
Book
Female Reproductive surgery in farm animals
2- Ovariectomy
Ovariectomy is the surgical removal of the ovary in case of large ovarian tumors and adhesions involving the ovary [13]. It can be performed via a flank or ventral abdominal approach or more recently through standing laparoscopic ovariectomy [3, 25, 26, 30].
1- Surgical approaches of ovariectomy in cattle
There are two different ovariectomy approaches in cattle
1- The left flank approach
A vertical skin incision (30 cm) is made over the left paralumbar fossa extending. All muscular layers were incised with the scalpel. The peritoneum was held with forceps, punctured with the scalpel, and incised with scissors proximally and distally. The uterus and the ovaries are grasped and located 5 cm cranial to the pelvic wall. Lidocaine (2%) is sprayed over the ovarian pedicle and the preformed knot ligates the ovary. After ligation, the ovary can be removed using curved Mayo scissors, and the ovarian pedicle is inspected for hemorrhage. The abdominal is sutured as in the cesarean section [25].
2- Laparoscopic ovariectomy
The cow is restrained in standing stocks and sedated with an I.M. injection of 0.05 mg/kg BW xylazine. The left paralumbar fossa from the transverse processes of the lumbar vertebrae to the level of the stifle and from the second last rib to the level of the tuber coxae was clipped, shaved, and aseptically prepared. Local infiltration with 10 ml of 2% lidocaine is performed in the subcutaneous and muscular tissue of the portal sites. The laparoscopic portal is made at the ventral angle of the paralumbar fossa, approximately 10 cm ventral to a line horizontally drawn through the tuber coxae and at the transition from the middle to the caudal third of the flank (Fig. 6). A vertical skin incision (2cm) is made at this site, and a security obturator is advanced through the musculature and peritoneum until air influx could be heard entering the abdominal cavity. A trocar-cannula unit (20 cm) with an air valve is introduced through the obturator and connected to a carbon dioxide insufflator. The laparoscope is inserted through the trocar. The abdomen is insufflated with carbon dioxide to an intraabdominal pressure of 5–10 mmHg. The two instrument portals, located 20 and 30 cm ventral to the tuber coxae (Fig. 6), are placed under endoscopic guidance. The uterus is identified and the ipsilateral uterine horn is grasped at its greater curvature with grasping forceps (43 cm long with locking handles). The uterine horn is gently pulled cranially, and the ovary within the bursa becomes visible and is grasped with claw forceps (43 cm long with locking handles). The grasping forceps is replaced by an injection cannula through which 20-30 ml 2% lidocaine is injected into different locations inside the mesovarium and mesosalpinx. The injection cannula is replaced with bipolar cauterizing forceps which is placed on the mesovarium 0.5 cm proximal to the ovary. The mesovarium is cauterized until a white discoloration, shrinkage or blister formation can be observed (Fig. 7). The proper ovarian ligament, is then cut with serrated curved scissors (Fig. 8) grasping forceps holding the ovary were pulled to the abdominal wall. The carbon dioxide is allowed to escape through the portals, the peritoneum and external oblique muscle are closed with simple interrupted sutures of five metric polydioxanones, and the skin is closed with simple interrupted sutures of four metric polyamide. The cows should undergo daily clinical and sonographic examinations for the first 5 days post-operatively and then twice a week until 30 days after surgery [3].
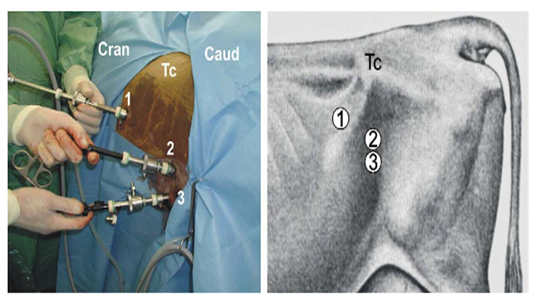
Fig. 6. Portals for laparoscopic ovariectomy via the left flank in a standing cow. TC: tuber coxae, 1: endoscope portal, 2: first instrument portal, 3: second instrument portal [3].
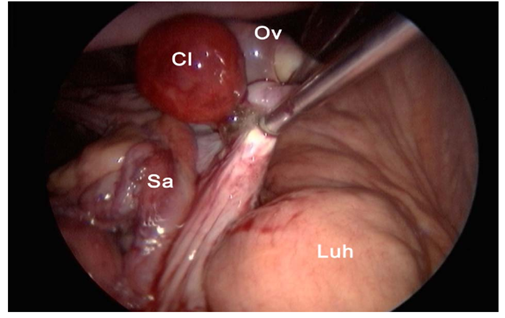
Fig. 7. Cauterization of the mesovarium using cauterization forceps. Cl: corpus luteum, Ov: ovary, Sa: salpinx, Luh: left uterine horn [3].
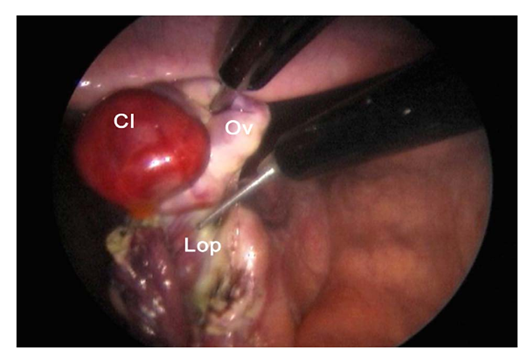
Fig. 8. Transection of the proper ovarian ligament (lop). Cl: corpus luteum, Ov: ovary [3].
2- Surgical approaches of ovariectomy in small Ruminants
There are two different ovariectomy approaches in small ruminants.
