
كتاب
Female Reproductive surgery in farm animals
1- Cesarean section
· Cesarean section (CS) involves the fetal extraction from the dam through a surgical incision in the abdominal wall and the uterus [1].
· It is commonly indicated in the cases of dystocia [11] which may be attributed to maternal or fetal causes.
· The maternal causes of dystocia include irreducible uterine torsion, hydropsy, narrow pelvis/pelvic fracture, incomplete cervical dilation, extra-uterine pregnancy, uterine inertia, uterine rupture, urinary bladder carcinoma, irreducible prolapse mass, and bicornual pregnancy. While the fetal causes include fetal abnormalities (hydrocephalus, fetal ascites, anasarca, cleft palate), fetal monsters, fetal mal-disposition, fetal oversize/emphysema, mummified fetus, and macerated fetus [10, 32].
· The cesarean section has several disadvantages including poor dam survival rates and poor fertility due to the increased incidence of peritonitis that leads to uterine adhesions and invariably results in animal death or infertility [1, 9].
· The rate of success of CS is affected by several factors including animal species, fetal viability, asepsis, and surgical technique and approaches [19].
The surgical approaches of cesarean section in different animals:
➡️1- Surgical approaches of cesarean section in cattle
There are different cesarean approaches in cattle [28] including;
1- Standing left paralumbar laparotomy.
2- Standing right paralumbar laparotomy.
3- Recumbent left paralumbar laparotomy.
4- Recumbent right paralumbar laparotomy.
5- Recumbent ventral midline laparotomy.
6- Ventral paramedian laparotomy.
7- Ventrolateral laparotomy.
8- Standing left oblique laparotomy.
The selection of the proper approach determines the anesthetic application technique and depends on the cow's health condition, type of dystocia, the surgeon’s preference, and availability of assistants [28]. The most common technique is the standing left paralumbar celiotomy [1, 28].
For details on methods of anesthesia, refer to Veterinary Anesthesia: - Acknowledgement | EHC | Egyptian Health Council
1- Standing left paralumbar laparotomy
A vertical incision is made in the middle of the left paralumbar fossa, approximately 10 cm ventral to the transverse processes of the lumbar vertebrae and continuing ventrally (Fig. 1) [28].
It has several advantages including its simplicity and easy closure of the abdominal wall, in addition, the rumen prevents small intestines evisceration during the surgery [19]. However, its disadvantage includes the difficulty of lifting the uterus and calf to the paralumbar incision [28].
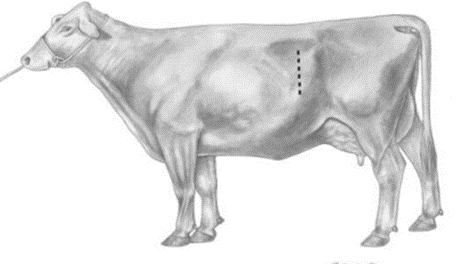
Figure (1). Standing left paralumbar celiotomy.
2- Standing right paralumbar laparotomy
· The surgical incision is made on the right paralumbar fossa in the same way as in the left paralumbar laparotomy.
· It is indicated in cases of a large calf in the right horn, a cow with severe adhesions on the left side due to repeated caesareans, and a cow with hydropsy [20].
· The main disadvantage of this approach is the difficulty of keeping the intestines in the peritoneal cavity with the right paralumbar approach [19].
3- Recumbent left paralumbar laparotomy
· The cow is casted and placed in right lateral recumbency, and the incision is made more ventral than in the standing left paralumbar laparotomy [15].
· This approach has several disadvantages including the more assistance required, the difficulty in exteriorization of the uterus, and the delayed closure of the incision due to increased tension on the muscle layers [28].
4- Recumbent right paralumbar laparotomy
It is similar to that of recumbent left paralumbar celiotomy. It has an additional complication which is the difficulty to keep the intestines in the peritoneal cavity [28].
5- Recumbent ventral midline laparotomy
· The cow is positioned in dorsal recumbency and the incision is performed 5–7 cm caudal to the umbilicus and extended caudally as required (Fig. 2) [28].
