Book
Screening of prediabetes and Type 2 Diabetes in Pediatrics
- Recommendations
|
Table 3. Recommendations |
|
|
|||
|
A. Management of Type 2 Diabetes |
|
|
|||
|
N |
Health questions |
Source Guideline |
Recommendations |
Quality of evidence |
Strength of Recommendation |
|
A1 |
Who are the adolescents at risk that should be screened for prediabetes or type 2 diabetes in primary health care setting or general pediatric department or outpatient clinic? |
ISPAD 2024 |
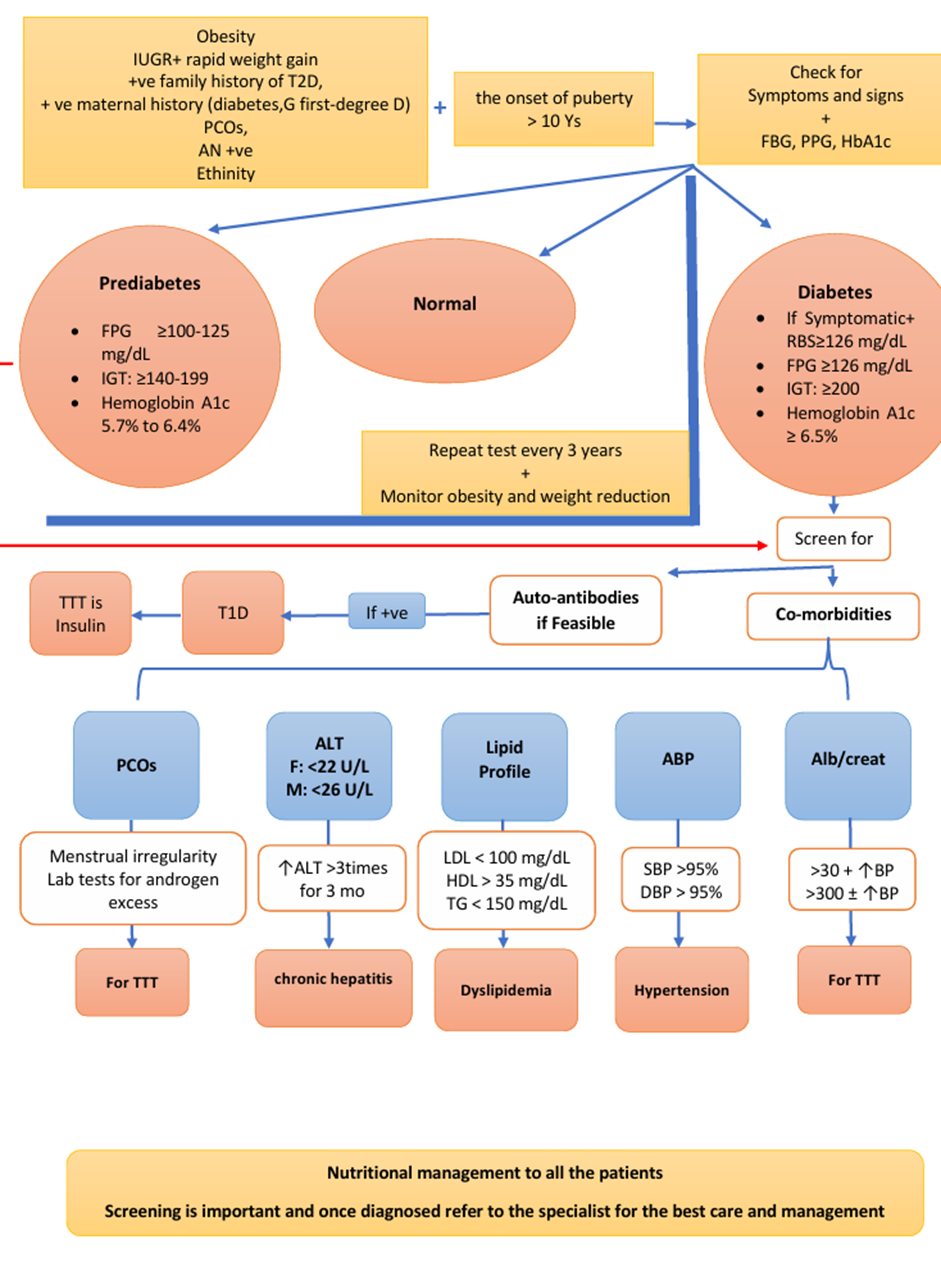
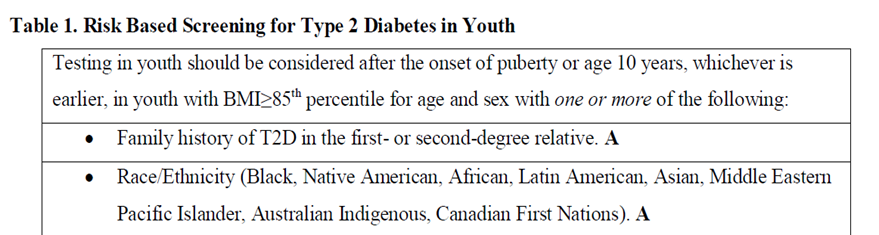
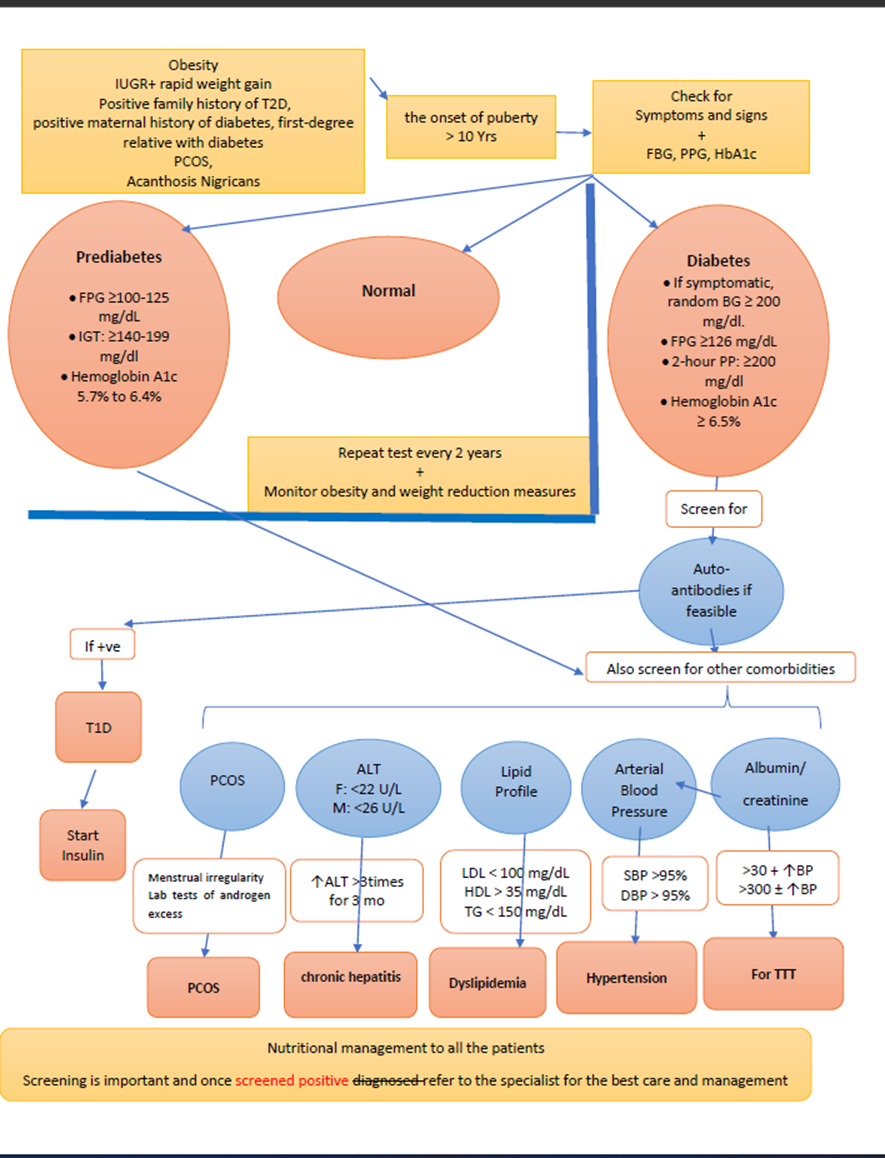
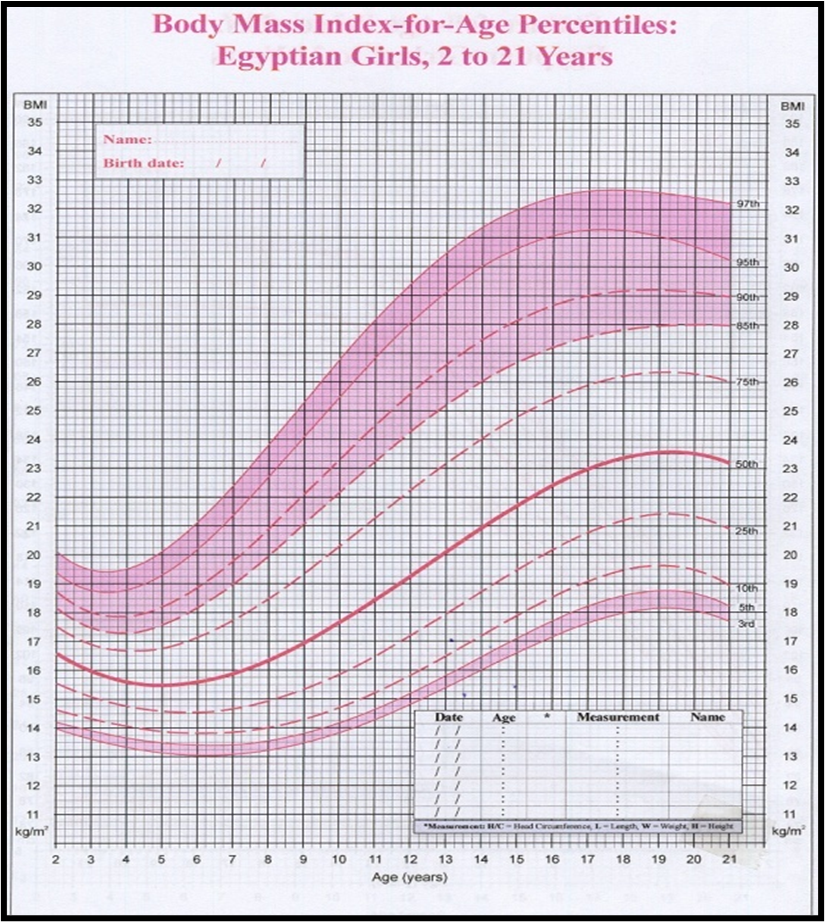
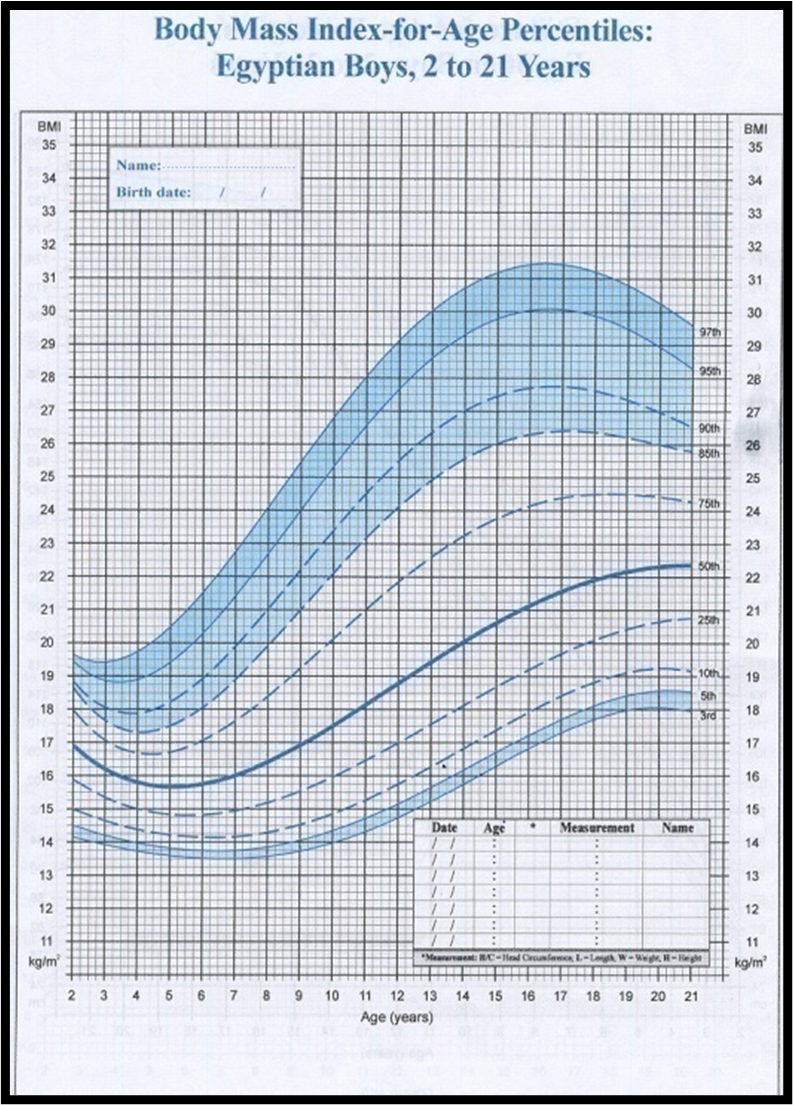
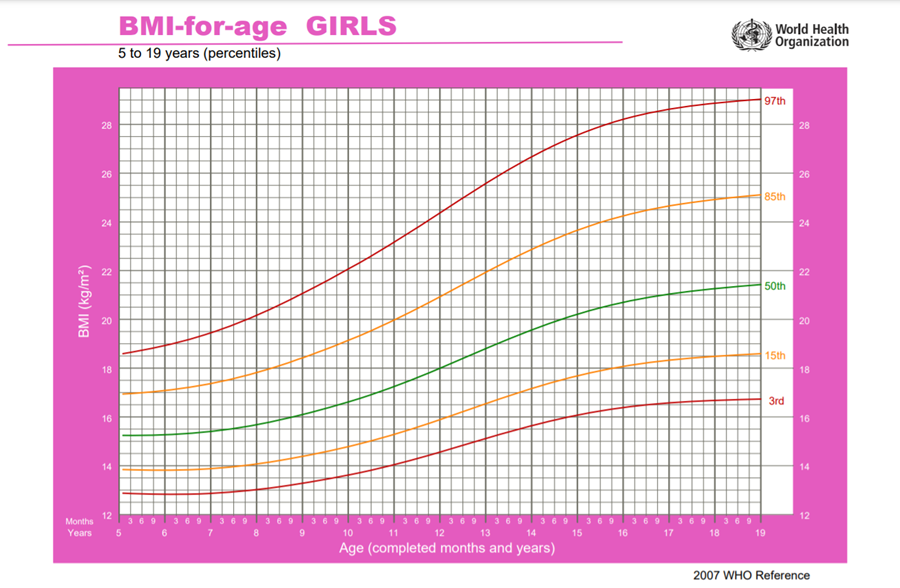
