Book
intensive care unit admission, discharge, and triage.
- Recommendations
|
Recommendations |
Reference |
|
General considerations |
|
|
We recommend that critically ill patients be transferred from the emergency department ,ward bed or Intermediate Care Units (IMCUs) to an available Intensive Care Unit (ICU) bed as rapidly as possible, ideally in less than or equal to 1 hour from the time the ICU bed is confirmed available and the decision to transfer is finalized. This is to minimize delays in accessing specialized ICU monitoring and interventions and to reduce potential risks associated with prolonged holding in non-ICU environments (Strong recommendation, low-quality evidence). |
1,2 |
|
We recommend that in circumstances where a critically ill patient requires ICU services that are unavailable within the current hospital or cannot be provided in a timely manner, clinicians immediately utilize officially established national or regional referral pathways to facilitate rapid assessment and transfer to an appropriate ICU. In Egypt, this includes contacting the National Project of Critical Care, Neonatal, and Emergency Services "Rayat Misr" through its designated electronic platform or emergency hotline (137) as per national protocols (Strong recommendation, low -quality evidence). |
1,2,3,4,5,6,7 |
|
We recommend that individual hospitals and their Intensive Care Unit (ICU) leadership formulate and regularly review explicit ICU admission and triage policies follow this guidline. These policies should be tailored to their specific institutional context, including the scope of clinical services provided (e.g., trauma, burn, neurocritical care, hepatic care), the demographic characteristics of their patient population, current ICU capacity, and available therapeutic resources (Strong recommendation, moderate-quality evidence). |
1,8,9,10 |
|
We suggest that Triage decisions must be made transparently and without any prejudice. Factors like ethnicity, race, sex, social standing, or financial resources are wholly irrelevant. (Good practice statement, low-quality evidence). |
1,8,9,10 |
|
We recommend that hospitals and their ICU leadership develop, implement, and regularly review explicit, transparent, and fair policies for the triage and allocation of ICU beds. These policies should provide a clear framework for balancing scheduled postoperative admissions with emergency admissions. This includes defining a process for temporarily reserving beds for imminent high-risk surgical arrivals while also having a dynamic override mechanism, managed by a designated triage officer or clinical leader (e.g., ICU director), to ensure any patient with an immediate life-threatening condition can access a necessary bed with minimal delay. Unjustified or prolonged reservation of an empty ICU bed in the face of a critically ill patient needing admission is inconsistent with ethical principles of justice and beneficence (Strong recommendation, moderate-quality evidence). The core issue is one of triage and resource allocation. An ICU bed is a scarce, high-cost resource. A structured, transparent policy is essential to:
|
1,2, 11 |
|
We recommend that hospitals, where feasible and appropriate based on patient population needs, establish Intermediate Care Units (IMCUs). These units should serve as a bridge between the general ward and the Intensive Care Unit to provide enhanced monitoring and a higher level of nursing care for two primary patient groups: those who no longer require intensive care but are too unstable for the general ward (step-down), and those who are deteriorating on the ward but may not require immediate ICU-level organ support (step-up). The implementation of IMCUs is intended to improve patient safety, reduce ICU readmissions, optimize the use of critical care beds, and potentially lower overall costs for specific high-risk patient populations. (Strong recommendation, moderate-quality evidence). The optimization of hospital resources while ensuring patient safety represents a significant challenge in modern healthcare. A critical gap often exists between the high-intensity, resource-heavy environment of the Intensive Care Unit (ICU) and the standard monitoring available on a general medical or surgical ward. Intermediate Care Units (IMCUs), also known as Step-Down or High-Dependency Units, are designed to bridge this gap, offering a level of care for patients who are too ill or unstable for the general ward but do not require the advanced organ support of an ICU. |
12,13,14,15, 390 |
|
We recommend that hospitals develop and implement a Rapid Response System to facilitate early identification, bedside assessment, and appropriate triage of clinically deteriorating patients on general wards. This system should include a clear set of vital sign-based trigger criteria (such as: Modified Early Warning Score ) Fig. 1 and a designated team with critical care skills to respond promptly Rapid Response Team (RRT). A primary function of this team should be to stabilize the patient and facilitate timely and appropriate admission to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) when indicated (Strong recommendation, High-quality evidence). A key element of contemporary patient safety programs is the Rapid Response System (RRS). Its purpose is to recognize and intervene with patients whose condition is worsening, aiming to prevent serious adverse events like cardiac arrest. This forward-thinking strategy has demonstrated a reduction in hospital deaths and an enhancement of patient results. Putting a successful RRS into practice involves several key aspects: straightforward activation standards, a specialized and capable response team, thorough training for all staff, and a dedication to ongoing quality enhancement. This guide details the fundamental elements and stages for creating and rolling out a successful Rapid response System in a hospital environment. The Four Cornerstones of a Rapid Response System An effective RRS is founded on four interrelated cornerstones:
|
16, 17, 18 ,19 ,20, 21, 22, 23,26, 27, 353, 391 |
|
We recommend that RRSs be utilized for early review of acutely ill non-ICU patients to identify patients who need or would benefit from ICU admission and treatment and to prevent unnecessary ICU admissions (Strong recommendation, moderate-quality evidence). When a patient on a general ward triggers the RRS—often due to concerning changes in vital signs, respiratory distress, or altered mental status—a team of critical care experts, typically including an ICU nurse, a respiratory therapist, and sometimes a critical care physician or advanced practice provider, is dispatched to the patient's bedside. The RRS team conducts a rapid but comprehensive assessment that goes beyond a simple review of vital signs. This evaluation is tailored to the patient's specific presentation and may include:
The decision to transfer a patient to the ICU is not based on a single parameter but is a complex clinical judgment made by the RRS team in collaboration with the primary medical team. The core of this decision-making process revolves around three key questions: 1. Does the patient require advanced organ support? This is a primary driver for ICU admission and includes the need for mechanical ventilation, vasopressors to support blood pressure, or renal replacement therapy. The RRS team's critical care expertise is vital in identifying the subtle signs that a patient is heading towards requiring such interventions. 2. Would the patient benefit from the level of monitoring available only in the ICU? Some patients may not immediately require invasive interventions but are at high risk of rapid deterioration. The continuous monitoring of vital signs, cardiac rhythms, and other physiological parameters in the ICU can be life-saving for these individuals. A key function of the RRS is to act as an "ICU without walls," bringing critical care expertise to the patient's bedside and often preventing the need for a physical transfer to the ICU. The RRS can achieve this through several interventions:
|
23, 24, 25, 26, 27, 391 |
|
We recommend implementing ICU consult teams to support ward/IMCU staff with deteriorating patients, facilitate transfer to ICU, and reduce ICU readmission rates. (Good practice statement, low-quality evidence). |
1, 26, 27, 28, 29, 30 |
|
Admission & Triage |
|
|
We suggest using the following tools for bed allocation during the admission and triage processes(Good practice statement, low-quality evidence). : Guide to resource allocation of intensive monitoring and care including levels of monitoring, care, and nursing ratios (table 2) ICU Admission Prioritization framework(table 3) |
1, 17, 18, 31, 32 |
|
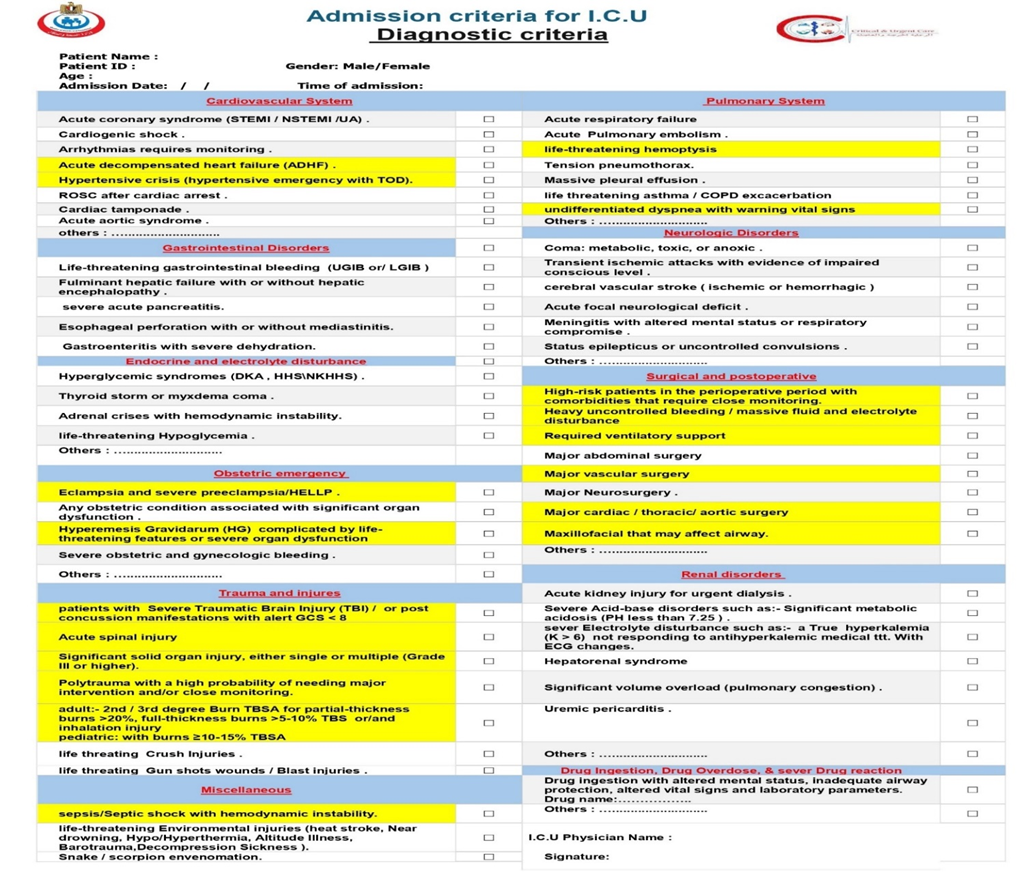
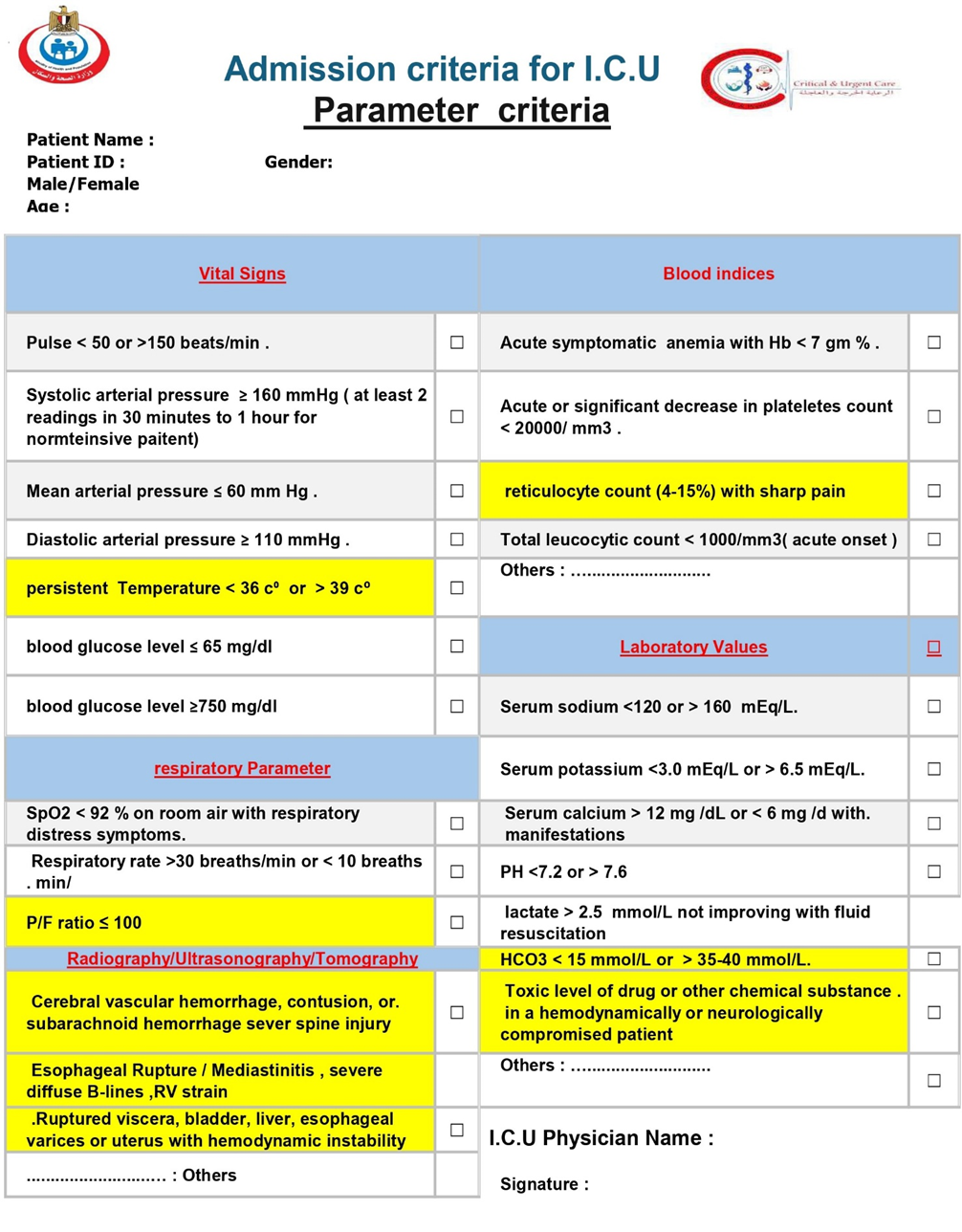
We suggest using the following tools as core of addmsion and discharge criteria checklist(Good practice statement, low-quality evidence): 1- addmsion checklist (table 4,5)
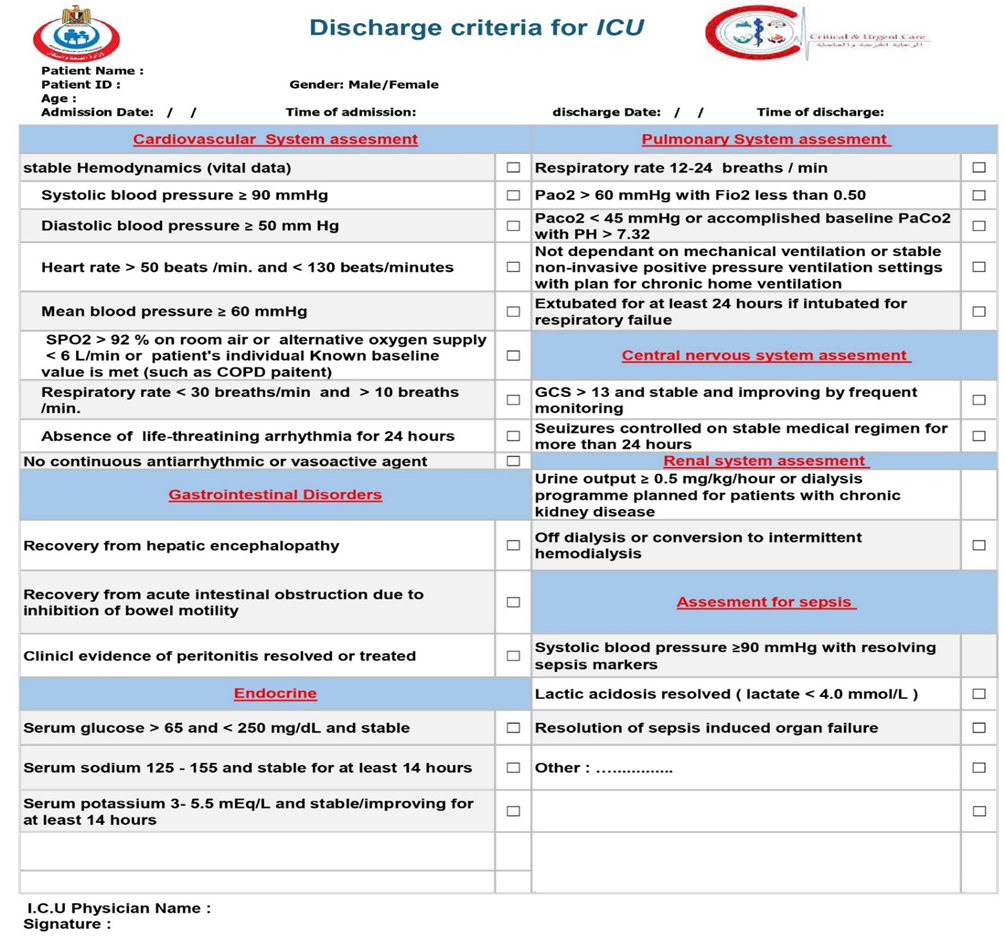
2- discharge criteria checklist(table 6):
|
1, 13, 27, 33, 35, 418 |
|
We recommend that the Acute Physiology and Chronic Health Evaluation (APACHE II) score, or a similar validated illness severity scoring system, be used as an adjunct to clinical assessment for patients being considered for Intensive Care Unit (ICU) admission. The calculation of an APACHE score upon presentation to the emergency department or for deteriorating ED/ward patients can provide valuable, objective information regarding the severity of illness and risk of mortality. A high or significantly rising score should be considered a strong indicator for the need for ICU-level care, facilitating timely and appropriate triage, especially for patients with conditions known to have a high mortality risk such as sepsis, acute respiratory distress syndrome (ARDS), and major trauma. It is crucial to emphasize that the APACHE score should not be used in isolation to determine ICU admission or discharge. It is a decision-support tool that, when integrated with a comprehensive clinical evaluation, patient preferences, and the overall clinical context, can lead to more informed and effective patient care.(Good practice statement, low-quality evidence). |
34 ,36, 37, 38 |
|
We recommended that patients with invasive mechanical ventilation or complex life-threatening conditions, including sepsis, receive care in an ICU. Additionally, weaning from mechanical ventilation should be restricted to an ICU or In necessities step down to a intermediate care unit (IMCU) , and not take place on a general ward. (Strong recommendation, moderate-quality evidence). |
1, 33, 39 |
|
We suggest avoiding admitting to a specialized ICU patients with a primary diagnosis not associated with that specialty (i.e., boarding) (Strong recommendation, moderate-quality evidence). |
1, 40, 285 |
|
Triage |
|
|
We suggest that hospitals and ICU leaders develop and implement admission and triage policies that are designed to minimize under-triage and overtriage is more acceptable (Good practice statement, low-quality evidence). Rationale for the Principle of Preferring Over-Triage: This principle is a cornerstone of patient safety in emergency and critical care triage. It acknowledges the different consequences of the two types of triage errors:
|
1, 2, 17, 24, 41 |
|
Diagnostic criteria |
|
|
