
كتاب
UPPER AND LOWER EYELIDS AFFECTION
- IV- ENTROPION OF THE EYELID
-Entropion
Inward rolling of the eyelid margin
Fig.13: Entropion of the lower eyelid in a foal.

Fig.14: Entropion of
the upper eyelid in a goat.
Causes
1- Conformational.
2- Spastic.
3- cicatricial .
4- subsequent to alteration in globe position (enophthalmos) or size (phthisis/microphthalmos).
Clinical Signs of Entropion
1- Rolling in of the eyelid.
2- Blepharospasm with further rolling in of the eyelid (“spastic entropion”).
3- Excoriation and maceration of the eyelid surface from constant contact with tears.
4- Rubbing of the affected area.
5- Corneal ulceration.
6- Corneal melanosis and vascularization in chronic cases.
7- Conjunctival hyperemia.
8- Epiphora or mucoid discharge.
Treatment of Entropion
- The various methods of treating entropion depend on the level of facial maturity, species, severity and position of eyelid abnormality.
- Eliminate other causes of spastic entropion before deciding on the extent of surgical resection.
- entropion progresses or improves with maturity in some animals, permanent surgical correction of entropion is best delayed until facial maturity is reached.
The general principles apply to all surgical techniques are
1- Accurately assess extent of skin resection before induction of anesthesia.
2- Undercorrection, with the need for a second operation, is preferable to overcorrection, which causes cicatricial ectropion.
3- Minimize surgical tissue trauma.
4- It is not necessary to remove orbicularis oculi muscle; doing so increases hemorrhage, operating time, postoperative edema, and risk of infection.
5- Use fine suture material (4/0 or smaller in dogs and cats).
6- Place multiple, closely spaced sutures of small “bites.”
7- Use an Elizabethan collar until 2 to 3 days after suture removal.
8- Provide adequate postoperative analgesia for the first 7 to 10 days.
9- For the first few days after surgery, while the tissues are swollen, the eyelid may appear overcorrected, but as swelling subsides (over 5 to 7 days) the correction can be better evaluated.
The technique of correction Entropion
1- Temporary “Tacking” Techniques ( Stapling technique - Suture technique)
- When surgery should not be performed in patients with a temporary cause of entropion, such as transient enophthalmos due to lack of orbital fat, as in young animals, especially foals.
- surgical staples have been used as they are quicker, less traumatic, and less irritating,
Persist in the tissue longer than sutures, and can be applied without general anesthesia.
- An Elizabethan collar can often be removed a few days after staples are placed.
- A topical antibiotic ointment is used initially.
- The staples are left in place for as long as necessary. In some animals tacking may have to be repeated several times until facial maturity is reached and permanent corrective surgery can be performed.
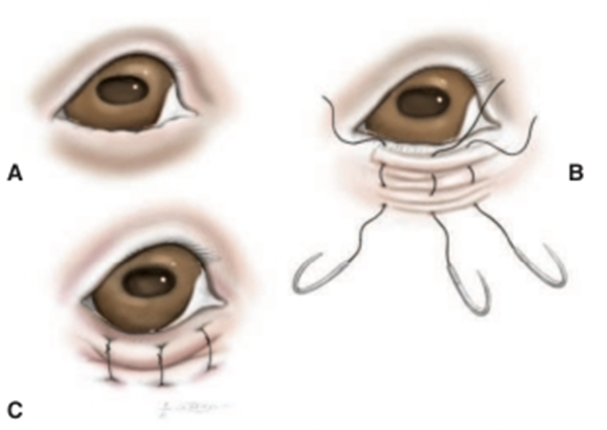
Fig. 15: Temporary “tacking” sutures used to correct entropion in immature animals or animals with a transient cause for Entropion(David et al, 2008).
A- Lower eyelid entropion.
B- Placement of a series of vertical mattress sutures.
- The first bite is taken very close to the eyelid margin, and the second bite is taken a few millimeters distant to the first. A 2/0 or 3/0 nylon suture is recommended.
C- As the suture is tightened a small furrow between the two bites is created and causes the eversion of the eyelid. The sutures are tied with the knots as distant from the eye as possible.

Fig.16: Lower eyelid entropion in a Labrador retriever puppy that
temporarily everted with surgical staples (David et al, 2008).
1- Injection Technique in Lambs
- entropion in lambs has been treated with subcutaneous injection of a liquid to physically alter lid alignment.
- Various fluids have been injected to evert the lower eyelid. A subcutaneous injection of Injection of procaine penicillin or long-acting tetracycline , also sterile air (5-15 ml) is effective in many cases.
2- Wedge Resection
- If the cause of entropion is euryblepharon (elongated eyelids), the lower eyelid can be shortened by resection of a full-thickness wedge from its lateral end.