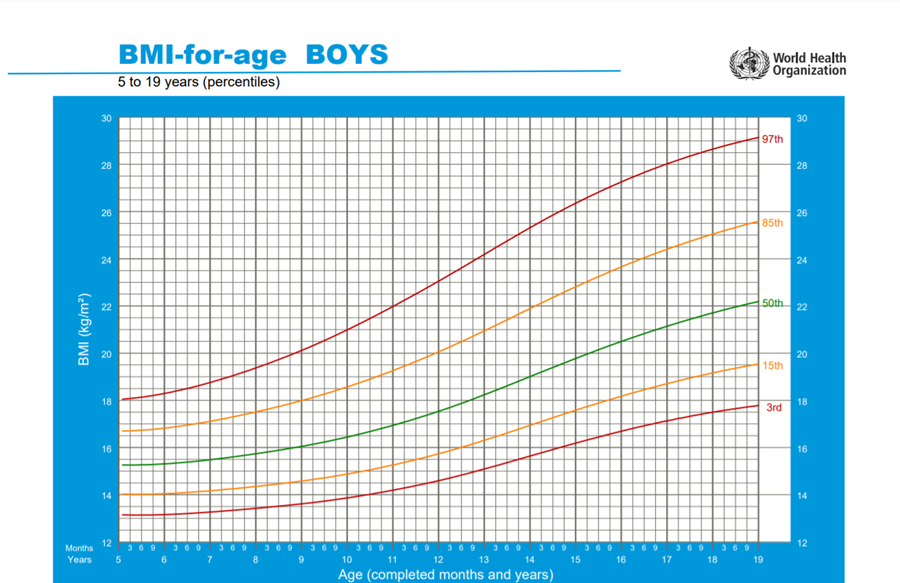
Risk factors to develop type 2 diabetes: Consider testing to identify clinical cases of type 2 diabetes in children and adolescents after the onset of puberty or after 10 years of age, whichever occurs earlier, in those who have risk factors for diabetes, which include: Obesity (BMI > 95th percentile for age and sex), intrauterine growth retardation with rapid infant weight gain, first-degree family history of type 2 diabetes, maternal history of diabetes or gestational diabetes during child's gestation, high-risk ethnicity, polycystic ovary syndrome (PCOS). |
High |
Strong |
|
|
|
ISPAD 2024 |
Risk-based screening for prediabetes and/or type 2 diabetes should be considered after the onset of puberty or after 10 years of age, whichever occurs earlier in children and adolescents who are overweight (BMI > 85th percentile) or obese (BMI > 95th percentile) and who have one or more additional risk factors for diabetes (Refer to table (1) in implementation tools for details and level of evidence). |
High |
Strong |
|
|
|
ISPAD 2024 |
Assessment for dysglycemia in obese at-risk youth should occur in the setting of clinical assessment of other obesity-related comorbidities metabolic dysfunction-associated steatotic liver disease (MASLD), dyslipidemia, elevated blood pressure [BP], and polycystic ovary syndrome) that are more prevalent than dysglycaemia (Refer to Q 6) below).
