
Book
Cow Milk Protein allergy
- Introduction
Cow's milk allergy may be defined as a reproducible adverse reaction to one or more milk proteins (usually caseins or whey β-lactoglobulin).4
Cow's milk allergy is classified by the underlying immune mechanism, timing of presentation and organ system involvement.
➡️Epidemiology
The perception of milk allergy is far more frequent than confirmed CMA.
Symptoms suggestive of cow's milk allergy based on self-reports vary widely, and only about one in three children presenting with symptoms is confirmed to be cow's milk allergic using strict, well defined elimination and open challenge criteria. 5 With these criteria, cow's milk allergy is shown to affect between 1.8% and 7.5% of infants in the first year of life. This may still be an overestimate.6 Clinicians should therefore anticipate that between 2–3% of children have cow's milk allergy.7
Patients with CMA develop gastrointestinal symptoms in 32 to 60% of cases, skin symptoms in 5 to 90%, and anaphylaxis in 0.8 to 9% of cases. This frequency of anaphylaxis is the main concern pointed out in many CMA studies.8
In Egypt, there are no population-based surveys on prevalence of cow milk allergy in adults or children.9
➡️Etiology and pathogenesis of cow’s milk allergy
Cow’s milk allergy (CMA) results from a defect in the immune tolerance toward cow’s milk proteins. The immune reactions involved can be immunoglobulin (Ig) E-mediated, cell-mediated or both (Table 1).10,11
The major milk proteins incriminated in CMA are whey proteins (ß-lactoglobulin) and caseins. 12,13
➡️IgE-Mediated CMA (Immediate hypersensitivity reaction)
The mechanism of IgE-mediated allergy is more understood than non- IgE-mediated reactions and is relatively easily suspected because of rapid onset of symptoms (Table 1). It occurs in 2 steps, the first is the sensitization step that starts when the immune system is abnormally programmed to produce IgE antibodies to milk proteins. These antibodies when binding to the surface of mast cells and basophils, prime them with an allergen-specific trigger. The second step is the activation of the primed mast cells upon re-exposure to milk proteins and subsequently trigger the rapid release of powerful inflammatory mediators. 4,10
➡️Non-IgE-mediated (Delayed hypersensitivity reaction)
In non-IgE-mediated reactions usually there is delayed onset of symptoms occurring within 1 hour to several days following cow’s milk intake. Usually the symptoms are confined to the gut ranging from allergic proctatitis to severe shock-like reactions with metabolic acidosis that is characteristic for the food protein – induced enterocolitis syndrome (Table 1).14-16
➡️Risk Factors
There are several risk factors for development of CMA, such as; artificial feeding, prematurity, antibiotic use, over intake or deficiency of vitamin D and family history.
➡️Diagnosis of CMA
The diagnosis of CMA should be undertaken in a stepwise approach, starting with history taking, clinical examination, and tests for specific IgE and dietary cow milk elimination/challenge.
➡️Clinical assessment
History taking and physical examination can establish the likelihood of the diagnosis, suggest whether an IgE or non-IgE mechanism is involved, can provide a guide to appropriately select and interpret further investigations and identify the potential food triggers.
A thorough medical history should ascertain the following information:
- The food suspected of provoking the reaction and the quantity ingested,
- The form of food (raw, cooked or baked),
- The length of time between ingestion and the development of symptoms,
- Whether ingesting the suspected food produced similar symptoms on other occasions,
- How long ago the patient experienced the last reaction to the food.
➡️Clinical examination: In conjunction with the medical history, clinical examination helps determine the useful diagnostic test or tests.17 Atopic asthma, allergic rhinitis, or atopic dermatitis might indicate an increased risk of IgE-mediated food allergy. Failure to thrive or dermatitis herpetiformis, might indicate other non–IgE-mediated, autoimmune, or nonimmunologic disease. The clinical evaluation should include examination of nutritional status and growth.18
Table 1 Main characteristics of IgE-mediated and non-IgE-mediated allergy
|
Characteristic |
IgE-mediated |
Non-IgE-mediated |
|
Time from exposure to reaction |
Minutes to 2 h |
Several hours to days |
|
Severity |
Mild to anaphylaxis |
Mild to moderate. May cause failure to thrive and edema |
|
Duration |
May persist beyond 1 year of age |
Usually resolved by 1 year of age |
|
Diagnosis |
Specific serum IgE, skin prick tests Oral challenge |
Elimination Oral challenge |
Adapted from: Lifschitz C, Szajewska H;201519
➡️Clinical spectrum of CMA:
From a clinical and diagnostic standpoint, it is most useful to subdivide food hypersensitivity disorders according to the predominant target organ and immune mechanisms (Table 2, 3 and 4).