· It is indicated in the case of an emphysematous fetus [28]. It has several disadvantages including its limited application in older cows due to the increased size of the udder and the presence of increased ventral vasculature, in addition to the increased tension on the incision [1, 28, 29].
6- Recumbent ventral paramedian laparotomy
· The cow is put in dorsal recumbency and the incision is made 5 cm lateral and parallel to the linea alba and medial to the milk vein (Fig. 2).
· It has an advantage compared to the midline incision in that the abdominal wall closure is more secure [28].
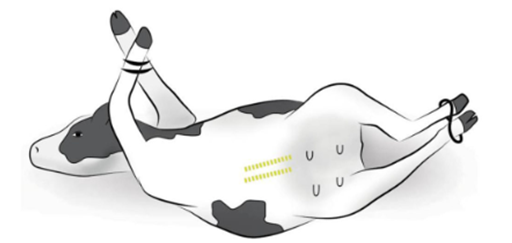
Figure (2). Recumbent ventral midline and paramedian celiotomy
7- Ventrolateral celiotomy
· The cow is positioned in the right lateral recumbency. A curved incision is made 20 cm dorsal to the udder, medial to the stifle fold, and about 50 cm cranio-ventrally (Fig. 3) [28].
· It has several advantages including the avoidance of vascularized musculature of the flank, does not require dorsal recumbency, and allows excellent exteriorization of the uterus. It is suited for older beef and dairy cows [19].
· The disadvantages are the difficult and less secure closure of the incision due to the increased tension, which may be prone to herniation and evisceration [28].
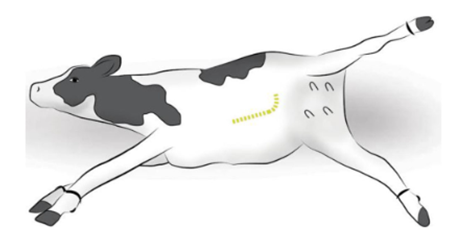
Figure (3) Ventrolateral celiotomy
8- Standing and recumbent left oblique celiotomy
· The incision is made 4-6 cm ventral and cranial to the tuber coxae and is extended cranioventrally toward the caudal rib (Fig. 4) [28].
· It has several advantages including relative accessibility to the apex of the uterine horn, easy exteriorization of the uterus, useful in case of a very heavy calf and the healing of the incision is rapid as the internal abdominal oblique muscle is incised parallel to the muscle fibers [1, 28].
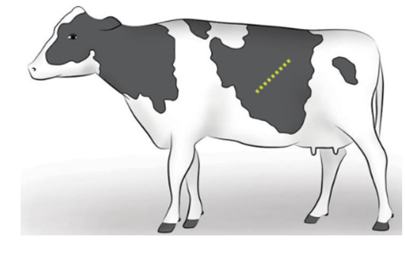
Figure (4) Standing left oblique celiotomy
➡️2- Surgical approaches of cesarean section in small ruminants
CS in the small ruminant can be performed through 2 techniques [6] including:
1. Left paralumbar approach.
2. Ventral midline approach.
The surgical approach chosen must include consideration of the dam and fetal health and the availability of support personnel. The ventral midline approach is preferred when uterine contents may be contaminated [33].
1- Left paralumbar approach.
It is the most common surgical approach in small ruminants [35]. The animal is positioned in the right lateral recumbency. The left flank is clipped and a vertical or slightly oblique 15–25 cm skin incision is made 10 cm below the transverse processes of the lumbar vertebrae centered in the paralumbar fossa [33]. The skin and the cutaneous trunci muscle are incised sharply; the external and internal abdominal oblique muscles are incised with either a scalpel blade or scissors. The uterus incision is made over the greater curvature of the uterus to minimize hemorrhage. The incision can be made directly over a fetal limb or a fetal head. The incision should be long enough to allow for the extraction of the largest portion of the fetus to minimize uterine tears [6].
2- Ventral midline approach.
The animal is positioned in dorsal recumbency and the ventral abdomen from the umbilicus to the cranial udder is surgically clipped. A skin incision is made just cranial to the udder and extended cranially 20–25 cm [6, 33].