|
High |
Strong |
|
A2 |
What are tests recommended for screening of prediabetes or type 2 diabetes in primary health care setting or general pediatric department or outpatient clinic? |
ISPAD 2022 |
Fasting plasma glucose, 2-h plasma glucose after 75-g OGTT, and A1C can be used to test for prediabetes or diabetes. |
Intermediate
|
Strong |
|
|
|
Diabetes Canada Clinical Practice Guidelines Expert Committee, Panagiotopoulos C, Hadjiyannakis S, Henderson M. Type 2 Diabetes in Children and Adolescents. Can J Diabetes. 2018 Apr;42 Suppl 1:S254. Doi: 10.1016/j.jcjd.2017.10.037.PMID:29650104.
|
Recommend using a combination of A1C and fasting or random blood glucose to screen for type 2 diabetes in children and youth with risk factors. “A 2-hour OGTT may be considered as an initial screening test in children and youth with 3 or more risk factors and should be done in those in whom there is a discrepancy between the A1C and fasting or random blood glucose results”. |
Good Practice Statement |
|
|
A3 |
What is considered a positive screening test result for prediabetes or type 2 diabetes in primary health care setting or general pediatric department? Sub-questions: -What is the cut off value for normal fasting blood glucose in adolescents? -What is the cut off value for normal postprandial glucose in adolescents? -What is the cut off value for normal HbA1c in adolescents? |
ISPAD 2022 |
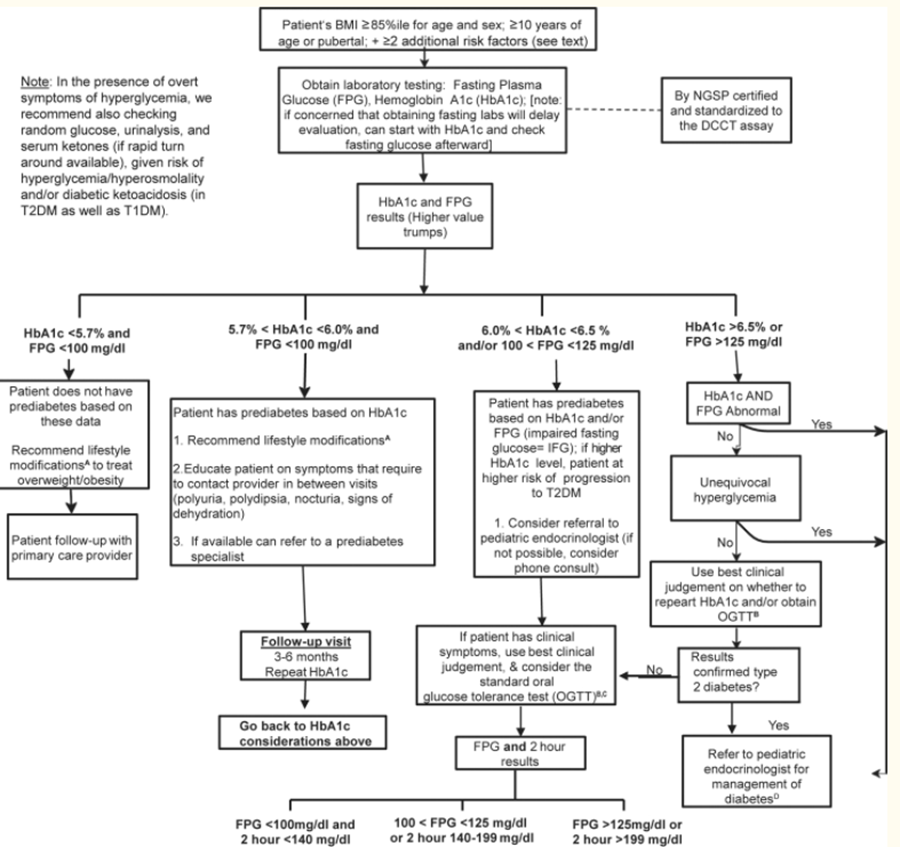
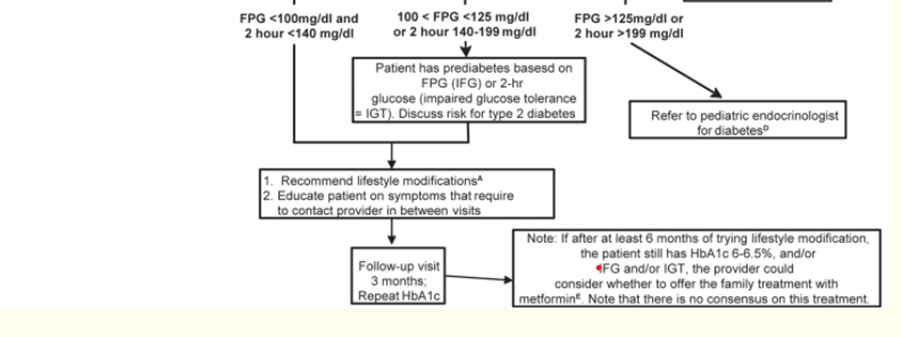
Criteria for considering diagnosis of prediabetes according to ADA definitions: • Impaired fasting glycemia (IFG): FPG ≥100-125 mg/dL • Impaired Glucose tolerance (IGT): Post-challenge plasma glucose is ≥140-199 mg/dL • Hemoglobin A1c ˂5.7% normal, 5.7% to 6.4% prediabetes. (Should be laboratory-based, DCCT aligned, NGSP certified methodology).