Table 2. Clinical spectrum of food allergy:
|
|
IgE-mediated min to 2 h |
Non-IgE or cell-mediated 2 h to several days |
Combined IgE and cell-mediated |
|
Skin |
Urticaria/ angioedema |
Allergic contact dermatitis |
Atopic dermatitis |
|
Respiratory |
Bronchial hyperreactivity
Rhino-conjunctivitis |
Heiner's syndrome
Extrinsic allergic alveolitis |
Bronchial asthma |
|
GIT |
Oral allergy syndrome (food pollen syndrome)
Gastrointestinal anaphylaxis |
Food protein induced enterocolitis Food protein induced allergic proctocolitis |
Allergic eosinophilic esophagitis
Eosinophilic gastroenteritis |
|
Generalized |
Anaphylaxis, and food associated, exercise-induced anaphylaxis |
||
Table 3: Gastrointestinal food hypersensitivities
|
Disorder |
Mechanism |
Symptoms |
Diagnosis |
|
Pollen‐food allergy syndrome (oral allergy syndrome) |
IgE-mediated |
Mild pruritus, tingling and/or angioedema of the lips, palate, tongue or oropharynx; occasional sensation of tightness in the throat and rarely systemic symptoms |
Clinical history and positive SPT to relevant food proteins (prick‐to‐prick method); ± oral challenge (positive with fresh food, negative with cooked food) |
|
Gastrointestinal anaphylaxis |
IgE-mediated |
Rapid onset of nausea, abdominal pain, cramps, vomiting, and/or diarrhea; other target organ responses, i.e. skin, respiratory tract, often involved |
Clinical history and positive SPTs or sIgE; ± oral challenge |
|
Allergic eosinophilic oesophagitis |
IgE and/or cell mediated |
Gastro-oesophageal reflux or excessive spitting up or emesis, dysphagia, intermittent abdominal pain, irritability, sleep disturbance, failure to respond to conventional reflux medications |
Clinical history; SPTs; endoscopy and biopsy; elimination diet and challenge |
|
Allergic eosinophilic gastroenteritis |
IgE and/or cell mediated |
Recurrent abdominal pain, irritability, early satiety, intermittent vomiting, failure to thrive and/or weight loss |
Clinical history; SPTs; endoscopy and biopsy; elimination diet and challenge |
|
Food protein induced proctocolitis |
Cell mediated |
Gross or occult blood in stool; typically thriving; usually presents in first few months of life |
SPTs negative; elimination of food protein results in clearing of most bleeding within 72 h; ± endoscopy and biopsy; challenge induces bleeding within 72 h |
|
Food protein induced enterocolitis |
Cell mediated |
Protracted vomiting and diarrhea (± bloody) not infrequently with dehydration; abdominal distention, failure to thrive; vomiting typically delayed 1–3 h post feeding |
SPTs negative; elimination of food protein results in clearing of symptoms within 24–72 h; challenge induces recurrent vomiting within 1–2 h, ∼15% develop hypotension |
|
Food protein induced enteropathy, e.g. coeliac disease (gluten sensitive enteropathy) |
Cell mediated |
Diarrhea or steatorrhea, abdominal distention and flatulence, weight loss or failure to thrive, ± nausea and vomiting, oral ulcers |
Endoscopy and biopsy IgA; elimination diet with resolution of symptoms and food challenge; coeliac disease: IgA anti-gliadin and anti-transglutaminase antibodies |
sIgE, specific immunoglobulin E; SPT, skin prick test. Quoted from Sampson, 200520
Table 4. Respiratory food hypersensitivities:
|
Disorder |
Mechanism |
Symptoms |
Diagnosis |
|
Allergic rhino-conjunctivitis |
IgE mediated |
Periocular pruritus, tearing, and conjunctival erythema, nasal congestion, rhinorrhea, sneezing |
Clinical history, SPTs, elimination diet, food challenge |
|
Asthma |
IgE and cell mediated |
Cough, dyspnea, wheezing |
Clinical history, SPTs, elimination diet, food challenge |
|
Heiner's syndrome (food induced pulmonary hemosiderosis) |
Unknown |
Recurrent pneumonia, pulmonary infiltrates, iron deficiency anemia, failure to thrive |
Clinical history, peripheral eosinophilia, milk precipitins (if due to milk), ± lung biopsy, elimination diet |
- IgE, immunoglobulin E; SPT, skin prick test. Adapted from Sampson 200520
Prognosis: Several studies found that 15% of children with IgE-mediated CMA remained allergic after 8.6 years while all children with non-IgE-mediated CMA outgrew their allergy by 5 years.6
The Cow's Milk-related Symptom Score (CoMiSS) is a clinical resource for primary healthcare providers which aims to increase awareness of CMPA symptoms.