We recommend that all patients presenting with ST-Elevation Myocardial Infarction (STEMI), ST-Elevation Myocardial Infarction (STEMI), Non-ST-Elevation Myocardial Infarction (NSTEMI) and other patients with Acute Coronary Syndromes (ACS) identified as high-risk (based on clinical features, ECG findings, cardiac biomarkers, hemodynamic instability, life-threatening arrhythmias, ongoing ischemia, acute heart failure and validated risk scores) be admitted to a Coronary Care Unit (CCU) an Intensive Care Unit (ICU), or an intermediate care unit (IMCU) with. This setting is necessary for continuous cardiac and hemodynamic monitoring, prompt management of life-threatening complications facilitation of timely reperfusion or invasive strategies, and optimization of medical therapy that require Intensive care, such as heart failure, cardiogenic shock, or serious arrhythmias, ventricular septal rupture, even if their initial condition appears stable, facilitation of timely reperfusion/revascularization strategies, and optimization of medical therapy (Strong recommendation, moderate-quality evidence). The primary purpose of admitting high-risk ACS patients to an ICU/CCU is to provide intensive monitoring and immediate intervention for life-threatening complications that are most common in the early hours and days after the acute event.
|
33, 42, 43, 44, 45, 46, 47, 48 |
|
We recommend that all patients diagnosed with cardiogenic shock characterized by persistent hypotension despite adequate fluid status and signs of end-organ hypoperfusion. be immediately admitted to an to a Coronary Care Unit (CCU) or Intensive Care Unit (ICU) or a specialized cardiac/cardiovascular ICU with equivalent capabilities This is to facilitate immediate and continuous hemodynamic monitoring, aggressive management with intravenous vasoactive medications, advanced respiratory support, rapid investigation and treatment of the underlying cause, and consideration for mechanical circulatory support (Strong recommendation, moderate-quality evidence). Admition is considered essential due to the need for:
|
33, 42, 43, 44, 45, 46, 47,49, 50, 51, 52, 53, 54 |
|
We recommend that patients presenting with arrhythmias be admitted to an a specialized Coronary Care Unit (CCU) or Intensive Care Unit (ICU) if the arrhythmia is life-threatening (e.g., sustained ventricular tachycardia, ventricular fibrillation, symptomatic high-grade atrioventricular block), causes hemodynamic instability (e.g., hypotension, shock, acute heart failure), is associated with severe symptoms directly attributable to the arrhythmia (e.g., syncope with a high-risk rhythm), or requires urgent electrical interventions (cardioversion, defibrillation, pacing) or pharmacological interventions with intravenous agents that necessitate continuous cardiorespiratory monitoring not feasible or safe in a lower-acuity setting (Strong recommendation, moderate-quality evidence). Patients with specific arrhythmias are admitted to an ICU/CCU due to:
|
33, 55, 56, 57, 58, 358 |
|
We recommend that patients with acute decompensated heart failure (ADHF) who exhibit signs of hemodynamic instability (e.g., hypotension, cardiogenic shock), severe respiratory distress or failure (requiring non-invasive or invasive mechanical ventilation), life-threatening arrhythmias, or who require intravenous vasoactive medications or invasive hemodynamic monitoring, be admitted to an Intensive Care Unit (ICU) or a Intensive Coronary Care Unit (CCU) for intensive management and monitoring (Strong recommendation, moderate-quality evidence). ADHF represents a spectrum of clinical severity. While many patients can be managed on general medical wards, those with severe ADHF require ICU/CCU admission due to:
|
33, 48, 49, 59, 60, 358 |
|
We recommend that patients presenting with a hypertensive emergency (defined as severely elevated blood pressure accompanied by acute, ongoing target organ damage) be admitted to an Intensive Care Unit (ICU) or a Intensive Coronary Care Unit (CCU) or a comparable high-acuity monitored setting. This is to facilitate immediate and controlled parenteral antihypertensive therapy, continuous (often invasive) blood pressure monitoring, and close observation and management of specific target organ dysfunction (Strong recommendation, moderate-quality evidence). It is vital to differentiate:
Patients with hypertensive emergencies require ICU admission due to the need for:
|
33, 61, 62, 63, 64, 65 |
|
We recommend that adult patients who achieve Return of Spontaneous Circulation (ROSC) after cardiac arrest and remain comatose or hemodynamically unstable, or who require ongoing ventilatory support, be admitted to an Intensive Care Unit (ICU) or a Coronary Care Unit (CCU) with equivalent ICU capabilities for comprehensive post-resuscitation care (Strong recommendation, moderate-quality evidence). Patients who achieve ROSC after cardiac arrest are critically ill and suffer from post-cardiac arrest syndrome. This complex syndrome includes:
Management of these patients in an ICU is essential for:
|
33, 66, 67, 68, 69 |
|
We recommend that patients diagnosed with cardiac tamponade, especially those exhibiting hemodynamic instability or requiring urgent pericardial drainage, be admitted to an Intensive Care Unit (ICU) or a Coronary Care Unit (CCU) with equivalent capabilities for continuous cardiorespiratory monitoring, management of potential complications, and further diagnostic evaluation and treatment of the underlying cause (Strong recommendation, moderate-quality evidence) Admission to an ICU/CCU is generally indicated for patients with cardiac tamponade, particularly if they exhibit hemodynamic compromise, due to the need for:
|
33, 70, 71, 72 |
|
We recommend that all patients diagnosed with or strongly suspected of having an Acute Aortic Syndrome (including aortic dissection, intramural hematoma, or penetrating atherosclerotic ulcer) be immediately admitted to an Intensive Care Unit (ICU) or a specialized cardiovascular ICU capable of providing comprehensive medical and peri-interventional management (Strong recommendation, moderate-quality evidence). AAS encompasses a group of life-threatening conditions including aortic dissection (AD), intramural hematoma (IMH), and penetrating atherosclerotic ulcer (PAU). These conditions are medical emergencies due to the high risk of aortic rupture, end-organ malperfusion, and death. Patients diagnosed with or strongly suspected of having AAS require immediate admission to an ICU or a specialized cardiovascular ICU. This is critical due to the need for:
|
33, 73, 74, 75, 76, 77, 78 |
|
We recommend that adult
patients presenting with sever valvular heart disease such as severe
acute mitral regurgitation, particularly when characterized by signs of
respiratory failure (e.g., pulmonary edema requiring advanced respiratory
support) or hemodynamic instability (e.g., hypotension, shock), be promptly
admitted to an Intensive Care Unit (ICU) or a specialized Cardiovascular/Coronary
Care Unit (CVICU/CCU). This is to facilitate immediate hemodynamic
stabilization with intravenous vasoactive medications (vasodilators and/or
inotropes), advanced respiratory support (non-invasive or invasive
ventilation), intensive monitoring, and optimization as a bridge to urgent
surgical intervention, which is the definitive therapy (Strong
recommendation, moderate-quality evidence). ICU/CCU admission is critical for patients with hemodynamically significant AMR due to the need for:
|
33,53, 54, 420, 421, 422, 423, 424, 425 |
|
Gastrointestinal Disorders |
|
|
We recommend that patients presenting with life-threatening gastrointestinal bleeding (UGIB or LGIB), characterized by hemodynamic instability (e.g., shock, persistent hypotension despite initial resuscitation), ongoing massive hemorrhage requiring significant transfusion, or validated high-risk scores indicating severe bleeding or high re-bleeding risk, be admitted to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive resuscitation, continuous hemodynamic monitoring, urgent diagnostic and therapeutic interventions (often endoscopic), specialized pharmacotherapy, and management of potential complications (Strong recommendation, moderate-quality evidence). Admission to an ICU (or a high-dependency unit with equivalent capabilities) is crucial for such patients due to the need for:
|
33, 79, 80, 81, 82, 83, 84, 85, 86, 87 |
|
We recommend that all patients diagnosed with Acute Liver Failure (ALF) / Fulminant Liver Failure (FLF) – characterized by severe acute liver injury with coagulopathy (INR ≥1.5) and any degree of hepatic encephalopathy (or those without initial encephalopathy but with rapid deterioration of liver function and coagulopathy indicating high risk of imminent ALF/FLF) – be promptly admitted to an Intensive Care Unit (ICU). Ideally, this should be a specialized liver unit or transplant center operating under a high-intensity ICU model, characterized by the intensivist being primarily responsible for or having mandatory daily co-management in the day-to-day care of the patient, ensuring expert critical care input alongside hepatology or/and transplant surgery expertise (Strong recommendation, moderate-quality evidence). Acute Liver Failure is a critical medical emergency characterized by rapid and severe liver injury, impaired liver synthetic function (coagulopathy with INR ≥1.5), and the development of hepatic encephalopathy (any degree of altered mental status) in individuals without pre-existing cirrhosis. The condition is associated with a high risk of life-threatening complications, including:
|
33, 88, 89, 90, 91, 92, 93 |
|
We recommend that all patients diagnosed with severe acute pancreatitis, defined by the presence of persistent organ failure (>48 hours), be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This includes, but is not limited to, aggressive goal-directed fluid therapy, management of respiratory and cardiovascular failure, renal replacement therapy if indicated, specialized nutritional support, advanced pain control, and monitoring and management of local and systemic complications (Strong recommendation, moderate-quality evidence). Severe acute pancreatitis, as defined by the Revised Atlanta Classification and other international guidelines, is characterized by persistent organ failure (lasting >48 hours), which may involve one or multiple organ systems (respiratory, cardiovascular, renal). It is often associated with pancreatic necrosis and a profound systemic inflammatory response syndrome (SIRS), leading to multi-organ dysfunction syndrome (MODS). This life-threatening condition necessitates ICU admission for:
|
33, 94, 95, 96, 97, 98, 99, 100, 101 |
|
We recommend that patients diagnosed with or strongly suspected of having esophageal perforation, with or without initially evident mediastinitis, be promptly admitted to an Intensive Care Unit (ICU). (Strong recommendation, moderate-quality evidence). Esophageal perforation is a highly lethal surgical emergency. The breach in esophageal integrity allows immediate and continued contamination of the mediastinum and/or pleural or peritoneal cavities with oropharyngeal secretions, gastric contents, and bacteria. This leads to:
Given these life-threatening sequelae, patients with esophageal perforation almost invariably require admission to an ICU or a specialized high-acuity surgical unit. This is essential for:
|
33, 102, 103, 104, 105, 106, 107 |
|
We recommend that patients presenting with acute gastroenteritis complicated by severe dehydration leading to hemodynamic instability (e.g., shock, manifested by hypovolemic shock ,persistent hypotension despite initial fluid challenge, significant end-organ hypoperfusion (e.g., oliguria/anuria, altered mental status)), or critical electrolyte or acid-base or acute kidney injury requiring intensive management – be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive and goal-directed fluid resuscitation, continuous hemodynamic and laboratory monitoring, potential vasopressor support, correction of critical electrolyte and acid-base abnormalities, and management of organ dysfunction (Strong recommendation, moderate-quality evidence). gastroenteritis are self-limiting, severe dehydration is a life-threatening complication that can lead to:
Admission to an ICU is typically indicated when severe dehydration leads to these complications, requiring:
|
33, 108, 109, 110 |
|
Endocrine and electrolyte disturbance |