|
High |
Strong |
|
|
|
ISPAD 2022 |
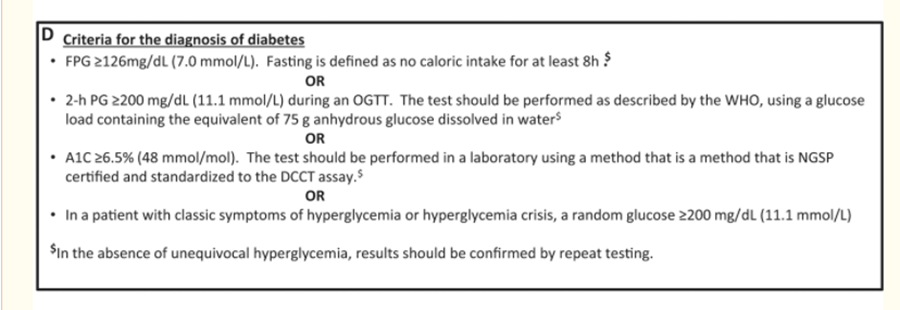
Criteria for diagnosis of type 2 diabetes: a) Symptoms of diabetes (polyuria, polydipsia, nocturia, and unexplained weight loss) and a random plasma glucose ≥200 mg/dL OR · Fasting blood glucose ≥126 mg/dL OR · 2-hour blood glucose concentration during an oral glucose tolerance test (OGTT) ≥200 mg/dL OR · Hemoglobin A1c (HbA1c) ≥6.5% (Should be laboratory-based, DCCT aligned, NGSP certified methodology). Point-of-care measurement of HbA1c is not acceptable for diagnosis.
|
High |
Strong |
|
|
|
ISPAD 2022 |
In the absence of symptoms, testing should be confirmed with a repeat test on a different day.
Measurement of insulin or C-peptide is NOT recommended as part of routine evaluation |
Intermediate
|
Strong |
|
A4 |
When to repeat screening for prediabetes or type 2 diabetes in adolescents if initial tests are normal in those at risk? |
ISPAD 2022 |
If tests are normal:
repeat testing at a minimum of 3-year intervals, or more frequently if BMI is increasing, the cardiometabolic risk profile is deteriorating, there is a strong family history of T2D, or evidence of pre-diabetes |
Low |
Conditional |
|
A5 |
When to consider referral to pediatric endocrinologist and diabetologist in adolescents with suspected prediabetes or type 2 diabetes in the primary health care setting or general pediatric department? |
ISPAD 2022 |
Referral to pediatric diabetologist/endocrinologist is recommended in children and adolescents suspected to have prediabetes or type 2 diabetes according to the American Diabetes Association (ADA) criteria. |
High |
Strong |
|
A6 |
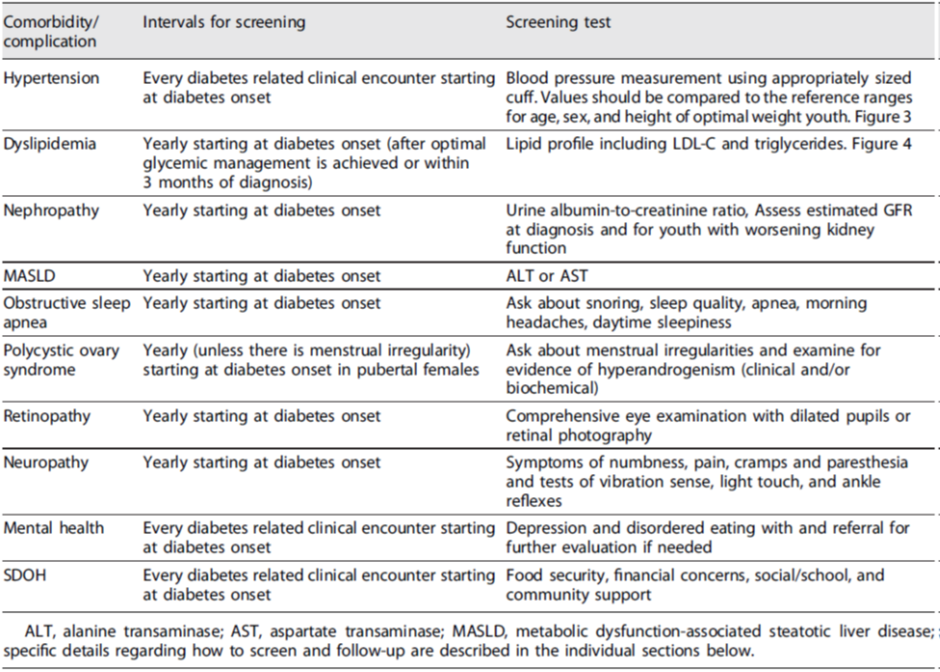
When and how to screen for comorbidities of prediabetes and type 2 diabetes in adolescents at risk in the primary health care setting or general pediatric department or outpatient clinic? Sub-questions: a.When to consider elevated blood pressure? b.What are the normal values for lipids? c.What are the normal values for liver enzymes? d.How to diagnose PCOS? |
ISPAD 2022 |
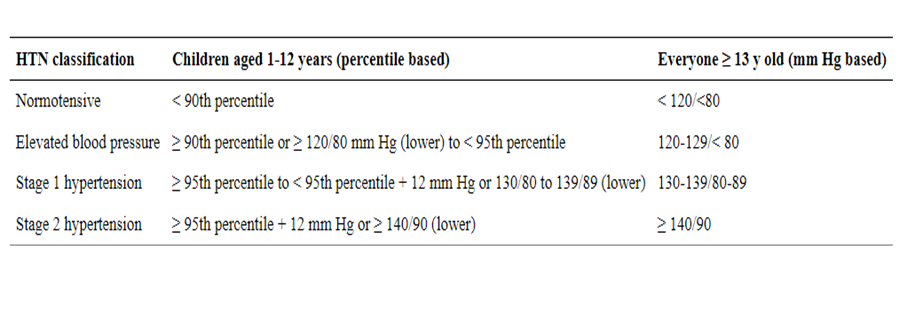
Hypertension: Blood pressure should be monitored at every visit according to standardized techniques specific for children. Elevated BP should be confirmed on 2 additional separate days.