1- Ventral midline approach
Ovariectomy is easily performed on the anesthetized animal placed in dorsal recumbency. A small incision (6- 8 cm) is made in the ventral midline just cranial to the udder and continues into the abdominal cavity. The urinary bladder and the uterus are recognized and the uterine horns are exteriorized by gentle traction. For hysterectomy or ovariohysterectomy, the mesometrium is transected after ligation of small blood vessels. The uterus is transected at the level of the body. A circumferential trans-fixation ligature of absorbable suture material is placed close to the cervix. If the remaining portion of the uterine body is large, it should be closed with an inverting suture pattern before replacing it in the abdomen. The vasculature supplying the ovary and horn on one side are ligated and transected. The remaining uterus is closed with an inverting pattern. Some advocate a two-layer uterine closure [33].
2- Laparoscopic approach
Laparoscopy is usually performed on the sedated animal in dorsal recumbency on a cradle that can be tilted. Animals should be fasted for at least 12 hours to reduce rumen fill and the possibility of regurgitation. An area (25 cm x 25 cm) cranial to the mammary gland is prepared by clipping and surgical scrubbing. Three portals are necessary: one each for the laparoscope, a manipulation instrument, and special instruments (insemination gun, suture material). The site of the desired portals is infiltrated with a local anesthetic before introducing a trocar and cannula. For simple technique, the portals are created by making a small skin incision to allow trocar introduction. Visualizing the abdominal viscera requires insufflation with CO2 and elevating the hindquarters to a 40° angle [33]. The rest of the technique is performed as in cattle.
3- Surgical approaches of ovariectomy in mares
There are two different Ovariectomy approaches in mare
1- Flank Approach
The flank ovariectomy approach can be performed in the standing or recumbent position. To perform a standing flank laparotomy, the mare is sedated, and restrained in standing stocks, and the tail is wrapped. The recumbent flank technique requires general anesthesia, resulting in a greater cost and potentially increased risk to the mare. It is generally only used for unilateral ovariectomy, as it offers easy access to only one ovary [5]. The mares are placed in lateral recumbency so that the ovary to be removed is upper-most [16].
The paralumbar fossa is clipped, aseptically prepared, and draped. Regional anesthesia in the form of an inverted L-block or local infiltration of the proposed incision site is required. The incision is started 5 cm ventral to the lumbar transverse processes between the 18th rib and the tuber coxae and is extended ventrally 10 to 15 cm (Fig. 9). Following incision of the skin and subcutaneous tissues, a grid or modified grid approach is used to incise the abdominal musculature. The grid approach involves separating the external abdominal oblique muscle along the direction of its fibers, whereas a modified grid technique involves incising this muscle along the line of the skin incision. The internal abdominal oblique and transversus abdominis muscles are bluntly separated along the direction of their fibers. The peritoneum may be incised or bluntly perforated to allow access to the abdomen, and the ovary is identified and isolated. In standing mares, the mesovarium is anesthetized by topical administration of anesthetic or by direct injection of anesthetic into the mesovarium. The ovary may be transected within the abdomen or after exteriorization. Following removal of the ovary, the mesovarium is observed for hemorrhage and oversewn if required. Closure of the laparotomy incision is routine. Postoperative pain and discomfort may be observed in association with the flank incision. Incisional swelling and discharge may be noted 24 to 72 hours after surgery [16].
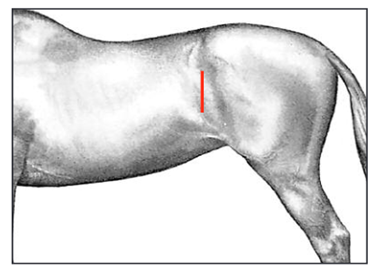
Fig. 9. Position of paralumbar flank incision (in both standing and recumbent horses) for ovariectomy between the 18th rib and tuber coxae [16].
2- Laparoscopic Techniques
Mares are sedated using either xylazine hydrochloride or detomidine hydrochloride in combination with butorphanol tartrate. For bilateral ovariectomy, both paralumbar fossae are prepared for aseptic surgery and draped [16]. The paralumbar fossa is desensitized using regional anesthesia or by direct infiltration of the proposed laparoscope and instrument portal sites [17]. The abdominal cavity can be insufflated with carbon dioxide the trocar–cannula [4]. A 15 mm skin incision is made at the dorsal border of the internal abdominal oblique muscle, and the sharp laparoscopic trocar–cannula is introduced into the abdominal cavity perpendicular to the paralumbar fossa (Fig. 10). The trocar is replaced by the laparoscope, and the ovary is identified. The first portal is made 4 to 8 cm ventral to the laparoscope portal, and a second portal is made 4 to 8 cm ventral to the first (Fig. 11). The mesovarium is infiltrated with a local anesthetic using a long spinal needle. Hemostasis of the mesovarium can be achieved using suture ligatures. The ovary is transected using laparoscopic scissors distal to the site of ligation or coagulation. After removing the ovary, the abdomen is deflated through a laparoscopic cannula. The superficial abdominal fascia and skin at the portals are closed separately [16].
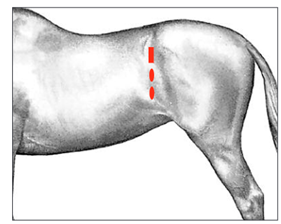
Fig. 10. Position of the laparoscope (rectangle) and instrument portals (ovals) for laparoscopic ovariectomy in the standing horse. The laparoscope portal is positioned between the 18th rib and the tuber coxae, just dorsal to the crus of the internal abdominal oblique muscle. Instrument portals are created 4 to 8 cm ventral to the laparoscope portal [16].