- If the entropion is associated with a “notch” deformity, the wedge can be repositioned to remove the deformed tissue. As with all incisions that involve the eyelid margin, accurate apposition with a two-layer closure is essential.
|
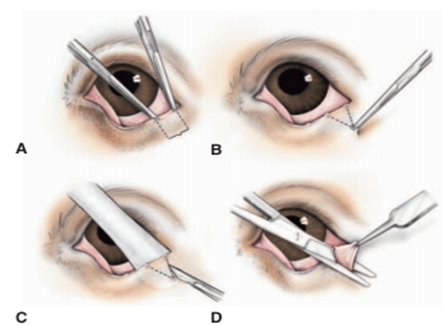
Fig.17: Eyelid wedge resection (David et al, 2008). A- The extent of eyelid margin resected with hemostats or with a dermatologic marker pen. B- The apex of the triangle or “wedge”resected in a similar manner. Usually the height of this triangle is approximately twice its base. C- The skin incision is made with a No. 15 Bard-Parker scalpel while the eyelid is supported by a Jaeger lidplate. D- The subcutis and conjunctiva are cut with straight Mayo or Stevens’s tenotomy scissors, so that the tissue wedge is completely resected.
|
|
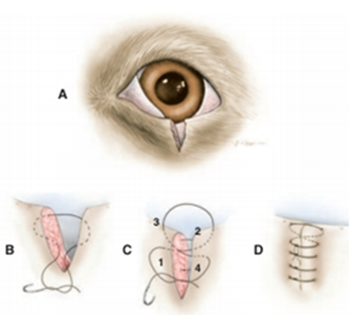
Fig.18: Standard two-layer closure technique (David et al, 2008). A- This technique is used for all eyelid wounds that involve the eyelid margin. B- A buried 3/0 to 5/0 absorbable horizontal mattress suture without penetrating the skin, the margin itself, or the conjunctiva. Suture is placed so that the appositional forces are at the margin, but the knot is distal from it so as to avoid corneal contact ,from the eyelid margin to the apex of the incision so as to close the sub cutis. C- The skin is closed using a figure-of-eight suture of 3/0 or 4/0 silk or braided nylon. Both suture ends are left long at this stage. D- The rest of the skin incision is closed with a series of closely spaced simple interrupted sutures. The ends of the figure-of-eight suture are incorporated into the knot of the firs simple interrupted suture so that they are directed away from the eye. |
1- Hotz-Celsus Procedure
- If the cases are simple, breed-related or conformational entropion can be using a Hotz-Celsus procedure.
- The initial incision parallel to the eyelid margin should be made at the haired-non haired border.
- The length of this first incision is dictated by the length (extent) of inverted eyelid.
- Gentle pressure with the thumb on the lower lid at the point of entropion until the eyelid margin (meibomian gland orifices) can be seen along the whole length will assist with outlining the full lateral and medial extent of entropion.
- The tendency is to make this incision too.
- The real “art” of entropion surgery is in deciding on the amount of tissue to be resected at the widest point.
- The most important point is to ensure that the
- Use of calipers or some other simple method of measurement may assist in resection of a symmetric portion of the contralateral eyelid if that is required.
- The skin incisions are best made with a No. 15 Bard-Parker or No. 64 Beaver scalpel blade.
- The eyelid tissue is then best resected with a small pair of tenotomy scissors such that it has a V-shaped or boat keel–shaped profile.
- The wound is then closed with multiple, small, closely spaced, simple interrupted sutures of 3/0 or 4/0 braided nylon or silk.
- Sutures should be placed perpendicular to the eyelid margin.
- It is easily performed by placement of the first suture centrally (at the widest point of resection) and placement of each subsequent suture such that it bisects the distance still to be sutured.
- Topical antibiotic ointment, an Elizabethan collar, and a systemically administered NSAID for analgesia. Systemic antibiotics are not necessary. Sutures can be removed approximately 10 days postoperatively.
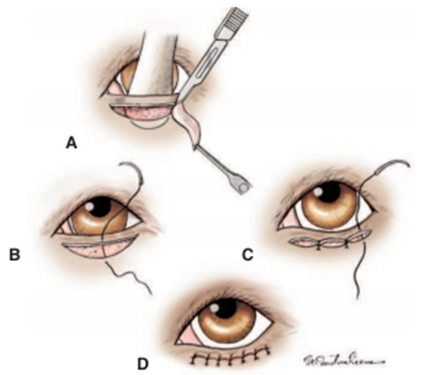
Fig.19: Hotz-Celsus procedure for correction of Entropion (Moore and Constantinescu,1997)
A- A Jaeger lid plate is inserted into the conjunctival fornix to provide support for the incisions.
- The initial incision is made parallel to the eyelid margin at the haired-nonhaired border.
- A second incision is made that arcs between the ends of the first incision.