|
High |
Strong |
|
|
|
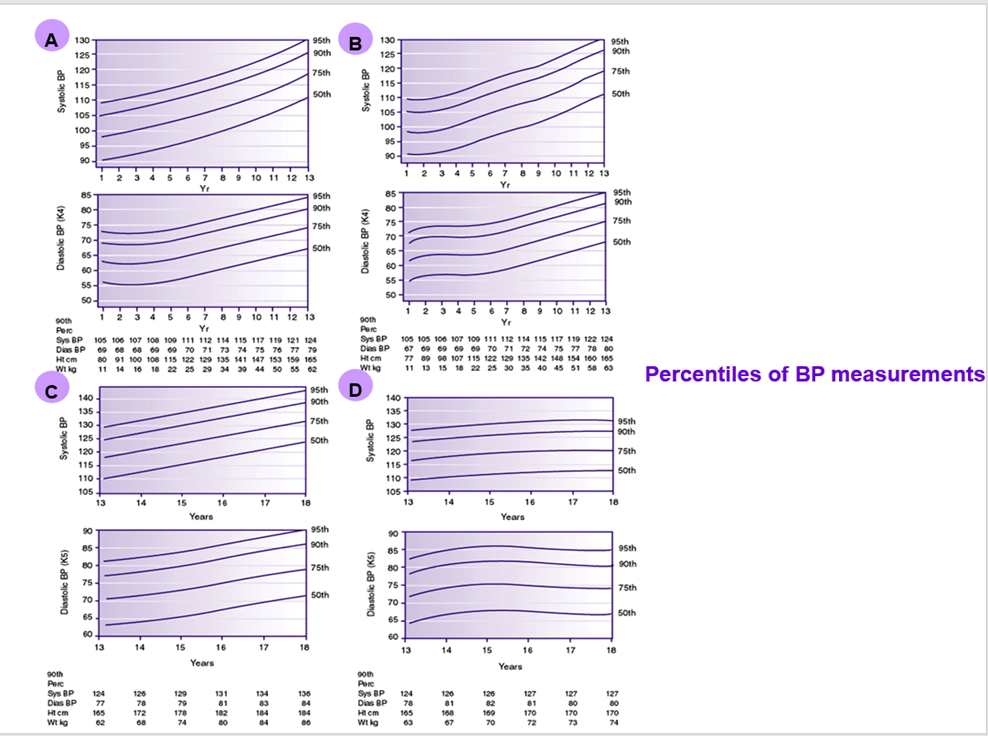
ISPAD 2022 |
Hypertension is defined as an average systolic or diastolic BP > 95th percentile for age, sex, and height, with high normal BP being 90th to <95th percentile. Initial treatment of elevated blood pressure should consist of weight loss, limitation of dietary salt, and increased physical activity. |
Very Low |
Conditional |
|
|
|
ISPAD 2022 |
Dyslipidemia: Initial screening for dyslipidemia does not require fasting Goal levels for lipids are: 1. LDL-Cholesterol < 100 mg/dL 2. HDL- Cholesterol > 35 mg/dL 3. Triglycerides < 150 mg/dL |
Intermediate
|
Strong |
|
|
|
ISPAD 2024 |
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD Evaluation for MAFLD and non-alcoholic Steatohepatitis (NASH) by measuring ALT and AST should be done at diagnosis of type 2 diabetes and annually thereafter |
High |
Strong |
|
|
|
ISPAD 2022 |
Interpretation of ALT should be based upon sex-specific upper limits of normal in children (22 U/L for girls and 26 U/L for boys) and not individual laboratory upper limits of normal.
|
High |
Strong |
|
|
|
ISPAD 2024 |
If liver enzymes remain >3 times the upper limit of normal after 6 months refer to a pediatric gastroenterologist for consultation to exclude other causes of elevated liver enzymes, imaging and/or liver biopsy
|
Intermediate |
Strong |
|
|
|
ISPAD 2022 |
Polycystic ovary syndrome Female patients should be asked about menstrual irregularities, and symptoms of hyperandrogenism. Patients with menstrual irregularities should be tested for hyperandrogenism |
Very low |
Conditional |
|
|
|
ISPAD 2024
|
Diagnosis of PCOS in adolescents should be based on a complete picture that includes clinical signs and symptoms of androgen excess, increased androgen levels, and exclusion of other causes of hyperandrogenemia in the setting of oligomenorrhea (See appendix).
