
Book
the Diagnosis and Management of Thyroid Nodules
- Annexes
Table 1. Quality and Significance of the four levels of evidence in GRADE
|
Quality |
Current definition |
Previous definition |
|
High |
We are very confident that the true effect lies close to that of the estimate of the effect |
Further research is very unlikely to change our confidence in the estimate of effect |
|
Moderate |
We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different |
Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate |
|
Low |
Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect |
Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate |
|
Very low |
We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect |
Any estimate of effect is very uncertain |
Table 2. Factors that determine How to upgrade or downgrade the quality of evidence
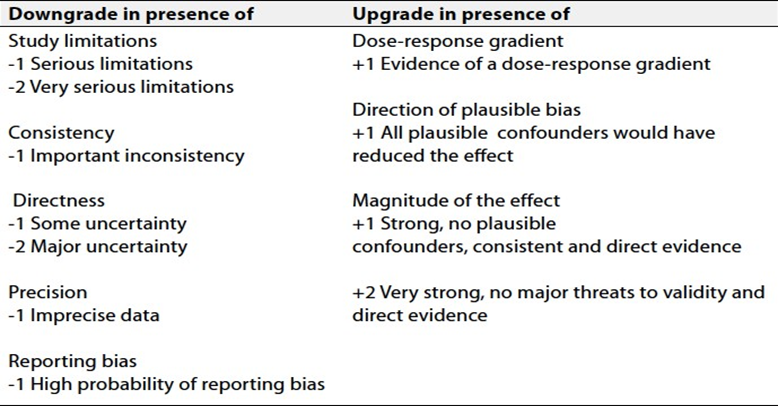
Table 3: EU-TIRADS categories with corresponding malignancy risks and indication of FNAC(8)
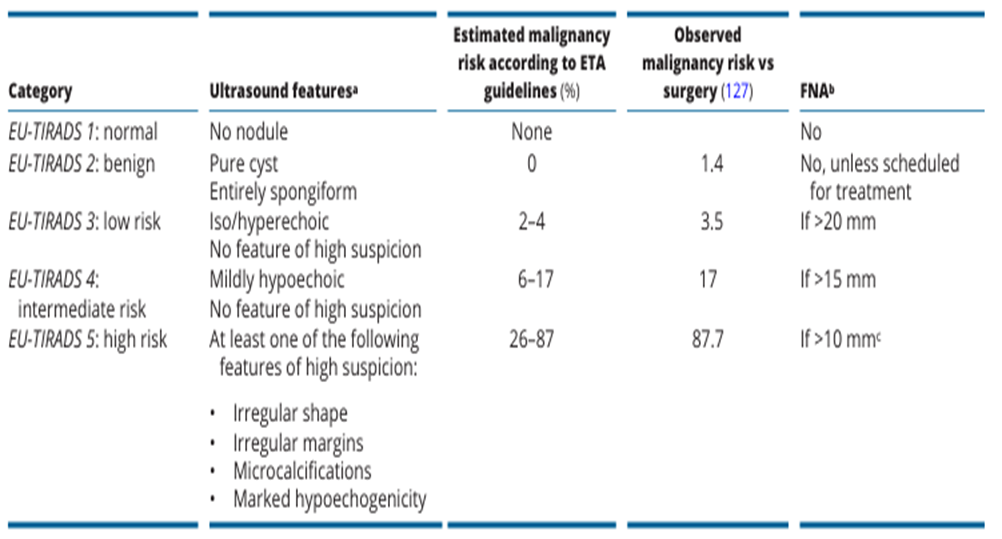
Table 4: Sonographic Patterns, Estimated Risk of Malignancy, and Fine-Needle Aspiration Guidance for Thyroid Nodules (3).
|
Sonographic pattern |
US features |
ROM % |
FNA size cutoff |
|
High suspicion |
Solid hypoechoic nodule or solid hypoechoic component of a partially cystic nodule with one or more of the following features: irregular margins (infiltrative, micro lobulated), microcalcifications, taller than wide shape, rim calcifications with small extrusive soft tissue component, evidence of ETE |
>70–90 |
Recommend FNA at ≥1 cm |
|
Intermediate suspicion |
Hypoechoic solid nodule with smooth margins without microcalcifications, ETE, or taller than wide shape |
10–20 |
Recommend FNA at ≥1 cm |
|
Low suspicion |
Isoechoic or hyperechoic solid nodule, or partially cystic nodule with eccentric solid areas, without microcalcification, irregular margin or ETE, or taller than wide shape. |
5–10 |
Recommend FNA at ≥1.5 cm |
|
Very low suspicion |
Spongiform or partially cystic nodules without any of the sonographic features described in low, intermediate, or high suspicion patterns |
<3 |
Consider FNA
at ≥2 cm a reasonable option |
|
Benign |
Purely cystic nodules (no solid component) |
<1 |
No biopsy |
Table 5: The Bethesda system for reporting thyroid cytopathology, ROM with clinical management recommendations (6).
|
Diagnostic category |
ROM average% (range) |
Usual management |
|
Nondiagnostic |
13 (5–20) |
Repeat with ultrasound guidance |
|
Benign |
4 (2–7) |
Clinical and sonographic follow-up |
|
Atypia of Undetermined Significance |
22 (12–30) |
Repeat FNA, molecular testing, diagnostic lobectomy, or surveillance |
|
Follicular neoplasm |
30 (23–34) |
Molecular testing, diagnostic lobectomy |
|
Suspicious for Malignancy |
74 (67–83) |
Molecular testing, lobectomy, or near-total thyroidectomy |
|
Malignant |
97 (97–100) |
Lobectomy or near-total thyroidectomy |