- The width of the skin to be removed determines the extent of eversion this procedure will create.
B- The defect is closed with a series of simple interrupted skin sutures.
- The first suture placed should be at the widest point of the resected tissue.
C- Each of the following sutures is then placed so as to bisect the space remaining.
D- Final appearance.
1- Medial Canthoplasty
In brachycephalic dogs a syndrome of eyelid, conjunctival, and corneal lesions is seen commonly which called brachycephalic ocular syndrome characterized by :
a- Lower medial Entropion.
b- Breed-related exophthalmos (shallow orbits)
c- Macropalpebral fissure (evident as excessive limbal or scleral exposure)
d- Lagophthalmos (and/or sleeping with the eyelids incompletely closed)
e- Medial caruncular trichiasis
f- Nasal fold trichiasis
g- Pigmentary keratitis
h- Epiphora due to “kinking” of the nasolacrimal canaliculi and obscuring of the puncta.
Aim of surgery
E- To provides a way to neatly correct many of the contributing features of this syndrome, by:
1- shortening the lower and upper eyelids.
2- removing the medial caruncle, and everting the lower medial Entropion.
F- thereby reducing corneal exposure, frictional irritation, and functional nasolacrimal apparatus obstruction.
G- It is recommended for dogs with progressive corneal lesions.
H- It is also suitable for patients with postproptosis exophthalmos that does not resolve and causes lagophthalmos and secondary corneal lesions.
The surgical technique
I- The animal placed in dorsal recumbency with the neck ventroflexed or may be placed in sternal recumbency with the head elevated.
J- Important features of the procedure are avoidance of the lacrimal puncta, meticulous removal of all hair follicles from the medial caruncle and conjunctiva, careful incision of the eyelids, perfect realignment of the eyelid margin, and appropriate postoperative management as for other eyelid procedures.
K- In very severe cases, medial and lateral canthoplasties may be required.
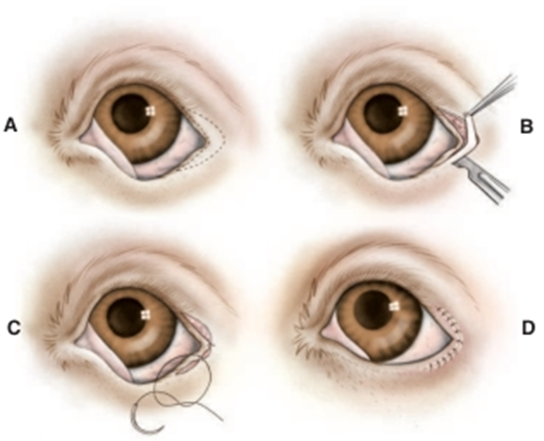
Fig.20: Lateral arrowhead procedure for entropion of the lateral
aspects of the upper and lower eyelids and the lateral canthus (Moore and Constantinescu,1997).
(This isusually performed after a lateral canthal tenotomy).
A- An arrowheadshaped section of tissue to be removed is outlined surrounding the lateral canthus.
- Its dimensions are dictated by the severity and extent of the entropion and may be asymmetric.
B- The tissue is resected with a scalpel blade and tenotomy scissors.
C- The incisions are closed using the rule of bisection, beginning with a suture placed at the lateracanthus.
D- All sutures must be placed perpendicular to the eyelid margin if maximal eversion is to be achieved.
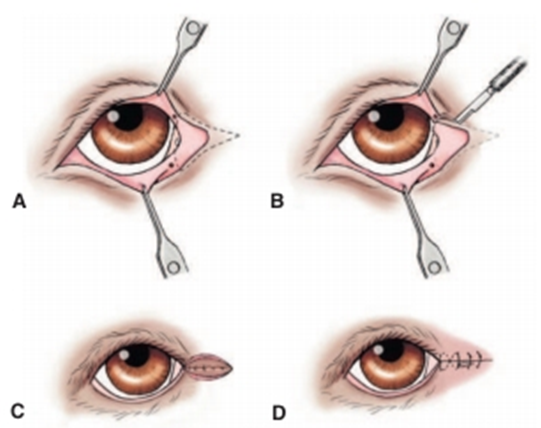
Fig.21: Medial canthoplasty(Moore and Constantinescu,1997).
A- The area to be resected is outlined and should include approximately the medial one fourth of the upper and lower eyelid margins, the medial caruncle, and a section medial to the medial canthus.
- Care is taken to not resect the nasolacrimal puncta.
B- The outlined tissue is resected using a No. 64 Beaver blade.
- The incisions should be perpendicular to the upper and lower eyelid margins where they cross them.
C- A buried mattress suture is used to appose the fresh edges of the canthus, continued as a series of mattress
sutures if required.
D- The skin is closed with a figure-of-eight suture at the new canthus with a series of simple interrupted sutures.