Co-Miss score for clinical evaluation of CMA:
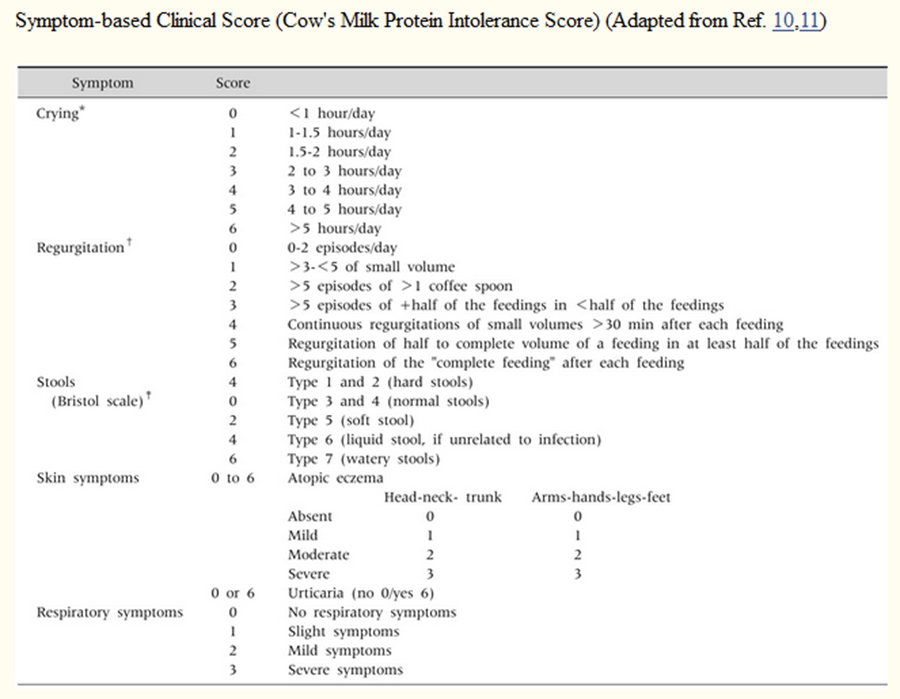
A score of 12 or more indicates that symptoms are cow milk related, potentially CMA. Adapted from DRACMA 2010 and Kattan et al 2016.4,21
➡️Specific IgE-based tests:
Detection of specific IgE in IgE mediated reactions can be performed through either skin prick test (SPT) or serum specific IgE(sIgE) measurement. All IgE based tests should be interpreted in the context of the history. This is because a number of sensitized patients will not react to ingestion of cow milk.22
Serum CMP specific IgE measurement can be especially helpful in patients with severe systemic manifestations for fear of anaphylaxis, those with extensive eczema, or those who could not stop antihistamines where skin testing is not feasible. The sensitivity is greater than 90% for skin testing and 70%–90% for serum food-specific IgE measurement. The specificity of both tests is less than 50%.22,23
In the presence of a good clinical history, cut-off levels for SPT wheal size of ≥ 3 mm larger than the negative control or sIgE ≥ 0.35 kU/L is strongly supporting diagnosis of CMA.24
Results of skin prick tests and specific IgE with ≥ 95% positive predictive values
|
Test |
Infants ≤ 2 years |
> 2 years |
|
Skin prick test (wheal diameter in mm) |
6 |
8 |
|
Specific IgE levels (U/mL) |
5 |
15 |
Quoted from Du Toit et al., 200925.
