Book
Female Reproductive surgery in farm animals
4- Perineal lacerations
Perineal (rectovaginal) lacerations occur in different species but are more common in mares [36]. Most lacerations arise at the time of foaling due to excessive manipulation during assisted delivery for extraction of the oversized or malpositioned fetus [37]. Depending on their extent, the perineal lacerations have been classified into 3 grades: first, second, and third-grade lacerations as follows [38]:
First-grade laceration: involves the skin of the vulval dorsal commissure and mucosa of the vestibule.
Second-grade lacerations: compromise the closure of the labia and predispose to pneumovagina. Extend through the perineal body, and involve the mucosa and submucosa of the vestibule and the constrictor vulvae muscle. If the perineal body is not reconstructed, the mare will develop a sunken perineum and be predisposed to pneumovagina and urovagina.
Third-grade lacerations: occur penetration of the rectum, perineal body, and anal sphincter, resulting in a complete loss of barrier between the rectum and vestibule (Fig. 15) resulting in a common passage for urination and defecation [38]. The fecal contamination of the reproductive tract results in vaginitis and endometritis. In addition, the loss of the constrictor vulva muscle or a functional rectal sphincter leads to a "wind sucker" during exercise that causes unattractive noise and leads to pneumovagina and further bacterial dissemination to the reproductive tract.

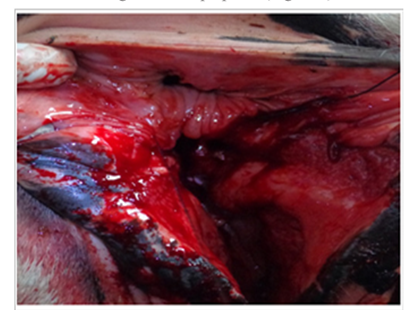
Figure 15. 3rd grade of perineal lacerations with separate shelf for rectum & vagina [38].
Treatment
First-grade injuries do not require surgical intervention. If needed, a Caslickʾs procedure can be performed [37].
Second and third-grade injuries require a Caslickʾs procedure and reconstruction of the perineal body.
In third-grade injuries, the management of the laceration includes 2 parts: immediate treatment and delayed surgical repair [39]. The initial therapy includes daily wound care and cleaning of the contaminated tissues with diluted povidone-iodine solution for ten days to allow subsidization of the perineal swelling. The animal is administered tetanus toxoid along with antibiotics, anti-inflammatory, and anti-histaminic [38].
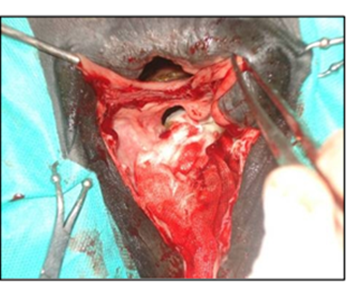
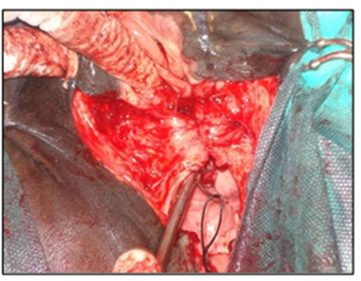
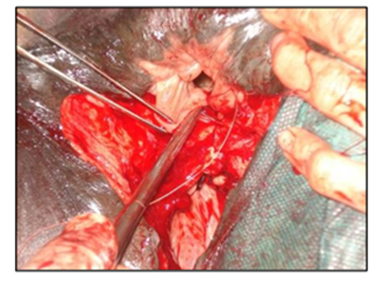
The surgical repair of the perineal body is applied after 10-15 days until the perineal swelling is completely subsided. The mare is controlled in a standing position and sedated with xylazine (5-10ml, slow i.v. route) together with epidural anesthesia with the injection of 5-10ml lignocaine Hcl in between the 1st & 2nd intra-coccygeal space. The perineal area is prepared for the surgery with povidone-iodine and the anus, perineum, and vulvar lips are retracted with towel clamps (Fig. 16). A combination of sharp and blunt dissection is used to separate the tissue into rectal (two-thirds of the thickness) and vestibular shelves (one-third of the thickness). The dissection is continued cranially for 3 to 5 cm and laterally until the tissue shelves can be opposed on the midline without tension (Fig. 17). The septum between the rectum and vagina was sutured by a six-bite pattern using a nonabsorbable suture material (No. 2) (Fig. 18). The rectal mucosa is sutured with simple interrupted suturing using 0 vicryl (Fig. 19). The skin of the perineal body is sutured with non-absorbable suture material (No. 2) in a horizontal mattress pattern (Fig. 20) [37, 38].
|
|
|
|
|
|
|
Figure 20. The skin of the perineal body was closed with non-absorbable suture material (No. 2) in a horizontal mattress pattern [38].
|
|