|
|
We recommend that adult patients presenting with severe Diabetic Ketoacidosis (DKA) – characterized by criteria such as arterial pH <7.1, serum bicarbonate <10 mEq/L, significant ketonemia/ketonuria with altered mental status (stupor/coma), or hemodynamic instability – and all patients with Hyperosmolar Hyperglycemic State (HHS) – characterized by marked hyperglycemia (often >600 mg/dL or >33.3 mmol/L), high effective serum osmolality (often >320 mOsm/kg), profound dehydration, and altered mental status – be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities. This admission is essential for aggressive intravenous fluid and electrolyte management, continuous intravenous insulin therapy with frequent and precise monitoring, close observation for neurological and cardiovascular complications, and identification and management of precipitating factors or concurrent organ dysfunction (Strong recommendation, moderate-quality evidence). severe DKA and virtually all cases of HHS are life-threatening metabolic emergencies. Admission to an ICU/HDU is generally indicated for these severe presentations due to:
|
33, 111, 112, 113, 114, 115, 116 |
|
We recommend that all patients diagnosed with or highly suspected of having thyroid storm be promptly admitted to an Intensive Care Unit (ICU) or intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity and potential for rapid deterioration, we suggest their care be managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists (Strong recommendation, moderate-quality evidence). Thyroid storm is a rare but life-threatening exacerbation of hyperthyroidism, characterized by acute and severe multisystem decompensation. It carries a significant mortality rate (10-30%) even with treatment. Admission to an ICU is considered essential due to the need for:
|
33, 117, 118, 119, 120, 121 |
|
We recommend that all patients diagnosed with or highly suspected of having myxedema coma be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity and potential for rapid deterioration, we suggest their care be managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists(Strong recommendation, moderate-quality evidence). Myxedema coma is a rare, life-threatening, extreme manifestation of decompensated hypothyroidism. It is a medical emergency with a high mortality rate (historically 25-60%, though improving with early recognition and aggressive management). Admission to an ICU is considered essential due to the profound multi-system derangements and the need for intensive monitoring and support, including:
|
33, 122, 123, 124, 125, 126, 127 |
|
We recommend that all adult patients presenting with adrenal crisis complicated by hemodynamic instability (e.g., hypotension refractory to initial fluid challenges, signs of shock) be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Given the complexity of managing shock, electrolyte disturbances, and potential multi-organ involvement, we suggest their care managed within ICU model, characterized by the intensivist being responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with endocrinology specialists(Strong recommendation, moderate-quality evidence). Adrenal crisis (acute adrenal insufficiency) is a life-threatening endocrine emergency characterized by an acute deficiency of cortisol, often accompanied by aldosterone deficiency in primary adrenal insufficiency. When complicated by hemodynamic instability (i.e., hypotension progressing to shock, often refractory to initial fluid resuscitation alone), it signifies a state of severe physiological decompensation with high mortality if not recognized and treated promptly and aggressively. ICU admission is essential for such patients due to the need for:
|
33, 128, 129, 130, 131 |
|
We recommend that adult patients presenting with life-threatening hypoglycemia – characterized by severe neuroglycopenia (e.g., coma, seizures, significantly altered mental status requiring external assistance for recovery) or those requiring continuous intravenous glucose infusions with very frequent monitoring to prevent relapse and maintain euglycemia – be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. (Strong recommendation, moderate-quality evidence). Admission to an ICU is typically indicated for such patients due to the need for:
|
33, 132, 133, 134, 135, 136, 137, 138 |
|
Obstetric emergency |
|
|
We recommend that all patients presenting with eclampsia, severe pre-eclampsia with severe features (including but not limited to severe hypertension, evidence of significant end-organ dysfunction), or HELLP syndrome be promptly admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the complexity and potential for rapid deterioration, we suggest their care be managed within a high-intensity ICU/ IMCU model, characterized by experienced multidisciplinary input including obstetricians, anesthesiologists, intensivists, and neonatologists, with clear protocols for escalation and management This includes continuous hemodynamic monitoring, seizure prophylaxis with magnesium sulfate, antihypertensive therapy, and preparation for potential delivery. (Strong recommendation, moderate-quality evidence). These conditions represent the most severe end of the spectrum of hypertensive disorders of pregnancy and are major causes of maternal and perinatal morbidity and mortality. Admission to an ICU/ IMCU is crucial due to the need for:
|
33, 139, 140, 141, 142, 143, 144, 145, 146, 147, 148 |
|
We recommend that all obstetric patients (pregnant or postpartum) who develop significant acute organ dysfunction (e.g., sever postpartum hemaorage, cardiovascular collapse/shock, severe respiratory failure requiring advanced support, acute kidney injury requiring renal replacement therapy, severe coagulopathy, or profound neurological impairment, sever trauma) be promptly admitted to an an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the unique physiological changes of pregnancy and the need for coordinated multidisciplinary care (obstetrics, critical care, anesthesia, neonatology), we suggest their care be managed within a high-intensity ICU/ IMCU model includes continuous hemodynamic monitoring, respiratory support, renal replacement therapy, and other advanced interventions as necessary. (Strong recommendation, moderate-quality evidence). Obstetric patients can develop significant organ dysfunction due to a variety of pregnancy-specific conditions (e.g., obstetric hemorrhage, amniotic fluid embolism, acute fatty liver of pregnancy, peripartum cardiomyopathy) or non-obstetric conditions occurring during or aggravated by pregnancy (e.g., sepsis, pneumonia/ARDS, cardiac disease, trauma). "Significant organ dysfunction" implies failure of one or more vital organ systems (cardiovascular, respiratory, renal, hepatic, neurological, hematological) that threatens the mother's life and often the fetus's well-being. Admission to an ICU/ IMCU is crucial in such cases for:
|
33, 139, 140, 141, 149, 150, 151, 152, 153 |
|
We recommend that pregnant patients with Hyperemesis Gravidarum (HG) who develop severe, life-threatening complications. Such complications include, but are not limited to, profound dehydration leading to hypovolemic shock or severe acute kidney injury (AKI), severe refractory electrolyte imbalances (e.g., critically low potassium or sodium) causing cardiac or neurological symptoms, Wernicke's encephalopathy, or esophageal complications. be admitted to an Intensive Care Unit (ICU) or a intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management with obstetric expertise. Given the unique physiological changes of pregnancy and the need for coordinated multidisciplinary care (obstetrics, critical care, anesthesia, neonatology), we suggest their care be managed within a high-intensity ICU/ IMCU model includes continuous hemodynamic monitoring, respiratory support, renal replacement therapy, and other advanced interventions as necessary. (Strong recommendation, moderate-quality evidence). While most cases of HG are managed on general inpatient wards or as outpatients, a small but critical subset can develop severe, life-threatening complications requiring ICU admission. These complications include:
|
33, 139, 140, 154, 155, 156, 157 |
|
We recommend that adult patients presenting with severe obstetric or gynecologic bleeding, characterized by hemodynamic instability (e.g., shock, persistent hypotension despite initial fluid resuscitation), ongoing massive hemorrhage requiring significant transfusion (e.g., activation of massive transfusion protocol), or evidence of significant end-organ hypoperfusion or coagulopathy, be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate aggressive resuscitation including balanced blood product replacement, continuous hemodynamic monitoring, urgent interventions for source control (medical, radiological, or surgical), specialized pharmacotherapy (e.g., tranexamic acid, uterotonics), and management of potential complications such as coagulopathy, ARDS, or AKI (Strong recommendation, moderate-quality evidence). every obstetric bleeding (e.g., postpartum hemorrhage (PPH), placental abruption, ruptured ectopic pregnancy, placenta accreta spectrum) and severe acute gynecologic bleeding (e.g., from ruptured ovarian cysts, advanced gynecologic cancers, severe abnormal uterine bleeding, postoperative hemorrhage) are major causes of maternal/female morbidity and mortality. "Severe" bleeding implies hemodynamic instability (hypovolemic shock), the need for massive transfusion, or evidence of end-organ hypoperfusion and coagulopathy. Admission to an ICU or a unit with intermediate care capabilities is crucial for such patients due to the need for:
|
33, 139, 140, 141, 149, 158, 159, 160, 161, 162, 163, 164 |
|
Trauma and injures |
|
|
We recommend that all adult patients presenting with severe traumatic brain injury or post concussion manifestations, defined by a Glasgow Coma Scale (GCS) score of ≤ 8 after initial resuscitation, be promptly admitted to an Intensive Care Unit (ICU) capable of providing comprehensive neurocritical care. This includes airway protection, mechanical ventilation, intracranial pressure monitoring, hemodynamic support, and multidisciplinary care. Given the complexity of managing severe TBI and the potential for rapid neurological deterioration, we suggest their care be managed within a high-intensity neuro-ICU model, characterized by the intensivist (often a neurointensivist or an intensivist with neurocritical care expertise) being primarily responsible for or having a mandatory and active role in the day-to-day co-management of the patient, in close collaboration with neurosurgery and other relevant specialists (Strong recommendation for ICU admission, moderate-quality evidence Conditional recommendation for specific ICU model,low quality evidence) Patients with severe TBI (GCS ≤ 8) are at high risk of mortality and severe long-term disability. ICU admission is critical for:
|
33, 165, 166, 167, 168, 169 |
|
We recommend that adult patients with an acute spinal cord injury resulting in significant neurological deficit (e.g., quadriplegia, paraplegia) that causes or poses an imminent risk of respiratory failure (typically injuries at or above the C5 level) or hemodynamic instability (neurogenic shock, typically from injuries at or above the T6 level) be promptly admitted to preferably a specialized Neuro-ICU or Intensive Care Unit (ICU), preferably one with expertise in neurocritical care and trauma. This is to facilitate advanced airway and respiratory support (including mechanical ventilation), intensive hemodynamic monitoring and management to maintain spinal cord perfusion, prevention and treatment of systemic complications, and expert multidisciplinary care in conjunction with neurosurgery and spine surgery teams (Strong recommendation, moderate-quality evidence). acute SCI, particularly injuries affecting the cervical or high thoracic spinal cord, often leads to life-threatening physiological derangements that necessitate admission to an ICU. The primary drivers for ICU admission are:
|
33, 165, 170, 171, 172, 173, 174, 175 |
|
We recommend that adult patients presenting with significant solid organ injury, classified as American Association for the Surgery of Trauma (AAST) Grade III or higher (either single or multiple organs), be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for intensive monitoring and management. This is to facilitate continuous hemodynamic and hematological assessment, early detection of bleeding or failure of non-operative management, readiness for urgent angiographic or surgical intervention, aggressive pain control, and management of associated injuries or systemic complications. For patients who are hemodynamically unstable or have evidence of ongoing bleeding despite initial resuscitation, direct ICU admission is strongly recommended (Strong recommendation, moderate-quality evidence). Patients sustaining solid organ injuries (e.g., to the liver, spleen, kidneys, pancreas, urogenital ) classified as American Association for the Surgery of Trauma (AAST) Grade III or higher are at substantial risk for serious complications, even if initially hemodynamically stable and selected for non-operative management (NOM). Admission to an ICU or a closely monitored environment like an IMCU is often crucial for:
|
33, 165, 176, 178, 179, 180, 181, 182, 183 |
|
We recommend that all adult patients presenting with polytrauma who have a high probability of needing major intervention (e.g., surgery, angiography) and/or require intensive physiological monitoring and support due to actual or impending organ dysfunction or hemodynamic instability be promptly admitted to an Intensive Care Unit (ICU), preferably one within a designated trauma center with readily available multidisciplinary trauma expertise. (Strong recommendation, moderate-quality evidence). Admission to an ICU is crucial for such patients due to the need for: Management of Hemorrhagic Shock and Trauma-Induced Coagulopathy (TIC): Aggressive resuscitation with blood products according to massive transfusion protocols (MTPs), control of ongoing hemorrhage (surgical, angiographic), and specific management of TIC. Airway Management and Advanced Respiratory Support: Many polytrauma patients require endotracheal intubation and mechanical ventilation due to traumatic brain injury (TBI with GCS ≤ 8), thoracic trauma (e.g., flail chest, pulmonary contusions, hemopneumothorax), altered mental status from shock, or for operative procedures. ARDS is a common complication requiring specialized ventilator strategies. Intensive Neurological Monitoring and Management: For patients with associated TBI, including monitoring for and management of intracranial hypertension (ICHtn) and optimization of cerebral perfusion pressure (CPP). Support for Multiple Organ Dysfunction Syndrome (MODS): Polytrauma frequently leads to SIRS and MODS, affecting cardiovascular, respiratory, renal, hepatic, and coagulation systems, requiring integrated organ support. Continuous Hemodynamic Monitoring: Often invasive (arterial line, central venous catheter, advanced cardiac output monitoring) to guide resuscitation and vasoactive drug therapy. Post-Operative Critical Care: Following damage control surgery or other major operative interventions. Pain Management: Complex pain management strategies are often required for multiple injuries. Monitoring for Missed Injuries and Complications: Such as compartment syndromes, sepsis, venous thromboembolism (VTE), fat embolism syndrome. Coordination of Multidisciplinary Care: Involving trauma surgeons, intensivists, orthopedic surgeons, neurosurgeons, anesthesiologists, interventional radiologists, and other specialists. |
33, 165, 176, 178, 179, 180, 184, 185, 186, 187 |
|
We recommend that decisions regarding ICU admission for adult burn patients should carefully consider factors such as the type of burn, percentage of Total Body Surface Area (%TBSA) affected, presence of inhalation injury, location of burns, associated trauma, patient age, pre-existing comorbidities, and the number of victims in large-scale mass casualty incidents. Specifically, under normal circumstances, we advise that adult patients presenting with severe second- or third-degree burns—including partial-thickness burns exceeding 15–20% TBSA, full-thickness burns exceeding 5–10% TBSA, require mechanical ventilation (eg, significant inhalation injuries, massive fluid resuscitation), electrical or major chemical burns, burns involving critical areas (face, hands, feet, genitalia, perineum, or major joints), or burns in individuals with significant pre-existing medical conditions or accompanying traumatic injuries—be ideally admitted to a dedicated Burn Intensive Care Unit (ICU) within a specialized Burn Center. Given the complex and highly specialized nature of burn care, we strongly suggest that these patients be managed by an experienced multidisciplinary burn team, comprising intensivists, burn surgeons, specialized nurses, respiratory therapists, and nutritionists within an ICU setting. (Strong recommendation, moderate-quality evidence). Not all 2nd or 3rd-degree burns necessitate ICU admission. The decision is critically dependent on Burn Center care for severe injuries inherently involves ICU-level management for the acute phase. Criteria typically include:
Severe burns are profound injuries leading to complex pathophysiological changes that require intensive, multidisciplinary care. ICU admission is crucial for:
|
33, 188, 189, 190, 191, 192, 193, 194 |
|
We recommend that adult patients presenting with severe burns defined by criteria be admitted to an Intensive Care Unit (ICU). While admission to a specialized Burn ICU within a designated Burn Center is the optimal standard of care, a general ICU can and should provide the necessary life-saving critical care for these patients when a specialized Burn ICU is not immediately available or in/During mass casualty scenarios.( Good practice statement, low-quality evidence). |
33, 191, 192, 193, 194 |
|
We recommend that adult patients presenting with life-threatening crush injuries – characterized by extensive muscle damage, prolonged compression, evidence of or high risk for Crush Syndrome (e.g., significant rhabdomyolysis, hyperkalemia, early AKI), severe compartment syndrome, or associated hemodynamic instability – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate aggressive resuscitation including Correction of Metabolic Acidosis and Other Electrolyte Disturbances, balanced blood product replacement, continuous hemodynamic monitoring, urgent interventions for source control (medical, or surgical), Monitoring and Management of Compartment Syndrome , specialized pharmacotherapy (e.g., tranexamic acid, uterotonics), and management of potential complications such as coagulopathy, ARDS, or AKI (Strong recommendation, moderate-quality evidence). Life-threatening crush injuries, particularly those leading to or at high risk of Crush Syndrome or severe Compartment Syndrome, are medical emergencies with significant morbidity and mortality. Crush Syndrome is a systemic manifestation of muscle cell damage resulting from prolonged pressure, leading to rhabdomyolysis (release of myoglobin, potassium, phosphate, uric acid), which can cause:
Compartment syndrome, if not promptly treated by fasciotomy, leads to irreversible muscle and nerve damage and can contribute to systemic complications. ICU admission is crucial for such patients due to the need for:
|
33, 188, 189, 190, 191, 192, 193, 194, 195, 196, 197, 198, 199 |
|
We recommend that all patients presenting with life-threatening gunshot wounds or blast injuries, characterized by hemodynamic instability, significant hemorrhage requiring or likely to require massive transfusion, compromised airway or breathing, severe traumatic brain injury (GCS ≤ 8), or evidence of significant penetrating or multi-system trauma, be promptly admitted to an Intensive Care Unit (ICU), ideally within a designated trauma center equipped for comprehensive trauma and critical care. Given the complexity and need for coordinated, multidisciplinary expert care (trauma surgery, critical care, neurosurgery, orthopedic surgery, anesthesia, interventional radiology), we suggest their care be managed within a ICU model, characterized by the intensivist and trauma surgeon having a primary or mandatory and active co-management role (Strong recommendation, moderate-quality evidence). life-threatening gunshot wounds and blast injuries represent severe forms of trauma, often resulting in polytrauma with complex injury patterns and a high risk of mortality and significant morbidity. ICU admission is critical for these patients due to:
|
33, 165, 176, 178, 179, 181, 182, 183, 184, 186, 200, 201 |
|
Pulmonary System |
|
|
We recommend
that adult patients presenting with acute respiratory failure, defined by
severe hypoxemia (PaO2/FiO2 ratio < 100), hypercapnia (PaCO2 > 50 mmHg
with pH < 7.35), or the need for non-invasive or invasive mechanical
ventilation, be promptly admitted to an Intensive Care Unit (ICU) or an intermediate
care unit (IMCU) with equivalent capabilities. This is to facilitate advanced
respiratory support (including mechanical ventilation and lung-protective
strategies when indicated), continuous respiratory and hemodynamic
monitoring, management of the underlying cause of respiratory failure, and
treatment of potential complications (Strong recommendation, high-quality
evidence). ICU admission is crucial for patients with ARF due to:
|
33, 225, 226, 227, 228, 229, 230, 231, 232, 233, 234, 235 |
|
We recommend that adult patients presenting with acute pulmonary embolism be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities if they are classified as high-risk (i.e., presenting with hemodynamic instability/shock) or intermediate-high risk (i.e., hemodynamically stable but with evidence of both right ventricular dysfunction and myocardial injury). This is to facilitate immediate hemodynamic and respiratory support, administration and monitoring of reperfusion therapies (e.g., thrombolysis), close observation for clinical deterioration allowing for timely rescue interventions, and management of potential complications (Strong recommendation, moderate-quality evidence). Not all patients with acute PE require ICU admission. The decision is critically dependent on risk stratification, which primarily assesses the short-term risk of death or hemodynamic decompensation. This is based on hemodynamic stability, markers of right ventricular (RV) dysfunction, and myocardial injury. Admission to an ICU/IMCU is crucial for:
|
33, 236, 237, 238, 239 |
|
We recommend that patients presenting with life-threatening hemoptysis – characterized by airway compromise, hemodynamic instability, significant respiratory failure, or bleeding volume/rate considered to be high risk – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities. This is to facilitate immediate airway management, resuscitation, continuous cardiorespiratory monitoring, and urgent diagnostic and therapeutic interventions, most notably bronchoscopy and bronchial artery embolization (BAE), in a coordinated, multidisciplinary fashion involving intensivists, pulmonologists, interventional radiologists, and thoracic surgeons (Strong recommendation, moderate-quality evidence). Life-threatening hemoptysis (often also termed "massive hemoptysis") is a medical emergency with high mortality. While definitions vary regarding the volume of expectorated blood (e.g., >100-600 mL/24h), a more clinically relevant definition focuses on any amount of bleeding that causes physiological compromise. The primary cause of death is asphyxiation from blood filling the airways, rather than exsanguination from blood loss. Admission to an ICU is crucial for patients with life-threatening hemoptysis due to the need for:
|
33, 240, 241, 242, 243, 244, 245 |
|
We recommend that all patients who have been treated for a tension pneumothorax be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This admission is essential for ongoing hemodynamic resuscitation and support, management of respiratory failure (often with mechanical ventilation), monitoring and management of the chest drain and any persistent air leak, observation for complications such as re-expansion pulmonary edema, and diagnosis and treatment of the underlying precipitating cause (Strong recommendation, moderate-quality evidence). A tension pneumothorax is an immediate, life-threatening emergency where air progressively accumulates in the pleural space, causing complete lung collapse, mediastinal shift, and compression of the great vessels. This leads to acute respiratory failure and obstructive shock, which can rapidly progress to cardiac arrest. While the immediate life-saving intervention is rapid decompression (via needle thoracostomy followed by definitive tube thoracostomy/chest drain), subsequent admission to an ICU or Intermediate Care Unit (IMCU) is crucial. The initial event is a sign of severe underlying injury or pathology, and these patients remain critically ill. ICU admission is necessary for:
|
33, 246, 247, 248, 249, 250, 251 |
|
We recommend that adult patients presenting with a massive pleural effusion that causes acute respiratory failure (characterized by severe dyspnea, increased work of breathing, or hypoxemia) or hemodynamic compromise be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to treating underlying cause pleural effusion also facilitate treating urgent, controlled therapeutic drainage, provide advanced respiratory and hemodynamic support as needed, allow for intensive monitoring for and management of potential complications (especially re-expansion pulmonary edema), and to diagnose and manage the severe underlying cause of the effusion (Strong recommendation, moderate-quality evidence). A massive pleural effusion is typically defined radiologically as opacification of most or all of a hemithorax, often with contralateral mediastinal shift. While the underlying cause can vary (e.g., malignancy, infection/empyema, heart failure, trauma/hemothorax, liver cirrhosis), the need for ICU admission is not determined by the effusion itself, but by its acute physiological consequences or the severity of the underlying illness. ICU or Intermediate Care Unit (IMCU) admission is crucial for patients with a massive pleural effusion who present with:
|
33, 253, 254, 255, 256, 257, 258, 259, 260, 261, 262 |
|
We recommend that adult patients presenting with a severe or life-threatening exacerbation of asthma or COPD be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Indications for this level of care include acute respiratory failure requiring non-invasive or invasive mechanical ventilation, severe dyspnea with signs of respiratory muscle fatigue, altered mental status, persistent or worsening hypoxemia, or severe/worsening respiratory acidosis despite initial therapy. This is to facilitate advanced respiratory support, continuous cardiorespiratory monitoring, intensive pharmacotherapy, and management of potential complications (Strong recommendation, moderate-to-high quality evidence). While most exacerbations of asthma and COPD are managed in outpatient or general ward settings, severe exacerbations can lead to life-threatening acute respiratory failure. Admission to an ICU or an intermediate (IMCU) is crucial for patients with signs of severe distress or impending respiratory arrest. For Severe Asthma Exacerbation (Status Asthmaticus), ICU admission is indicated for:
For Severe COPD Exacerbation, ICU admission is indicated for:
|
33, 263, 264, 265, 265, 266, 267, 268, 269, 270 |
|
We recommend that adult patients presenting with undifferentiated dyspnea accompanied by warning signs of physiological instability – characterized by severe respiratory distress (e.g., high respiratory rate, accessory muscle use, inability to speak), hypoxemia (e.g., SpO2 <90% on significant oxygen support), hemodynamic compromise (e.g., shock, hypotension), or altered mental status – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate cardiorespiratory stabilization and life support (including non-invasive or invasive mechanical ventilation), continuous intensive monitoring, and a rapid, concurrent diagnostic evaluation to identify and treat the underlying cause (Strong recommendation, moderate-quality evidence). "Undifferentiated dyspnea" refers to severe shortness of breath where the underlying cause is not immediately clear. When accompanied by "warning vital signs" or other objective signs of severe distress, it represents a state of active or impending cardiorespiratory collapse and is a medical emergency. The need for ICU admission is not driven by the specific diagnosis (which is unknown) but by the severity of the physiological derangement, which requires immediate stabilization, intensive monitoring, and rapid diagnostic evaluation. Warning Vital Signs and Clinical Features Indicating Need for ICU: These include, but are not limited to:
ICU admission is crucial for:
|
33, 271, 272, 273 |
|
Neurologic Disorders |
|
|
We recommend that all patients presenting in a coma (defined as a Glasgow Coma Scale [GCS] score of ≤ 8) of a known or suspected metabolic, toxic, or anoxic etiology be promptly admitted to an Intensive Care Unit (ICU). This is to facilitate immediate airway management (endotracheal intubation and mechanical ventilation), continuous cardiorespiratory and neurological monitoring, rapid diagnostic evaluation to determine the specific cause, and administration of specific treatments (e.g., targeted temperature management, metabolic correction, antidotes, enhanced elimination techniques) and comprehensive organ support. Given the complexity and need for multidisciplinary expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with relevant specialists (e.g., neurology, toxicology, endocrinology) (Strong recommendation, moderate-quality evidence). Coma, a state of unarousable unresponsiveness, is a medical emergency regardless of its cause. The primary and most immediate life-threat for any comatose patient is the loss of airway protective reflexes, leading to a high risk of airway obstruction, aspiration of gastric contents, and respiratory arrest. Therefore, admission to an ICU is essential for all patients in a coma to provide:
|
33, 274, 275, 276, 277, 278, 279, 285 |
|
We recommend that adult patients presenting with acute neurological deficits accompanied by an impaired level of consciousness (Glasgow Coma Scale score <15, and especially ≤ 8) be promptly admitted to an Intensive Care Unit (ICU) or a Comprehensive Stroke/neuro Unit with equivalent ICU capabilities. This is to facilitate immediate airway management if necessary, intensive neurological and hemodynamic monitoring, management of intracranial pressure and cerebral edema, and post-procedure care, and management of systemic complications (Strong recommendation, low-quality evidence). |
33, 280, 281, 282, 283, 284, 285 |
|
We recommend that adult patients presenting with a severe acute cerebral vascular stroke (ischemic or hemorrhagic:- ( intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH))be promptly admitted to an Intensive Care Unit (ICU), preferably a specialized Neuro-ICU, or a Comprehensive Stroke Unit with equivalent ICU capabilities. Indications for this level of care include, but are not limited to, an impaired level of consciousness (Glasgow Coma Scale [GCS] score ≤ 8), signs of intracranial hypertension or impending herniation, the need for mechanical ventilation, hemodynamic instability, ongoing management of therapies such as intravenous thrombolysis or post-mechanical thrombectomy care, or management of severe complications such as large or expanding hematomas, intraventricular hemorrhage, or aneurysmal subarachnoid hemorrhage (Strong recommendation, moderate-quality evidence). While not all stroke patients require ICU admission (many are managed in dedicated Stroke Units), those with severe strokes or life-threatening complications need the level of monitoring and intervention that only an ICU can provide. The specific indications vary slightly between ischemic and hemorrhagic stroke, but the overarching need is driven by actual or potential neurological and systemic decompensation. ICU admission is crucial for:
|
33, 280, 281, 282, 285, 286, 287, 288, 289 , 290, 291 |
|
We recommend that adult patients presenting with an acute focal neurological deficit who also exhibit signs of critical illness – characterized by an impaired level of consciousness (Glasgow Coma Scale score ≤ 13), acute respiratory failure requiring advanced support, hemodynamic instability, signs of increased intracranial pressure or impending herniation, or status epilepticus – be promptly admitted to an Intensive Care Unit (ICU), preferably a specialized Neuro-ICU or a Comprehensive Stroke Unit with equivalent ICU capabilities. This is to facilitate immediate airway management, continuous neurological and hemodynamic monitoring, aggressive management of intracranial pressure and other neurological complications, and rapid investigation and treatment of the underlying life-threatening cause (Strong recommendation, moderate-quality evidence). ICU admission is not indicated for the focal deficit itself, but for the severity of the underlying cause or for associated life-threatening complications. Therefore, this response focuses on patients presenting with an AFND who also have signs of critical illness requiring ICU-level care. Patients with an AFND require ICU admission when the underlying condition leads to or poses an immediate risk of:
|
33, 280, 281, 282, 285, 288, 289, 290, 292, 293, 294 |
|
We recommend that adult patients with Myasthenic Crisis (defined by respiratory failure secondary to myasthenia gravis) and those with severe Guillain-Barré Syndrome (GBS) – characterized by rapid progression of weakness, evidence of respiratory muscle compromise (e.g., vital capacity <20 mL/kg), significant bulbar dysfunction, or severe autonomic instability – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate intensive cardiorespiratory monitoring, timely non-invasive or invasive mechanical ventilation, management of autonomic dysfunction, administration of specific immunotherapies, and comprehensive supportive care. Given the need for specialized neurological and critical care expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with neurology specialists(Strong recommendation, moderate-quality evidence). Both Myasthenic Crisis and severe Guillain-Barré Syndrome are acute neuromuscular emergencies where the primary life-threat is acute respiratory failure due to weakness of the respiratory muscles (diaphragm and intercostal muscles). ICU admission is crucial for:
|
33, 295, 296, 297, 298, 299, 300, 301, 302, 303, 304, 305 |
|
We recommend that adult patients presenting with neurological infections such as:- meningitis, who also exhibit signs of severe neurological compromise (e.g., altered mental status with a Glasgow Coma Scale [GCS] score ≤ 11, and particularly ≤ 8) or significant systemic organ dysfunction (e.g., respiratory compromise requiring advanced airway or ventilatory support, or hemodynamic instability/septic shock) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This is to facilitate immediate airway management, intensive neurological and hemodynamic monitoring (including management of intracranial pressure), rapid administration of appropriate antimicrobial and adjunctive therapies, and comprehensive management of seizures, shock, and multi-organ failure (Strong recommendation, high-quality evidence).
