Book
LACRIMAL SYSTEM
- Dacryocystitis
It means inflammation of the lacrimal sac, canaliculi and nasolacrimal duct. Dacryocystitis usually is a concurrent with or sequelae to conjunctivitis.

Fig.7 : Dacryocystitis and secondary conjunctivitis in a horse. The conjunctivitis results from the failure of tear drainage as well as the reflux of tears from the obstructed and inflamed nasolacrimal sac.
Causes:
Viral, bacterial and mycotic infections are the most common causes. Cystic dilations of the nasolacrimal duct causing chronic dacryocystitis in dogs have been described
Symptoms:
1- Thick mucoid or mucopurulent discharge is present at the medial canthus.
2- Mucopurulent conjunctivitis is usually present.
3- Small swelling at the medial canthus is evident and painful to palpation. Digital pressure over this swelling may extrude a mucopurulent exudate.
4- In acute dacryocystitis, abscess may form and opens subcutaneously at the medial canthus. Fistula may develop connecting the sac with external skin.
5- Painful, erythematous dermatitis at the medial canthus in some cases.
6- History of recurrent unilateral conjunctivitis with temporary responses to topical antibiotics and attempted flushing.
DIAGNOSIS.
based on clinical signs, especially expression of purulent material from the puncta. The exact
site of the obstruction may be determined by cannulation, dacryocystorhinography, or magnetic resonance imaging.
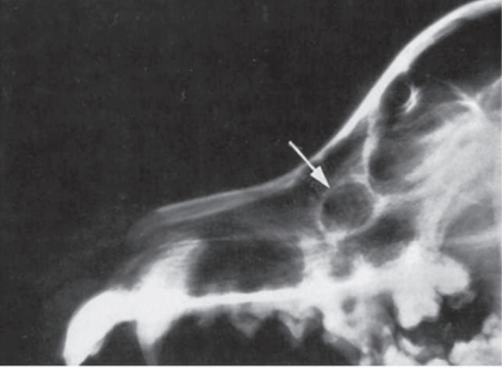
Fig.8: Lateral radiographic view of the skull of a 4-year-old golden retriever with recurrent intermittent episodes of purulent discharge from the right eye. A radiolucent area with sclerotic margins (arrow) is evident dorsal and rostral to the maxillary process of the maxillary bone (dorsal to the upper right fourth premolar). (Woerdt et al., 1997)
Treatment:
A- Medical treatment
By flushing and topical medication are effective in some cases, they are less reliable than catheterization and there is a greater chance of recurrence.
B- Surgical treatment
1- Catheterization and placement of retention tube which is left in place for 2 to 3 weeks. The inserted tubes rarely cause discomfort unless they become loose. For the first few days the uncannulated punctum may be flushed daily with a topical ophthalmic antibiotic solution, and topical antibiotic/corticosteroid solution is also applied to the ocular surface. If abscessation of the sac or severe dermatitis is present, systemic antibiotics are added.
2- Dacryocystotomy when the obstruction prevents the passage of a catheter.
|
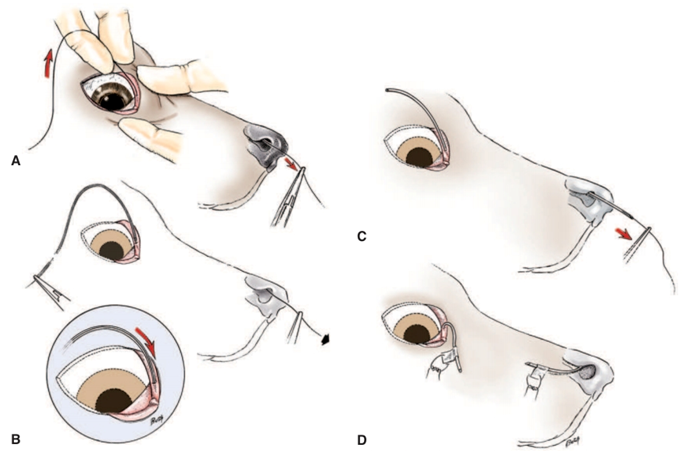
Fig.9: Indwelling nasolacrimal duct catheterization for correction of recurring obstruction: A, A monofilament nylon thread (2/0 with a smooth melted end) is passed via the superior punctum to emerge from the nose . B, Fine polyethylene (PE90), polyvinyl, or silicone tubing with a beveled end is passed over the thread. Halsted forceps are clamped behind the tubing, which is pulled from the nasal end by forceps on the thread. In horses, larger tubing is used. C, Care is taken as the tubing enters the punctum. Note: The inferior punctum may also be used if threading via this punctum was used. The tubing is pulled down the nasolacrimal duct, past any obstructions. D, The tube is sutured in place for 2 to 3 weeks. An Elizabethan collar should be considered to prevent the tubing from being dislodged. (Bistner et al.,1977) . |