
Book
Female Reproductive surgery in farm animals
3- Caslickʾs operation
Caslick’s operation is indicated when malformation or inadequate closure of the vulva (Fig. 11) is present. The compromised vulval seal is associated with pneumovagina, or wind sucking, which can predispose ascending contamination and infection. Contamination of the caudal reproductive tract can initially cause vaginitis, which may extend to induce acute endometritis and, in late gestation, will predispose placentitis [14, 22]. The inadequate closure of the vulva is attributed to several causes including trauma during foaling, weight loss, or congenital deviation from the ideal conformation, ageing, and poor body condition score [8, 18]. Moreover, poor vulval conformation is predisposed in mares with a flat-topped croup and a tail setting level with the sacroiliac joint [8, 23].
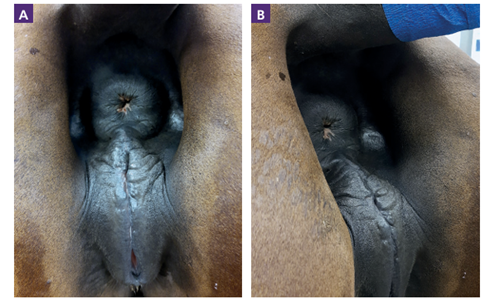
Figure 11. Vulval malconformation in a mare. A cranial sloping of the dorsal commissure of the vulva due to a sunken anus [2]. B: before correction, A: after correction.
The vulval malconformation can be diagnosed and assessed by the Caslick’s index [23]. It is the only way to objectively quantify the degree of abnormality and correlates positively with the likelihood of developing pneumovagina [7, 8, 23]. It is calculated by multiplying the effective length of the vulva in centimeters by the angle of declination of the vulva in degrees [7, 23]. A value of >150 is considered indicative of the need for a Caslick’s vulvoplasty [8, 24]. The need for a Caslick’s operation is suggested by a positive wind sucker test (parting the vulval labia and listening to the sound of air rushing into the vagina), which indicates an in competent vestibulovaginal fold, or the detection of air in the vagina and uterus during per rectum ultrasound examination [8].
Procedures of Caslick’s operation:
Caslick’s operation should be performed on the standing, restrained mare under local anesthesia. Adequate restraint can be achieved by placing the mare in examination stocks, using a twitch and/or by positioning the back-end of the mare just inside a stable door (Bradecamp, 2011). The mare’s rectum should be emptied, with the tail bandaged and held or tied to one side. The perineal region should then be gently cleaned with disinfectant soap such as povidone iodine soap, dried with paper towels or cotton, and prepared with a minimally-irritant antiseptic solution (0.5% chlorhexidine or 30% alcohol). About 15–20ml of local anesthetic (2% lidocaine) should be injected subcutaneously using a 20-gauge or smaller needle along the mucocutaneous junction of both vulval labia, starting at the most ventral aspect of the proposed vulvoplasty and progressing to the dorsal commissure of the vulva (2), (Fig. 12).
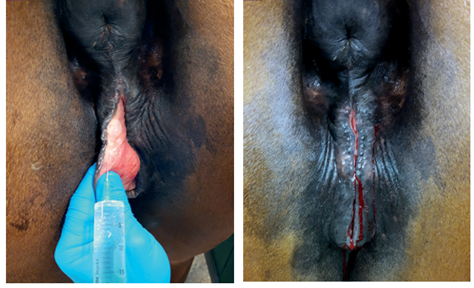
Figure 12. Subcutaneous injection of 2% Lidocaine along the mucocutaneous junction of both labia [2].
The ventral extent of the Caslick’s operation should continue to about 2–3cm below the level of the ischial tuberosities, and in the case of a cranially sloping vulva, to below the level where the vulva orifice assumes a vertical orientation. At least 3cm of the vulva must be left open to allow unconstrained urination. A thin strip of mucosa is removed from the mucocutaneous junction of the labial rim using tissue scissors, to expose a strip of submucosa around 8–10mm wide. To allow removal of the tissue, thumb forceps can be used to grasp a ribbon of mucosa [12]. Care should be taken that the dorsal commissure is not omitted, by creating a wound with an inverted U-shape. The labia are sutured together to oppose the freshly created wounds using either a simple continuous, interrupted or continuous interlocking suture pattern (Bradecamp, 2011). It is advisable to use a suture material of approximate size 0 (4 metric) with a curved, round bodied, sharp needle. Suture material can be either absorbable (Vicryl), or non-absorbable (Ethilon). The suture should pass through the middle to deep part of the incised tissue to ensure adequate healing and minimize the risk of fistula formation (Fig. 13). In addition, the sutures should exit the skin approximately 1cm away from the labial rim to prevent them tearing through. The individual stitches should be placed 0.5–1cm apart to avoid gaps and fistula formation (Fig. 14). For a regular Caslick’s procedure, postoperative topical or systemic antibiotics are not indicated [12]. Aftercare includes avoiding or minimizing rectal palpation and manipulation of the surgical field for 10–14 days. Remove the sutures after 7–14 days if non-absorbable suture material is used. To prevent tearing of the vulva at foaling, a Caslick’s operation should be reopened shortly before parturition (less than 14 days before the estimated date of birth) [12]. Opening requires sufficient local anesthesia and involves a straight cut in the direction of the scar between the opposed labia, using either tissue scissors or a scalpel. Postpartum, a Caslick’s operation can be repeated 1–2 days after parturition [12], or after the foal heat, with assurance that the mare has no fluid in the uterus and is no longer at risk of postpartum metritis.

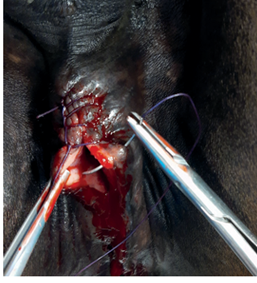
Figure 13. A thin strip of mucosa is removed from the mucocutaneous junction, creating an approximately 8–10mm wide strip of exposed submucosa. The labia are sutured using a simple interrupted, continuous or continuous interlocking suture pattern and exit approximately 1cm from the labial rim (c)

Figure 14. Caslick’s procedure using an interlocking suture technique. Adequate closure can be checked by inserting a finger and applying gentle pressure to the suture from the vaginal aspect.