➡️The basophil activation test (BAT):
The BAT is a flow cytometry-based assay of the expression of activation markers on the surface of basophils following stimulation with allergen.26 It is still not available for practical use in Egypt.
➡️Atopy patch test:
There is insufficient evidence for the routine use of atopy patch test for the evaluation of cow's milk allergy and does not have an additional value in predicting outcomes of OFC.17
Total serum IgE measurements have negligible -if any- role in the diagnosis of food allergy .22
➡️The elimination diet in the work-up of CMA:
Milk elimination is integral to the diagnosis of CMA especially in cases with negative specific IgE result. A definite improvement in symptoms without the need for medication supports the diagnosis. The duration of elimination ranges from 3 to 5 days in children with immediate clinical reactions (eg, angioedema, vomiting, exacerbation of eczema within 2 hours) to 1 to 2 weeks in children with delayed clinical reactions (eg, exacerbation of eczema, rectal bleeding, ). In patients with gastrointestinal reactions (eg, chronic diarrhea, growth faltering), it may take 2 to 4 weeks on a CMP-free diet to judge the response. Care should be undertaken to avoid accidental ingestion and contact with CM and or inhalation of milk vapor (strict elimination).5,27 Goat’s and sheep’s milk should be strictly avoided because of high cross reactivity with CMP.28 Maternal elimination diet is used in case of exclusively breast-fed infants.
➡️Oral Food Challenge (OFC):
The clinician should consider OFC test to confirm the diagnosis of CMA unless there is clinical history consistent with anaphylaxis.16 In patients who demonstrate significant improvement on the elimination diet, the diagnosis of CMA should be confirmed by a standardized oral challenge test. OFC is also indicated to demonstrate tolerance and monitor immunotherapy.27
In the first year of life, a challenge test should be performed with an infant formula based on cow’s milk. Fresh pasteurized cow’s milk can be used above 12 months of age. A false positive challenge due to primary lactose intolerance, may be avoided by using lactose-free CMP-containing formula or milk.27
The starting dose during an oral milk challenge should be lower than a dose that can induce a reaction and then be increased stepwise to 100mL (eg, in children with a delayed reaction, stepwise doses of 1, 3.0, 10.0, 30.0, and 100mL may be given at 30-minute intervals). If severe reactions are expected, then the challenge should begin with minimal volumes (eg, stepwise dosing of 0.1, 0.3, 1.0, 3.0, 10.0, 30.0, and 100mL given at 30-minute intervals). There should be documentation of any signs and symptoms and the amount of milk that provokes symptoms. If no reaction occurs, then the milk should be continued at home every day with at least 200 mL/day for at least 2 weeks. The parents should be contacted by telephone to document any late reactions.27
➡️Differential diagnosis of CMA:
So, the accurate diagnosis depends on high index of suspicion and exclusion of the extremely common functional GI disorders which affects approximately half of infants (40-60%) all over the world.28
For infants presenting with vomiting and posseting: In functional infant regurgitation. the vomiting tends to be effortless and does not upset the infant, and pain is not usually prominent. However, this is not the case in cow’s milk allergic infants with vomiting who are often miserable, rather irritable babies who suffer frequent back-arching and screaming episodes. Feed refusal and aversion to lumps are also prominent features.5
For infants presenting with infant colic: Colic is often confused with simple fussiness, and adding unsortable or inconsolable crying as an additional criterion will help identify ‘true’ colic from simple fussiness [Middle East Consensus Statement on the Diagnosis and Management of Functional Gastrointestinal Disorders in <12 Months Old Infants.28 Observational studies have suggested cow’s milk allergy as a contributing factor in some infants demonstrating extreme colic.5
➡️For infants presenting with diarrhea:
Lactose intolerance can be confused with non-IgE mediated cow’s milk allergy as symptoms overlap. Lactose intolerance should be considered where patients present only with typical gastrointestinal symptoms including abdominal discomfort, bloating, flatulence, and explosive non-bloody watery diarrhea.5
A common cause of diarrhea among infants and toddlers is functional diarrhea (Toddler's diarrhea) which is characterized by daily painless recurrent passage of 4 or more large unformed stools for more than 4 weeks in a well growing child (6 to 60 months age).29
For well thriving infants presenting with bloody stools (suggestive of allergic proctosigmoiditis), exclude presence of anal fissure and gut infections. But if the bleeding is significant or associated with severe anemia, growth failure or systemic manifestations, the differential diagnosis should include primary immune deficiency, inflammatory bowel disease, antibiotic associated diarrhea and other gut conditions.