If suspected refer to endocrinologist.
|
Intermediate
|
Strong |
|
A 7 |
1) How to prevent progression of prediabetes to type 2 diabetes in adolescents in primary health care setting or general pediatric department? Sub-questions: a.What are the lifestyle and exercise measures in the primary health care setting or general pediatric department that can help prevent prediabetes development and its progression to type 2 diabetes in adolescent? b.What are the dietary counseling measures in the primary health care setting or general pediatric department that help to prevent prediabetes development and its progression to type 2 diabetes in adolescent? What are the pharmacologic interventions in the primary health care setting or general pediatric department that can help prevent prediabetes development and its progression to type 2 diabetes in children and adolescent? |
ISPAD 2022 |
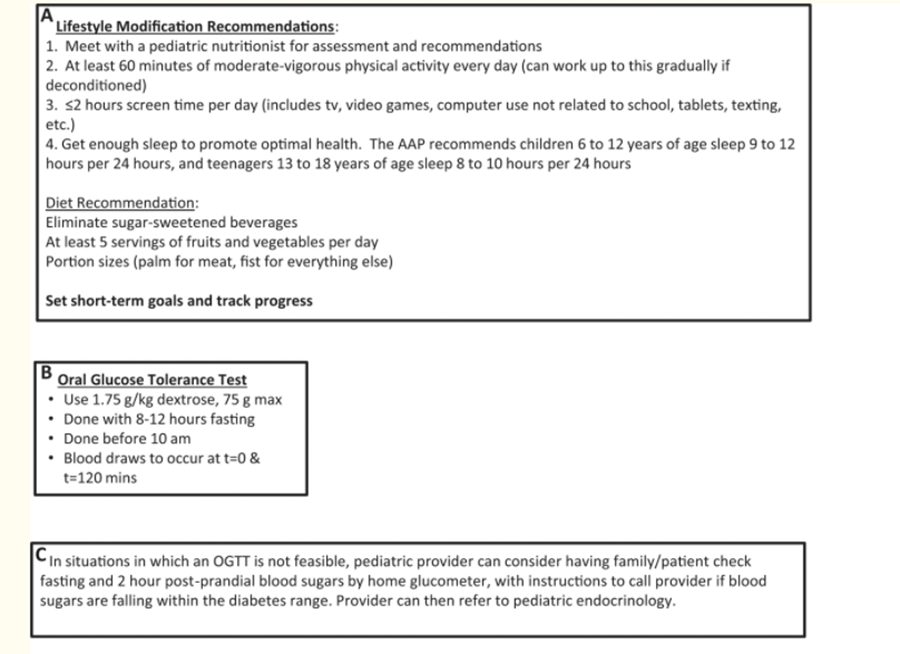
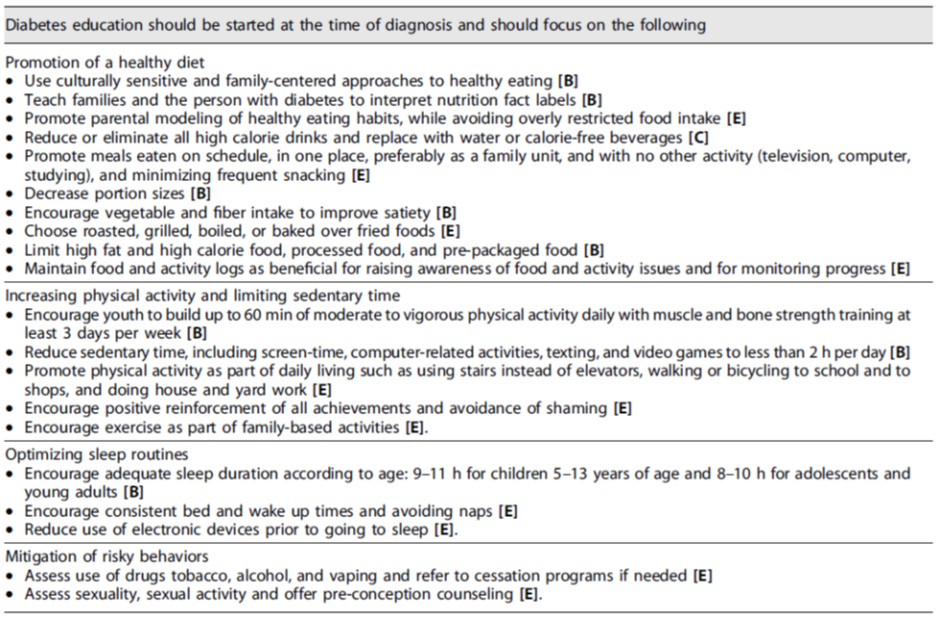
Only lifestyle change, with decreased caloric intake and increased physical activity has been shown to be effective for adolescents with pre-diabetes. |
High |
Strong |
|
|
|
ISPAD 2022 |
Diet modification should focus on: · Eliminating sugar-sweetened soft drinks and juices. · Reducing the intake of foods made from refined, simple sugars and high fructose corn syrup. · Limiting use of high-fat and/or high calorie dense foods.
