
كتاب
the Management of Ventral Hernia
- Annexes
Table 1. Primary ventral hernia classification, (17)
|
Primary ventral hernia classification |
Diameter (cm). |
|
Midline Epigastric Umbilical |
Small Medium Large < 2 cm 2 – 4 cm > 4 cm
|
|
Lateral Spigelian Lumbar |
|
Table 2. Incisional hernia classification, (17)
|
Midline Sub-xiphoid M1 Epigastric M2 Umbilical M3 Infra-umbilical M4 Suprapubic M5
|
|
Lateral Subcostal L1 Flank L2 Iliac L3 Lumbar L4 |
|
Recurrent incisional hernia Yes No |
|
Length (cm) |
|
Width (cm) < 4cm W1 4 - 10 cm W2 >4 cm W3
|
Table 3. Incisional hernia anatomical location borders, (17)
|
Borders of Borders of Midline area Lateral area ______________________________________________
Cranial Xiphoid process Costal margin Caudal Pubic bone Inguinal ligament Lateral Linea semilunaris Lumbar region Medial Linea semilunaris
|
Table 4. M and L zones for incisional hernia, (17)
|
Medial |
Lateral |
||||
|
M1 |
Sub-xiphoidal |
Xiphoid to 3 cm caudally |
L1 |
Subcostal |
Between the costal margin and a horizontal line 3 cm above the umbilicus |
|
M2 |
Epigastric |
3 cm below the xiphoid to 3 cm above the umbilicus |
L2 |
Flank |
Latera to the rectal sheath in the area 3 cm above and below the umbilicus |
|
M3 |
Umbilical |
3 cm above to 3 cm below the umbilicus |
L3 |
Iliac |
Between a horizontal line 3 cm below the umbilicus and the inguinal region |
|
M4 |
Infra-umbilical |
3 cm below the umbilicus To 3 cm above the pubis |
L4 |
Lumbar |
Latero dorsal to the anterior axillary line |
|
M5 |
Supra-pubic |
Pubic symphysis to 3 cm Cranially |
|
|
|
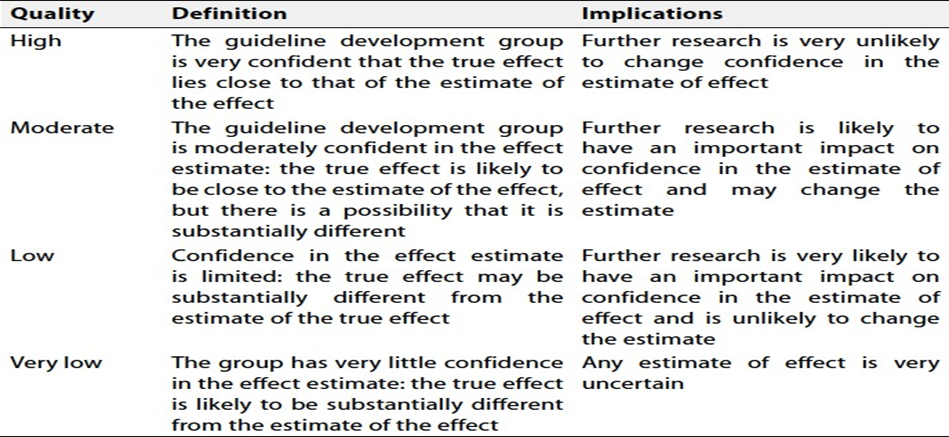
Table
5. Quality and Significance of the four levels of evidence in GRADE
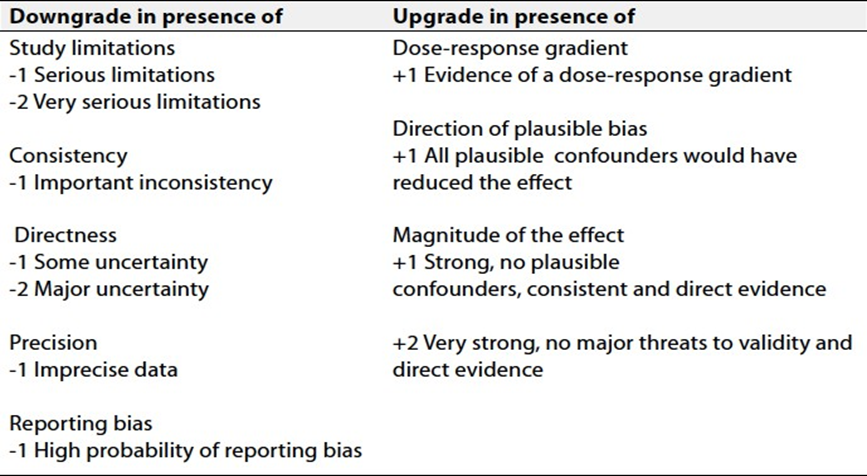
Table 6.
Factors that determine How to upgrade
or downgrade the quality of evidence
|
Table 7: Recommendations for mesh placed in the EXTRAPERITONEAL POSITION, (17). |
|
VHWG 2013 grade11 Risk Factors Recommended mesh Mesh to consider Contra-indicated mesh |
|
Low risk Composite, Biologic, Grade 1: Low risk No history of wound Plain mesh Fully absorbable PTFE infections Co-morbidities: Grade 2: Smoker, obese, Composite, Biologic, Intermediate risk diabetic, COPD, Plain mesh Fully absorbable PTFE previous wound infection Grade 3A Clean contaminated No mesh Plain Mesh*, Fully Composite, PTFE absorbable, Biologic Grade 3B Contaminated No mesh Fully absorbable, Composite, PTFE Biologic Grade 3C Dirty contaminated No mesh Fully absorbable Composite, Biologic, PTFE *It is recommended that if proceeding with a mesh repair after enterotomy, it should be large pore and placed in the retro-rectus position which is away from the peritoneal cavity and skin and is a well vascularized plane. |