Meningitis, particularly acute bacterial meningitis, can be a rapidly progressive and life-threatening infection. While uncomplicated cases may be managed on a general ward, admission to an ICU is crucial when patients develop severe complications. The primary drivers for ICU admission are:
|
33, 285, 292, 306, 307, 308, 309, 310, 311, 312, 313, 314, 315, 316, 317 |
|
We recommend that all adult patients with established convulsive status epilepticus (defined as continuous seizure activity >5 minutes or ≥2 discrete seizures without recovery of consciousness between them) or uncontrolled convulsions be promptly admitted to an Intensive Care Unit (ICU) or specialized Neuro-ICU or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management . This admission is essential to facilitate aggressive, stepwise anticonvulsant therapy (including potential administration of continuous anesthetic infusions for refractory cases), secure and manage the airway (often with mechanical ventilation), provide continuous electroencephalography (cEEG) and hemodynamic monitoring, and manage life-threatening systemic complications. Given the need for specialized neurological and critical care expertise, we suggest their care be managed within a ICU model, characterized by the intensivist having a primary or mandatory and active co-management role with neurology/epileptology specialists (Strong recommendation, high-quality evidence). Status Epilepticus (SE) is a neurological emergency defined as a continuous seizure lasting longer than 5 minutes, or two or more seizures without a full recovery of consciousness in between. "Uncontrolled convulsions" are functionally equivalent to convulsive status epilepticus. SE is associated with significant morbidity (including permanent neuronal injury) and mortality. ICU admission is critical for patients with established or refractory SE due to the need for:
|
33, 285, 318, 319, 320, 321, 322, 323, 324, 325, 326, 327, 328, 329 |
|
Surgical and postoperative |
|
|
We recommend that adult surgical patients be admitted to an Intensive Care Unit (ICU) or any specialized ICU or with equivalent capabilities for comprehensive critical care management if they meet one or more of the following criteria: (1) they have undergone a high-risk surgical procedure known to require intensive monitoring and support post-operatively (e.g., major cardiac, thoracic, aortic, neurological, vascular, abdominal, or transplant surgery); (2) they have severe pre-existing comorbidities that significantly impair their physiological reserve to withstand major surgery; or (3) they exhibit evidence of acute organ dysfunction or hemodynamic instability in the immediate postoperative period (e.g., need for mechanical ventilation, vasopressor support, or ongoing massive transfusion). This is to facilitate advanced organ support, continuous cardiorespiratory and neurological monitoring, management of major fluid shifts and bleeding, advanced pain control, and early detection and management of life-threatening postoperative complications (Strong recommendation, high-quality evidence). Admission to an ICU is not required for all surgical patients. It is reserved for a high-risk population whose physiological reserve is, or is expected to be, overwhelmed by the combined stress of their underlying disease, comorbidities, and the surgical procedure itself. The decision is based on a combination of pre-operative patient factors, the nature of the surgery, and the patient's immediate postoperative physiological state. ICU admission is crucial for:
|
1, 33, 168, 330, 331, 332, 333, 334, 335, 336, 353 |
|
We suggest that surgical patients who are hemodynamically stable at the conclusion of surgery, successfully extubated, and require only enhanced monitoring (e.g., continuous electrocardiography, invasive arterial pressure monitoring) or low-level therapeutic support (e.g., non-invasive ventilation, single low-dose vasopressor) may be admitted to a designated Intermediate Care Unit (IMCU) with appropriate nurse-to-patient ratios and protocols for rapid escalation of care if needed. This strategy can optimize critical care resource allocation without compromising patient safety. (Good practice statement, moderate -quality evidence). |
12, 13, 14, 15, 33, 330, 390 |
|
Renal disorders |
|
|
We recommend that adult patients with acute kidney injury (AKI) who require urgent renal replacement therapy be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate the safe initiation and management of renal replacement therapy (including continuous modalities like Continuous Renal Replacement Therapy for hemodynamically unstable patients), provide continuous monitoring for and treatment of life-threatening electrolyte and acid-base disturbances, and deliver comprehensive organ support for the underlying critical illness that precipitated the AKI such as:(CKD, sepsis, shock, tumor lysis syndrome or rhabdomyolysis etc.) (Strong recommendation, moderate-to-high quality evidence). AKI signifies that the kidney failure has led to life-threatening metabolic or fluid balance derangements that are refractory to medical management. The indications for urgent urgent renal replacement therapy are themselves critical conditions requiring an ICU level of care. Furthermore, the initiation of renal replacement therapy, especially intermittent hemodialysis, in a physiologically unstable patient can cause hemodynamic compromise and requires intensive monitoring. ICU admission is crucial for:
|
33, 237, 238, 239, 240, 241, 242, 243, 344, 349 |
|
We recommend that adult patients presenting with a severe acid-base disorder – characterized by extreme derangement in arterial pH (e.g., acidemia with pH < 7.20 or alkalemia with pH > 7.55) or a less extreme derangement accompanied by evidence of significant organ dysfunction (e.g., shock, altered mental status, respiratory failure) – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate continuous cardiorespiratory and neurological monitoring, aggressive management of the underlying cause, advanced respiratory and hemodynamic support as needed, and frequent biochemical monitoring to guide therapy (Strong recommendation, moderate-quality evidence). A severe acid-base disorder is a life-threatening condition where the blood pH moves to extreme levels, causing profound dysfunction of multiple organ systems. It is not a standalone diagnosis but rather a manifestation of a critical underlying illness (e.g., shock, sepsis, respiratory failure, renal failure, diabetic ketoacidosis, poisoning). The need for ICU admission is driven by the direct physiological consequences of the pH derangement and the intensity of care required to manage both the acid-base disorder and its underlying cause. ICU admission is crucial for managing:
|
33, 337, 344, 345, 346, 347, 348, 349, 350, 351 |
|
We recommend that adult patients presenting with severe hyperkalemia (e.g., serum K+ > 6.0-6.5 mmol/L) that is accompanied by any new ECG changes attributable to hyperkalemia, or that is refractory to initial medical therapies, be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU)/High-Dependency Unit (HDU) with continuous cardiac monitoring capabilities. This is to facilitate immediate and ongoing cardiac monitoring, administration of emergency medical therapies, urgent initiation of renal replacement therapy (dialysis) for definitive potassium removal, frequent laboratory monitoring, and management of the underlying cause (Strong recommendation, moderate-quality evidence). Severe hyperkalemia (generally defined as serum potassium [K+] > 6.0-6.5 mmol/L) is life-threatening primarily due to its effects on cardiac myocyte membrane potential, leading to lethal cardiac arrhythmias. The presence of ECG changes (from peaked T waves to QRS widening, sine wave pattern, and ultimately ventricular fibrillation or asystole) signifies significant cardiotoxicity. When this condition is refractory to initial medical therapies (e.g., calcium for membrane stabilization, insulin/dextrose and beta-agonists to shift potassium intracellularly), the patient is at immediate risk of cardiac arrest. ICU admission is crucial for:
|
33, 337, 350, 351, 352, 353, 354, 355, 356 |
|
We recommend that adult patients presenting with significant volume overload causing acute pulmonary edema and respiratory distress (characterized by severe dyspnea, increased work of breathing, and/or hypoxemia) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate advanced respiratory support (most notably non-invasive ventilation), aggressive and monitored fluid removal with intravenous diuretics or renal replacement therapy, administration of vasoactive medications as needed, and continuous cardiorespiratory monitoring (Strong recommendation, low-quality evidence). Significant volume overload becomes life-threatening when it leads to acute pulmonary edema (the accumulation of fluid in the lung's interstitial and alveolar spaces), causing severe gas exchange abnormalities and acute hypoxemic respiratory failure. This is a medical emergency regardless of the underlying cause (e.g., acute decompensated heart failure [ADHF], acute kidney injury [AKI] with anuria, iatrogenic fluid overload). Admission to an ICU or Intermediate Care Unit (IMCU) is crucial for:
|
33, 337, 357, 358 |
|
We recommend that adult patients with uremic pericarditis who present with cardiac tamponade or evidence of significant hemodynamic compromise (e.g., hypotension, shock) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate urgent pericardiocentesis or surgical drainage, safe initiation and management of intensive renal replacement therapy (dialysis) in an unstable patient, continuous cardiorespiratory and hemodynamic monitoring, and comprehensive management of the underlying severe renal failure (Strong recommendation, moderate-quality evidence). Uremic pericarditis is inflammation of the pericardium in patients with severe acute or end-stage kidney disease. While uncomplicated uremic pericarditis can sometimes be managed on a specialized nephrology ward with intensive dialysis, admission to an ICU becomes necessary when life-threatening complications arise. ICU care is crucial for:
|
33, 337, 359, 360, 361, 362 |
|
We recommend that adult patients diagnosed with Hepatorenal Syndrome-Acute Kidney Injury (HRS-AKI) be promptly admitted to an Intensive Care Unit (ICU), preferably one with expertise in hepatology and liver transplantation. This is to facilitate the administration and intensive monitoring of vasoconstrictor and albumin therapy, aggressive management of hemodynamic instability and other complications of decompensated cirrhosis (e.g., hepatic encephalopathy, bleeding), delivery of renal replacement therapy if indicated, and comprehensive multi-organ support as a bridge to potential liver transplantation (Strong recommendation, moderate-quality evidence). |
337, 363, 364, 365, 366, 367, 368, 369 |
|
Drug Ingestion, Drug Overdose, & sever Drug reaction |
|
|
We recommend that patients presenting with a known or suspected drug ingestion who exhibit signs of life-threatening toxicity – characterized by altered mental status with inadequate airway protection (e.g., Glasgow Coma Scale score ≤ 8), hemodynamic instability (e.g., shock, life-threatening arrhythmias, severe hypertension), respiratory failure requiring advanced support, ongoing seizures, or severe metabolic/laboratory abnormalities – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate immediate life support (airway, breathing, circulation), continuous cardiorespiratory and neurological monitoring, administration of antidotes, consideration of enhanced elimination techniques (e.g., hemodialysis), and management of multi-organ complications (Strong recommendation, moderate-quality evidence). The primary principle of managing severe poisoning is aggressive supportive care, alongside specific antidotes and enhanced elimination techniques where indicated. ICU admission is crucial for:
|
33, 353, 370, 371, 372, 373, 374, 375, 376, |
|
Miscellaneous |
|
|
We recommend that all adult patients presenting with septic shock (defined by persisting hypotension requiring vasopressors to maintain MAP ≥65 mmHg and serum lactate >2 mmol/L despite adequate volume resuscitation) and patients with sepsis accompanied by significant hemodynamic instability (e.g., hypotension responsive only to ongoing aggressive fluid resuscitation, or other signs of organ hypoperfusion such as persistently elevated lactate despite initial fluids) be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This admission is essential to facilitate timely implementation of sepsis management bundles, including rapid administration of appropriate antimicrobials, aggressive hemodynamic resuscitation with fluids and vasoactive agents, source control measures, potential advanced respiratory support, and continuous monitoring and management of organ dysfunction (Strong recommendation, moderate-quality evidence). ICU admission is crucial for these patients due to the need for:
|
1, 33, 104, 202, 203, 204, 205, 353 |
|
We recommend that adult patients presenting with life-threatening environmental injuries – specifically heat stroke (core temperature >40°C with CNS dysfunction), severe complications of drowning (e.g., significant hypoxemia, ARDS, altered mental status), severe hypothermia (core temperature <32°C with cardiovascular instability or coma), severe environmentally-induced hyperthermia with organ dysfunction, severe altitude illness (High Altitude Cerebral Edema [HACE] or High Altitude Pulmonary Edema [HAPE] with respiratory failure or coma), severe barotrauma (especially pulmonary barotrauma with Arterial Gas Embolism [AGE]), or severe Decompression Sickness (Type II DCS with neurological or cardiorespiratory compromise) – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. This is to facilitate aggressive specific therapies (e.g., rapid cooling/rewarming, hyperbaric oxygen coordination, specific pharmacotherapies), advanced respiratory and hemodynamic support, continuous multi-organ monitoring, and management of potential complications we suggest their care be managed within ICU model, characterized by the intensivist having a primary or mandatory and active co-management role in conjunction with relevant specialists (Strong recommendation, moderate-quality evidence). patients with life-threatening Environmental Injuries – specifically Heat Stroke, severe complications of Drowning, severe Hypo/Hyperthermia, severe Altitude Illness (HACE/HAPE), severe Barotrauma (especially with Arterial Gas Embolism), and severe Decompression Sickness These conditions, when severe, are medical emergencies associated with high risk of multi-organ dysfunction and mortality. ICU admission is crucial for intensive monitoring, aggressive supportive care, and specific interventions.