For children presenting with dysphagia: This symptom always warrants endoscopy to exclude presence of anatomical esophageal abnormalities (stricture, web) and get biopsies for diagnosis of eosinophilic esophagitis.5
Management of CMA:
Principles of management:
Key principles in the management of CMA:
▪️ The key principle in the management of CMA, regardless of the clinical type, is dietary elimination of CMP.
▪️ A substitute formula may not be necessary in infants who are breastfed and children above the age of 2 years.
▪️ Replacement of cow’s milk with a substitute formula is recommended for children below the age of 2 years and non-breastfed children.
➡️Elimination and avoidance of CMP
The management of CMA comprises the avoidance of cow’s milk and cow’s milk products and dietary substitution with an allergenically and nutritionally suitable milk alternative.4 Avoidance of CMP is not limited to exposure via the oral route.30-32 Avoidance of other bovine proteins should be evaluated on a case-by-case basis; while practically all children allergic to beef are allergic to milk,33the opposite is not true.34 A periodical re-evaluation of cow’s milk tolerance every 6-12 months with an open OFC (until tolerance develops) is recommended. Different types of formulas are available to replace cow’s milk in managing CMA.35 The choice of substitute formula should take into account the patient’s preferences, dietary requirements and individual circumstances, as well as cost and availability of the formula.36
Strategies for the management of CMA
➡️Exclusively breastfed children:
Mothers should be encouraged to continue breastfeeding and usually do not require dietary dairy restrictions unless the infant has symptoms whilst being breastfed. The incidence of CMA in exclusively breastfed children is very low; approximately 0.5% of breastfed children have CMA.37 As with all cases of CMA, avoidance of CMP is essential. It takes an average of 2–4 weeks for symptoms to improve or disappear. If symptoms do not improve after 2–4 weeks, an alternative diagnosis should be considered. If symptoms improve or disappear during maternal elimination diet, an open OFC can be performed 6 months later.38
➡️Formula-fed children:
Avoidance of CMP from the diet is essential. eHF is recommended as a substitute to cow’s milk formula in mild-to-moderate cases. AAF is recommended for infants presenting with anaphylaxis, allergic eosinophilic oesophagitis or if the symptoms in mild-to-moderate cases do not improve on eHF after 2–4 weeks.39
➡️Cross reactivity:
Studies on cross reactivity using oral challenges showed that 9.7% of 62 children with CMA reacted to beef. Well-cooked beef is less likely to cause symptoms for those with CMA. There is extensive cross-reactivity among sheep’s, cow’s, and goat’s milk but not with camel’s milk.
Special considerations:
Immunotherapy for CMA:
While there may seem to be potentially large benefits of oral immunotherapy in the management of CMA, frequent and serious adverse events have also been associated with its use. Oral immunotherapy is a promising but still experimental method to treat children with cow’s milk allergy.39 Until further research is done, immunotherapy is not recommended in the treatment of CMPA.
Prevention of cow’s milk protein allergy
Family history is the most important determinant of allergic risk in infancy.
P[ZAE1] revention in high-risk infants:
• Exclusive breastfeeding for 4–6 months. Some recent studies report that early exposure to CMP might promote tolerance.
• When breastfeeding is not possible, consider a hydrolyzed formula. There is no conclusive evidence to support the use of formulas with reduced allergenicity for preventive purposes in healthy infants without a family history of allergic disease.
• Avoidance of CMP during pregnancy is not necessary
