection.
- Care for the pessary: Remove it for cleaning, consult with a doctor.
Patient Instructions on Hormonal Therapy
- Benefits and drawbacks of hormonal therapy.
- Importance of cell examination and imaging.
- Take the therapy regularly.
- Avoid abruptly stopping the therapy.
Lifestyle Changes
- Perform pelvic exercises regularly.
- Maintain a healthy weight.
- Eat fiber-rich foods.
- Avoid smoking and alcohol.
- Avoid activities that require heavy lifting.
Nursing Management for Surgical Patients
Before Surgery
- Assess the patient.
- Health education.
- Prepare the patient for surgery.
- Perform necessary tests.
After Surgery
- Monitor the patient.
- Health education.
- Wound care.
- Administer medications.
- Follow-up care.
Preventing Recurrence of Prolapse
- Delay pregnancy.
- Use contraception.
- Avoid increasing internal pressure.
- Perform pelvic exercises regularly.
- Maintain a healthy weight.
- Eat fiber-rich foods.