|
33, 206, 207, 208, 209, 210, 211, 212, 213, 214, 215, 353 |
|
We recommend that adult patients presenting with signs of severe systemic envenomation from a snakebite or scorpion sting be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management.. Signs of severe envenomation requiring such admission include, but are not limited to: respiratory failure or compromise (e.g., neurotoxic paralysis, pulmonary edema), hemodynamic instability (e.g., shock, severe hypertension), venom-induced consumptive coagulopathy with active bleeding, significant neurological impairment (e.g., altered mental status, seizures), or evidence of severe end-organ damage such as acute kidney injury or severe rhabdomyolysis. This is to facilitate timely administration and monitoring of antivenom (including management of adverse reactions), advanced respiratory and hemodynamic support, management of coagulopathy, and comprehensive multi-organ supportive care (Strong recommendation, moderate-quality evidence). While many snakebites and scorpion stings cause only local effects, a significant number, depending on the species and venom dose, can cause severe, life-threatening systemic toxicity requiring ICU admission. The specific indications vary between snake and scorpion envenomation due to different venom pathophysiologies. For Snake Envenomation, ICU admission is crucial for managing:
For Scorpion Envenomation, ICU admission is crucial for managing:
|
33, 216, 217, 218, 219, 220, 221, 222, 223, 224, 353 |
|
Parameter criteria |
|
|
Vital Signs |
|
|
We recommend that adult patients presenting with warning vital signs indicating acute or impending critical illness be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such warning signs include, but are not limited to, evidence of a compromised airway; severe respiratory distress (e.g., respiratory rate >30 or <10 breaths/min, SpO2 <90% on significant oxygen support); hemodynamic instability (e.g., HR <40 or >130, shock with Systolic arterial pressure ≤ 90 mm Hg or ≥ 160 mmHg or requiring vasopressors) (Mean arterial pressure ≤ 60 mm Hg or Diastolic arterial pressure > 110 mmHg ). ; life-threatening arrhythmias; or a new, significant alteration in level of consciousness (e.g., GCS drop, new-onset coma). This is to facilitate continuous cardiorespiratory and neurological monitoring, immediate life support, and a rapid, concurrent diagnostic evaluation to identify and treat the underlying cause (Strong recommendation, moderate-quality evidence). ICU admission is often triggered not by a specific diagnosis, but by the degree of physiological derangement, which is directly measured by vital signs. "Warning vital signs" are objective indicators of actual or impending organ failure and a high risk of deterioration or cardiac arrest. The key vital signs and their "warning" thresholds that often necessitate ICU/IMCU admission include:
ICU admission is crucial for these patients for continuous cardiorespiratory monitoring, immediate life support (e.g., mechanical ventilation, vasopressors), and rapid diagnostic investigation to identify and treat the underlying cause. |
16, 32, 33, 35, 417 |
|
We recommend that adult patients with a persistent core body temperature of < 36°C (hypothermia) or > 39°C (high fever), particularly when associated with other signs of organ dysfunction (e.g., hemodynamic instability, respiratory distress, altered mental status) or a high clinical suspicion of severe infection/sepsis, be admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate aggressive investigation and treatment of the underlying cause, continuous cardiorespiratory monitoring, management of the systemic effects of the temperature derangement, and comprehensive organ support (Strong recommendation, low-quality evidence). A persistent and severe abnormality in body temperature is rarely an isolated finding. It is a cardinal vital sign and a key indicator of a significant underlying systemic process, most commonly sepsis. It can also be caused by severe environmental injuries, central nervous system catastrophe, or severe endocrine emergencies. The decision for ICU admission is driven by the fact that the temperature derangement signifies a critical illness that requires intensive monitoring and management of its cause and consequences. ICU admission is crucial for managing:
o Sepsis and Septic Shock: This is the most common cause. A temperature <36°C (hypothermia) or >38.3°C (fever) is part of the diagnostic criteria for Systemic Inflammatory Response Syndrome (SIRS), a component of older sepsis definitions. Hypothermia in sepsis is often a marker of severe illness and poor prognosis. Management requires aggressive resuscitation, antibiotics, source control, and organ support in an ICU. o Severe Environmental Injuries: As detailed previously, heat stroke or severe accidental hypothermia requires specialized temperature management and multi-organ support in an ICU. o Central Nervous System Emergencies: Brain injury (traumatic or stroke) can disrupt thermoregulation, and fever in this context can worsen secondary brain injury, requiring aggressive temperature control in a Neuro-ICU.
|
33, 377, 378, 379, 380, 381 |
|
respiratory Parameter |
|
|
We recommend that adult patients presenting with severe derangements in respiratory parameters indicating acute or impending respiratory failure be promptly admitted to an Intensive Care Unit (ICU) or or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Indications for this level of care include, but are not limited to: clinical signs of severe respiratory distress (e.g., Respiratory rate >30 breaths/min tachypnea or < 10 breaths /min, use of accessory muscles, inability to speak); evidence of severe gas exchange abnormalities (e.g., PaO2/FiO2 ratio <200 SpO2 < 92 % on room air, or SpO2 <90% on high-flow oxygen; acute hypercapnia with respiratory acidosis [pH <7.30]); or evidence of respiratory muscle weakness indicating impending respiratory arrest (e.g., vital capacity <20 mL/kg). This is to facilitate advanced respiratory support (including non-invasive or invasive mechanical ventilation), continuous cardiorespiratory monitoring, management of the underlying cause, and treatment of potential complications (Strong recommendation, moderate-to-high quality evidence). The key respiratory parameters indicating a need for ICU-level care fall into three main categories:
|
33, 225, 226, 227, 228, 229, 230, 231, 263, 264, 361 |
|
Radiography/Ultrasonography/Tomography |
|
|
We recommend that adult patients whose imaging studies (radiography, ultrasonography, or tomography) reveal a critical finding be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such critical findings include, but are not limited to, those indicating acute respiratory failure (e.g., diffuse bilateral opacities consistent with moderate/severe ARDS), obstructive shock (e.g., cardiac tamponade, massive pulmonary embolism with right ventricular strain, tension pneumothorax), catastrophic vascular events (e.g., acute aortic dissection, ruptured aneurysm), severe neurological compromise (e.g., large intracranial hemorrhage or infarct with mass effect, Cerebral vascular hemorrhage, contusion, subarachnoid haemorrhage, or sever spine injury), or major visceral injury (e.g., perforated viscus, severe solid organ injury with hemorrhage). This is to facilitate immediate life support, intensive monitoring for deterioration, management of organ dysfunction, and timely therapeutic interventions (surgical, radiological, or medical) (Strong recommendation, moderate-quality evidence). A patient with a critical imaging finding is admitted to the ICU to:
Warning Imaging Findings Often Requiring ICU Admission (such as): 1. Chest Imaging (CXR, CT, Ultrasound):
2. Head Imaging (CT, MRI):
3. Abdominal Imaging (CT, Ultrasound):
|
33, 165, 168, 194, 195, 196, 170, 171, 172, 173, 174, 175, 382, 383, 384 |
|
abnormalities in blood indices |
|
|
We recommend that adult patients presenting with critical abnormalities in blood indices that signify or pose an immediate risk of life-threatening organ dysfunction, hemorrhage, or severe systemic illness. T be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. Such critical findings include, but are not limited to, evidence; severe anemia (Hb < 7 gm % ) causing hemodynamic instability or myocardial ischemia or resulting from massive hemorrhage. severe coagulopathy (INR (>5-6)) or severe thrombocytopenia (< 20000/ mm3) with bleeding (e.g., DIC, Thrombotic Thrombocytopenic Purpura (TTP), or HELLP syndrome.) with active bleeding or Severe Leukopenia / severe neutropenia with sepsis or shock or Hyperleukocytosis/Leukostasis (>100,000/µL) leading to respiratory failure or stroke. This is to facilitate aggressive resuscitation (including massive transfusion), continuous monitoring, treatment of the underlying cause, management of organ failure, and reversal or control of the hematologic or biochemical derangement (Strong recommendation, moderate-quality evidence)
ICU admission is crucial for patients with severe abnormalities in blood indices to:
Key Blood Indices and Associated Critical Conditions Requiring ICU Admission: 1. Hematology (Complete Blood Count):
2. Coagulation:
|
33, 385, 386, 387,388 |
|
Laboratory Values (critical biochemical indices) |
|
|
We recommend that adult patients presenting with a severe electrolyte disturbance – characterized by an extreme laboratory value posing immediate risk (e.g., K+ >6.5 mmol/L, K+ <2.5 mmol/L, Na+ <120 mmol/L, Na+ >160 mmol/L, elevated serum lactate (e.g., >2-4 mmol/L) Serum calcium > 12 mg /dL or < 6 mg /d with manifestations, severe symptomatic abnormalities of magnesium, or phosphate) or by life-threatening clinical manifestations such as cardiac arrhythmias, tissue hypoperfusion ,seizures, coma, or respiratory muscle failure – be promptly admitted to an Intensive Care Unit (ICU) or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This is to facilitate continuous cardiac and neurological monitoring, frequent laboratory testing, controlled intravenous administration of corrective therapies, management of organ dysfunction, and treatment of the underlying cause (Strong recommendation, moderate-quality evidence). A severe electrolyte disturbance is a life-threatening condition where the concentration of one or more electrolytes in the blood is abnormal to a degree that causes or poses an immediate risk of severe organ dysfunction. Admission to an ICU or intermediate care unit (IMCU) is crucial because these conditions can lead to:
ICU care is essential for:
|
33, 344, 344, 345, 346, 347, 348, 349, 350, 351, 352, 353, 354, 355, 356, 375 |
|
We recommend that adult patients presenting with a life-threatening glycemic crisis be promptly admitted to an Intensive Care Unit (ICU) or or an intermediate care unit (IMCU) with equivalent capabilities for comprehensive critical care management. This includes patients with: (1) severe hypoglycemia (e.g., blood glucose <65 mg/dL or 3.6 mmol/L) causing significant neurological impairment (e.g., coma, seizures) or requiring a continuous intravenous glucose infusion for stabilization; and (2) severe hyperglycemia (e.g., blood glucose >750 mg/dL or 41.6 mmol/L) consistent with severe Diabetic Ketoacidosis (DKA) or Hyperosmolar Hyperglycemic State (HHS). This admission is to facilitate intensive monitoring of neurological, metabolic, and hemodynamic status; aggressive and controlled intravenous fluid, electrolyte, and insulin/glucose therapy; and management of underlying causes and systemic complications (Strong recommendation, moderate-quality evidence). While a glucose of <70 mg/dL is the alert value, and <65 mg/dL is clinically significant, ICU admission is reserved for life-threatening hypoglycemia. This is characterized by severe neuroglycopenia (brain dysfunction due to glucose deprivation) or a situation where prolonged or recurrent hypoglycemia is highly likely. ICU care is crucial for:
|
33, 111, 112, 113, 114, 115, 116, 132, 133, 134, 135, 136, 137, 138, 392, 393, 394, 395 |
|
Addmsion & Triage of mass casualty incidents , Pandemic and Epidemic |
|
|
We recommend that intensive care units be prepared to handle victims of external and internal disasters, including the collapse of surrounding services due to natural or man-made disasters. Every intensive care unit should have general disaster and evacuation plans within the hospital's plans. (Strong recommendation, moderate -quality evidence). |
1, 33, 188, 189, 190, 396, 398 ,399, 401 |
|
We recommend that the declaration of a Mass Casualty Incident (MCI) be followed by the immediate activation of the institutional disaster plan and a coordinated response from the complete healthcare team. This team must ensure the readiness of the institution and its critical care areas—notably the Emergency Department, operating rooms, and the ICU—to efficiently transition from routine to emergency operations and to augment their capacity for a significant influx of critically ill patients. (Strong recommendation, moderate -quality evidence). |
1, 33, 188, 189, 190, 396, 397, 398, 399, 400, 401, 402 |
|
We suggest at Mass Casualty Incident (MCI) that the emergncy and inetnsive care physicians identify all patients in need of ICU care and those already hospitalized who could be discharged, and then triage and transfer the incoming patients to the most appropriate setting as soon as possible (Strong recommendation, moderate -quality evidence). |
1, 33, 188, 189, 190, 396, 398, 402, 407, 408, 411, 412 |
|