➡️3- Surgical approaches of cesarean section in mares
Before cesarean, the mare undergoes a regime of anesthesia as follows; xylazine (0.8 mg/kg bwt, i.v.) followed by diazepam (0.04 mg/kg bwt, i.v.) and ketamine (2.2 mg/kg bwt, i.v.). To counteract the weight of the abdominal contents on the thorax, the animal is kept on halothane or isoflurane and oxygen, with ventilation. Intravenous fluids are administered together with other agents to maintain blood pressure [10]. For details on methods of anesthesia, refer to Veterinary Anesthesia: - Acknowledgement | EHC | Egyptian Health Council
There are several surgical approaches to CS in mare [31]:
1. Ventral midline approach
2. Modified low flank approach
3. Standing flank approaches
1- Ventral midline approach
It is the most frequently used incision in mares [10]. The mare is positioned in dorsal recumbency. A ventral midline incision (25 cm) is made into the abdomen, extending cranially from a point just caudal to the umbilicus.
The uterine horn is exteriorized and large stay sutures are made to stabilize the uterine horn during the procedure; one suture is made near the tip of the uterine horn close to the fetal limb, and one towards the body of the uterus, close to the point of the hocks. The exteriorized horn is isolated using drapes that prevent contamination from uterine contents. An incision is made between the 2 stay sutures through the uterine wall and chorioallantois from the level of the hock to the fetlock. The amniotic membrane is incised and the fetus is pulled from the hindlimbs out of the uterus. The umbilical cord is cut near the foal's body and the ends are clamped. The chorioallantois is separated from the endometrium for approximately 5 cm from its incised edges. Large blood vessels along the uterine incision are ligated. The uterus is sutured in 2 layers (the 1st layer is a simple continuous pattern and the second is a continuous Lembert pattern) using No. 2 polyglycolic acid suture material. The exteriorized uterine horn is rinsed with sterile saline and the contaminated drapes are removed. The abdominal cavity is rinsed with sterile saline and the fluids are removed by suction. The abdomen is closed as follows; Peritoneum and transverse abdominal muscles are sutured together with a double layer of No. 2 polyglycolic acid suture material using a simple interrupted pattern followed by a re-enforcing layer of lock stitch. Internal and external oblique abdominal muscles are sutured together by a lock stitch pattern using a double layer of absorbable suture material (No. 2). The skin incision is closed by an interrupted horizontal mattress pattern with nylon [21].
2- Modified low flank approach
The mare is positioned in the right lateral recumbency [34]. The incision is made in a cranio-dorsal to the caudo-ventral direction to the depth of the external abdominal oblique muscle. A grid approach through the external and internal abdominal oblique muscles and the transverse abdominal muscle is used to gain entry to the abdomen. The hysterotomy and fetal extraction proceed similarly to that explained above. Closure of the body wall entails suturing each muscle layer separately before closure of the fascia, subcutaneous tissue, and skin [10].
3- Standing flank approaches
A vertical skin incision (15 to 20 cm) is made approximately 5 cm ventral to the lumbar transverse processes, midway between the 18th rib and the tuber coxae in a cranial-caudal direction [27] (Fig. 5). The incision can be extended ventrally if needed. The incision usually is made on the left side unless surgical embryo transfer techniques are being performed. The skin and subcutaneous tissues are sharply incised. The external abdominal oblique is separated along the direction of its fibers. The internal abdominal oblique fibers are separated bluntly. The transversus muscle is sharply incised, and the peritoneum can either be sharply incised or bluntly separated.
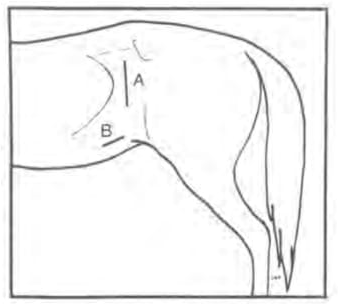
Figure (5). Diagrammatic representation of the left flank in a standing mare. (A): vertical skin incision, (B): oblique skin incision