|
Intermediate
|
Strong |
|
|
|
|
Reducing the use of processed, prepackaged, and convenience foods. • Portion control. • Reducing meals eaten away from home. • Increasing vegetable intake and limited use of fruit as a substitute for high-calorie and low nutrient foods. • Changing staple foods from enriched white rice and white flour to brown rice and whole grain items with lower glycemic index to promote gradual and sustainable absorption with meals. |
Very Low |
Conditional |
|
|
|
Esposito K, et al. A Journey into a Mediterranean diet and type 2 diabetes: a systematic review with meta-analyses. BMJ Open 2015;5:e008222. doi:10.1136/bmjopen-2015-008222 |
The Mediterranean diet which provides a carbohydrate content < 50% of daily energy and includes abundant use of poly- and mono-unsaturated fat (about 20%), mainly olive oil, was found to reverse dysglycemia. |
Good Practise Statement |
|
|
|
|
ISPAD 2022 |
The use of metformin and/or insulin in youth with prediabetes is not currently recommended. |
High |
Strong |

➡️Evidence to recommendations: Considerations
The GDG/ GAG was guided by the results of the AGREE II appraisals of the eligible CPGs and thoroughly reviewed the recommendations of the original source WHO CPGs in consideration of local contextual factors related to the national Egyptian health system like burden of the disease, equity, acceptability, feasibility, and other relevant factors. The GDG decided through an informal consensus process to adopt most recommendations however, there was a need to change the strength of 2 recommendations (B2 and B3) as they lack feasibility. Also, GDG/ GAG develops group of good practice statements to improve acceptability and feasibility.
➡️Implementation Tools and Considerations
To improve healthcare provision, quality, safety, and patient outcome, evidence-based recommendations must not only be developed, but also disseminated and implemented at national and local levels and integrated into clinical practice.
Dissemination involves educating related healthcare providers to improve their awareness, knowledge and understanding of the guideline’s recommendations. It is one part of implementation, which involved translation of evidence-based guidelines into real life practice with improvement of health outcomes for the patients.
Implementation requires an evidence-based strategy involving professional groups and stakeholders and should consider the local cultural and socioeconomic conditions. Cost-effectiveness of implementation programs should be assessed.
Specific steps need to be followed before clinical practice recommendations can be integrated into local clinical practice, particularly in low resource settings.
➡️Steps of implementing Type 2 Diabetes prevention strategies into the Egyptian health system:
1. Develop a multidisciplinary working group.
2. Assess the status of nutritional care delivery, care gaps and current needs.
3. Select the material to be implemented, agree on the main goals, identify the key recommendations for diagnosis, treatment and prevention and adapt them to the local context or environment.
4. Identify barriers to, and facilitators of implementation.
5. Select an implementation framework and its component strategies.
6. Develop a step-by-step implementation plan:
· Select the target populations and evaluate the outcome.
· Identify the local resources to support the implementation.
· Set timelines.
· Distribute the tasks to the members.
· Evaluate the outcomes.
7. Continuously review the progress and results to determine if the strategy requires modification.
➡️Guideline implementation strategies will focus on the following: -
1. For Practitioners
· Educational meetings: conferences, lectures, workshops, grand rounds, seminars, and symposia.
· Educational materials: printed or electronic information (software).
· Web-based education: computer-based educational activities.
· A trained person meets with providers in their practice setting to provide information with the intention of changing the provider’s practice. The information may include feedback on the performance of the provider(s).
· Reminders: the provision of information verbally, on papers or on a computer screen to prompt a health professional to recall information or to perform or avoid a particular action related to patient care.
· Optimize professional-patient interactions, through mass media campaigns, reminders, and education materials.
· Practice tools: tools designed to facilitate behavioral/practice changes, e.g., flow charts.
2. For Patients and care givers
· Patient education materials (Arabic booklet): Printed/electronic information aimed at the patient/consumer, family, caregivers, etc.
· Reminders: the provision of information verbally, on papers or electronically to remind a patient/consumer to perform a particular health-related behaviors.
· Mass media campaigns.
3. For Nurses
· Educational meetings: lectures, workshops or traineeships, seminars, and symposia.
· Educational materials: printed.
· A trained person meets with nurses in their practice setting to provide information with the intention of changing the provider’s practice.
· Reminders: the provision of information verbally, on paper or on a computer screen to prompt them to recall information or to perform or avoid a particular action related to patient care.
· Practice tools: tools designed to facilitate behavioral/practice changes.
4. For Stakeholders
Plans have been made to contact with all the health sectors in Egypt including all sectors of the Ministry of Health and Population, National Nutrition Institute, University Hospitals, Ministry of Interior, Ministry of Defense, Non-Governmental Organizations, Private sector, and all Health Care Facilities.
· Information and communication technology: Electronic decision support, order sets, care maps, electronic health records, office-based personal digital assistants, etc.
· Any summary of clinical provision of health care over a specified period may include recommendations for clinical action. The information is obtained from medical records, databases, or observations by patients. Summary may be targeted at the individual practitioner or the organization.
· Administrative policies and procedures.
· Formularies: Drug safety programs, electronic medication administration records.
5. Other activities to assist the implementation of the adapted guideline’s recommendations include:
· International initiative: Dissemination of the presented adapted CPG internationally via sending the final adapted CPG to the Guidelines International Network (GIN) Adaptation Working Group and contacting the CPG developers.
· Gantt chart has been designed to manage the dissemination and implementation stages for the adapted CPG over an accurate time frame (Appendix).
➡️Guideline Implementation Tools
Educational materials based on this Adapted CPG for treatment of CAP in children have been made available in several forms including:
1. Manual for physician for Blood pressure and Body mass index screening.
2. Algorithm for Type 2 diabetes screening.
References:
Samuels J, Samuel J. New guidelines for hypertension in children and adolescents. J Clin Hypertens (Greenwich). 2018;20(5):837-839. doi:10.1111/jch.13285
Flynn JT, Kaelber DC, Baker‐Smith CM, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017;140:e20171904.
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents . The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114:555‐576.
Magge SN, Silverstein J, Elder D, Nadeau K, Hannon TS. Evaluation and Treatment of Prediabetes in Youth. J Pediatr. 2020;219:11-22. doi:10.1016/j.jpeds.2019.12.061
https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age
Lifestyle recommendations for youth with T2D
Recommendations for screening of associated comorbidities/complications