We recommend that national and regional regulatory bodies, in collaboration with hospitals leadership, develop, fund, and regularly exercise comprehensive plans to enable a rapid and surge in intensive care capacity. These plans should aim to accommodate a significant increase over baseline ICU capacity (with models for extreme events targeting at least 300% expansion) by identifying convertible spaces, pre-allocating necessary resources (equipment, supplies, staffing protocols), and integrating flexible design considerations into healthcare building codes. Furthermore, these plans should establish a clear crisis management authority with the mandate to coordinate resources and patient flow across a region during a declared emergency (Strong recommendation, moderate-quality evidence). Major disasters (e.g., severe pandemics, mass casualty incidents from natural disasters or armed conflict) can overwhelm healthcare systems by creating a sudden, massive influx of critically ill patients. The COVID-19 pandemic provided a stark, real-world demonstration of this. A lack of preparedness leads to rationing of care, preventable morbidity and mortality, and collapse of healthcare infrastructure. Therefore, proactive planning is a cornerstone of national health security and public health preparedness. This involves a multi-pronged strategy:
|
1, 10, 33, 188, 189, 190, 397, 399, 400, 401, 403, 410, 411, 412 |
|
We suggest that during mass casualty scenarios, adult patients with severe burns—based on established clinical criteria—may be appropriately managed in general ICU settings to preserve specialized Burn ICU capacity for the most critically injured cases. This approach should be guided by well-coordinated regional and national triage systems to ensure optimal allocation of resources and timely care delivery. (Good practice statement, low-quality evidence). |
1, 33, 188, 189, 190 |
|
We recommend that national and regional regulatory bodies, in collaboration with hospitals leadership, develop, fund, and regularly exercise comprehensive plans for Pandemic & epidemics. These plans should cover national and hospital level. plans should include both triage and dissemination of patients throughout the hospital.Furthermore, these plans should establish a clear crisis management authority with the mandate to coordinate resources and patient flow across a region during a declared epidemics(Strong recommendation, moderate-quality evidence). |
1, 10, 33, 397, 399, 401, 403, 406, 409, 410 |
|
We suggest during Pandemic and Epidemic not using routine laboratory studies alone in determining the nature of illness. (Good practice statement, low-quality evidence). |
1, 36, 38, 402, 404, 405, 406, 407, 408, 414, 415, 416 |
|
We suggest during Pandemic and Epidemic not using scoring systems alone to determine level of care or removal from higher levels of care because these are not accurate in predicting individual mortality(Good practice statement, low-quality evidence). |
1, 36, 38, 402, 403, 404, 405, 406, 407, 408, 413 |
|
ICU discharge |
|
|
We recommend avoiding discharge from ICU “after hours” (“night shift”, after 7 pm in institutions with 12-hr shifts). In addition, best practice would seek to optimize evening and night coverage and services(Good practice statement, low-quality evidence). |
1, 36, 419 |
|
We suggest discharging patients at high risk for mortality and readmission (high severity of illness, multiple comorbidities, physiologic instability, and ongoing organ support) to a step-down unit intermediate care units (IMCU) then to the regular ward |
1, 27, 33, 36, 419 |
|
We recommend that the decision to discharge a patient from an Intensive Care Unit (ICU) be based on a structured, multi-domain assessment. This assessment should be guided by institutional policies that are based on a framework of objective criteria. Key domains to consider include: · the resolution of the acute life-threatening condition that prompted admission · the achievement of physiological stability · Neurological status: be adequately handled and monitored at the receiving unit · Genanral status of the patient be adequately handled and monitored at the receiving unit · able to protect their airway (unless there is a chronic baseline deficit) · Respiratory status: Stable RR 12-24 breaths / min & SpO2 ≥ 92% on room air OR patient's individual Known baseline value is met. · Cardiovascular status:stable hemodynamics, HR, BP, (OR patient's individual Known baseline value) with no arrhythmia or tolerable intermittent arrhythmia for at least 24 hr, with no signs of active bleeding or hypervolemia / hypovolemia · the absence of need for ongoing ICU-specific interventions · with adequately urine output, electrolyte level, and renal function and if need renal replacement therapy is possible outside the ICU · the patient's prognosis and goals of care · the capabilities and availability of resources at the next appropriate level of care (e.g., an intermediate care unit or general ward). This is to facilitate a safe,
timely, and appropriate transition of care that minimizes the risk of
clinical deterioration and ICU readmission (Strong recommendation,
moderate-quality evidence).
|
1, 27, 33, 419 |
|
We suggest that patients with cardiovascular disorders be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to, stable hemodynamics without the need for intravenous vasopressor or inotropic support(Systolic blood pressure ≥ 90 mmHg - Diastolic blood pressure ≥ 50 mm Hg -Heart rate > 50 beats /min. and < 130 beats/minutes) (OR patient's individual Known baseline value); stable respiratory status (OR patient's individual Known baseline value), having been weaned from invasive mechanical ventilation and requiring a low level of oxygen support manageable on a ward or IMCU (SPO2 > 92 % on room air or alternative oxygen supply < 6 L/min- Respiratory rate < 30 breaths/min and > 10 breaths /min.); and the absence of life-threatening cardiac arrhythmias or ongoing myocardial ischemia(Absence of life-threatining arrhythmia for 24 hours -No continuous antiarrhythmic or vasoactive agent) and Resolution of the Acute Insult. This is to ensure a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence).
|
1, 33 |
|
We suggest that adult patients admitted to the ICU for a pulmonary disorder be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to, successful liberation from invasive mechanical ventilation (as demonstrated by passing a spontaneous breathing trial and successful extubation or stable non-invasive positive pressure ventilation settings with plan for chronic home ventilation) ; stable and adequate gas exchange (e.g., SpO2 ≥ 92% on a low level of oxygen support [FiO2 ≤ 0.4]); absence of respiratory distress (e.g., respiratory rate <25/min, no accessory muscle use); and an effective cough with the ability to manage secretions. This is to ensure a safe transition of care and minimize the risk of respiratory decompensation and ICU readmission (Strong recommendation, moderate quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe gastrointestinal disorder be considered for discharge from the Intensive Care Unit (ICU) when they demonstrate resolution of the acute crisis and have achieved physiological stability, Neurological Stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: cessation of life-threatening bleeding with no evidence of re-bleeding; control of intra-abdominal sepsis source; resolution of shock with discontinuation of intravenous vasopressor/inotropic support; stable respiratory status after liberation from mechanical ventilation; and improving or stable organ function. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe neurologic disorder be considered for discharge when they demonstrate sufficient neurological and physiological stability: conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit) , demonstrate stable respiratory function and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: a stable and protected airway (e.g., patient is successfully extubated with adequate consciousness and protective reflexes, or has a stable tracheostomy with manageable respiratory needs); controlled intracranial pressure without need for intensive medical or surgical intervention; cessation of status epilepticus with seizures controlled on a stable medication regimen; and resolution of associated hemodynamic shock and respiratory failure. This is to facilitate a safe transition of care and minimize the risk of neurological deterioration or other complications requiring ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe endocrine or electrolyte disorder be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: resolution of hemodynamic shock with discontinuation of intravenous vasopressor/inotropic support; neurological stability with the patient being conscious, alert, and able to protect their airway (unless there is a chronic baseline deficit); stable respiratory function after liberation from mechanical ventilation; and correction of the life-threatening metabolic or electrolyte derangement to a safe level that can be managed with oral, subcutaneous, or intermittent intravenous therapies on a ward. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We suggest that adult patients admitted to the ICU for a severe renal disorder be considered for discharge when they demonstrate resolution of the acute life-threatening uremic complications and have achieved hemodynamic and respiratory stability. Key criteria for discharge readiness include, but are not limited to: correction of severe metabolic acidosis and life-threatening hyperkalemia; resolution of severe volume overload and its associated respiratory compromise; neurological stability with resolution of uremic encephalopathy; and stabilization of renal replacement therapy status (either recovery of native kidney function no longer requiring renal replacement therapy, or hemodynamic stability sufficient to transition from continuous to intermittent dialysis manageable in a non-ICU setting). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
1, 33 |
|
We recommend that adult patients admitted to the ICU for sepsis or septic shock be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: resolution of shock with discontinuation of intravenous vasopressor or inotropic support; stable respiratory status after liberation from mechanical ventilation and on minimal oxygen support; evidence of adequate source control of the infection; and a clear trajectory of improvement or stabilization of other organ dysfunctions (e.g., neurological, renal, hepatic, hematological, as may be reflected in a decreasing SOFA score). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
|
We recommend that adult patients admitted to the ICU for severe trauma and injuries be considered for discharge when they demonstrate resolution of the acute life-threatening crisis and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: control of hemorrhage with resolution of shock and discontinuation of intravenous vasopressor/inotropic support; stable respiratory status after liberation from mechanical ventilation and with a secure, protected airway; neurological stability with controlled intracranial pressure and cessation of status epilepticus; and evidence that the underlying injuries have been definitively managed or stabilized such that immediate re-operation is not anticipated. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
|
We recommend that adult patients admitted to the ICU for surgical or postoperative care be considered for discharge when they demonstrate resolution of the acute crisis and have achieved physiological stability, including neurological stability (e.g., conscious, alert, and able to protect their airway, unless there is a chronic baseline deficit), and no longer require ICU-specific interventions. Key criteria for discharge readiness include, but are not limited to: control of surgical hemorrhage with no evidence of ongoing bleeding; control of any surgical sepsis source; resolution of shock with discontinuation of intravenous vasopressor or inotropic support; stable respiratory status after liberation from mechanical ventilation; and evidence of improving or stable organ function. A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence acute crisis. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |
|
We recommend that adult patients admitted to the ICU for severe snake or scorpion envenomation be considered for discharge when they demonstrate resolution of the acute life-threatening systemic envenomation syndrome and have achieved physiological stability. Key criteria for discharge readiness include, but are not limited to: for neurotoxic envenomation, recovery of respiratory muscle function with successful liberation from mechanical ventilation and a secure airway; for hemotoxic envenomation, cessation of bleeding and sustained normalization of coagulation parameters; for cardiotoxic envenomation, resolution of shock with discontinuation of intravenous vasopressor/inotropic support and absence of life-threatening arrhythmias; and improvement or stabilization of any associated organ dysfunction (e.g., acute kidney injury). A period of observation (e.g., 12-24 hours) after achieving stability is often prudent to ensure no recurrence of toxicity in ICU then step down to IMCU if need this level of care then A period of observation (e.g., 12-24 hours) befor discharge to ward or home. This is to facilitate a safe transition of care and minimize the risk of clinical deterioration and ICU readmission (Strong recommendation, moderate-quality evidence). |
33, 27 |