
كتاب
LACRIMAL SYSTEM
- Keratoconjunctivitis sicca (KCS - Dry eye - Xerophthalmia)
- KCS is a disease involving the cornea and conjunctiva results from deficiency of the aqueous portion of the tear film. It is a common condition in dogs (The incidence of KCS in canine patients has been estimated at 1% Moore, 1999) and uncommon in cat and rare in other domestic animals.
- KCS is a common and important ocular disease in dogs. It should be suspected whenever chronic conjunctivitis, keratitis, or ocular discharge is present.

Fig. 14 : Early keratoconjunctivitis sicca (KCS) in a cat. Brown ocular discharge is present, the result of ocular surface inflammation KCS is commonly associated with feline herpesvirus (FHV1) infection in cats.
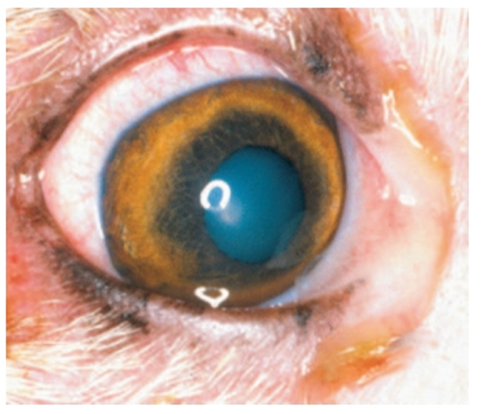
Fig.15: Mild keratoconjunctivitis sicca in a dog with a history of intermittent conjunctival hyperemia and discharge. At this stage tear production may wax and wane, and it is easy to misdiagnose the condition as intermittent conjunctivitis presumably of bacterial or allergic origin(David et al.,2008).

Fig.16: Severe keratoconjunctivitis sicca in an American cocker spaniel. Note the thick mucopurulent discharge that clings to the cornea, the hyperemia conjunctiva, and corneal roughening and pigmentation (David et al.,2008).
Causes:
1- Congenital absence of the lacrimal glands.
2- Spontaneous senile atrophy of the glands.
3- Lack of normal innervation of the glands. It may be due to traumatic causes, infection or spontaneously from unknown cause. This results in lack of lacrimal gland activity.
4- Trauma to the orbital and supra-orbital area damaging the lacrimal gland.
5- Surgical removal of the nictitans gland of the third eyelid.
6- Systemic disease, as canine distemper. The cause is a virus affecting the lacrimal and nictitans glands and may result in gland dysfunction.
7- Drug induced been associated with the nonsteroidal antiinflammatory drug (NSAID) , many sulfa derivatives, including trimethoprim sulfamethoxazole, sulfadiazine, and sulfasalazine. Sulfaderivative , with general anesthesia and topical or systemic atropine.Nutritional deficiencies as hypovitaminosis A.
8- Immune-Mediated. KCS in dogs is most often immunemediated.
9- Idiopathic causes; the majority of cases are of unknown cause.
Symptoms:
1- The clinical signs of KCS vary according to the degree of hyposecretion and the duration of the disease, also depending on whether the condition is bilateral or unilateral, acute or chronic and temporary or permanent.
2- Blepharospasm as a result of intense ocular pain and discomfort.
3- Mucoid and mucopurulent discharge. The eye and eyelids are covered with mucoid discharge. Change in the mucoid thread. As the tear production decreases, mucous production is increased as a protective mechanism for the eye resulting in increase in the size of mucous thread, change in its color into yellow green and becomes adherent to the conjunctiva.
4- Corneal changes include loss of luster, opacity, vascularization, pigmentation and keratinization.
5- Conjunctival changes. Conjunctiva becomes thick, dry and inflamed.
6- Nostrils may be normal or dry.
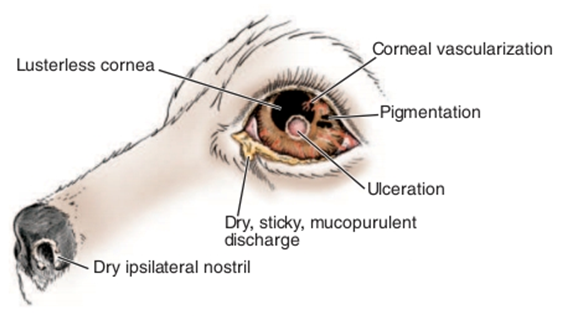
Fig.17: Clinical signs of keratoconjunctivitis sicca(David et al.,2008).
Diagnosis:
1- History of the case.
2- Clinical signs.
3- Schirmer’s tear test: The average normal tear wetting per minute is 20mm; suspicious levels are 5–10mm wetting per minute and most KCS patients exhibit wetting values less than 5mm per minute.
4- Rose-Bengal staining; 0.5% solution is instilled in the eye and the excess is flushed away with normal saline. Rose-Bengal stains the degenerated and devitalized corneo-conjunctival epithelium.
Treatment:
A) Medical Treatment:
1- Replacement of precorneal tear film by artificial tears as Methylcellulose 1%. Frequent instillation is essential.
2- Stimulation of lacrimal secretion by pilocarpine 1% solution, 1-4 drops added to the food.
3- Remove the excess of mucous by gentle and frequent washing and cleaning of the eyeball and eyelids with 5% acetylcysteine (mucomyst).
4- Control of infection by using broad spectrum antibiotics as chloramphenicol or gentamycin 4-6 times daily.
5- Anti-inflammatory agent as corticosteroids. It reduces conjunctival inflammation, conjunctival exudates, corneal vascularization and pigmentation.
B) Surgical treatment:
1- Surgical or cautery ablation of the lower punctum. This method is used to conserve the small amount of tears, if present. This technique has not been successful as KCS is usually absolute condition without any tear production.
2- Surgical reduction of the size of palpebral fissure through lateral tarsorrhaphy. Success of the procedure is dependent on some lacrimal activity.
3- Hydrophilic soft lenses applied to the cornea after application of medication to retains enough moisture and protect the cornea for several hours.
Parotid duct transportation: This operation is indicated when the medical treatment has been failed. A minimum of 3 months of medical treatment is desirable before starting surgical therapy as some dogs regain tear production during this time.
